You might also like
- The Code Stroke Handbook: Approach to the Acute Stroke PatientFrom EverandThe Code Stroke Handbook: Approach to the Acute Stroke PatientNo ratings yet
- Biomarkers For PDFDocument247 pagesBiomarkers For PDFBuga RazvanNo ratings yet
- Assessment Practices Cogn-Comm TBIDocument11 pagesAssessment Practices Cogn-Comm TBIRoisin McdonnellNo ratings yet
- RBANSDocument10 pagesRBANSFanel PutraNo ratings yet
- Management of Cerebral Edema, Brain Compression, and Intracranial PressureDocument29 pagesManagement of Cerebral Edema, Brain Compression, and Intracranial PressureNicolle Carrillo ForeroNo ratings yet
- ATLS 8th EditionDocument50 pagesATLS 8th EditionPaolo VegaNo ratings yet
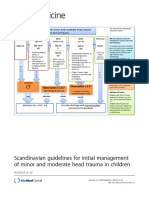
- Scandinavian Guidelines For Initial Management of Minor and Moderate Head Trauma in ChildrenDocument20 pagesScandinavian Guidelines For Initial Management of Minor and Moderate Head Trauma in ChildrenRafael Mujica OreNo ratings yet
- Research: CATCH: A Clinical Decision Rule For The Use of Computed Tomography in Children With Minor Head InjuryDocument8 pagesResearch: CATCH: A Clinical Decision Rule For The Use of Computed Tomography in Children With Minor Head InjuryCarlos Martin Yafac RiscoNo ratings yet
- Research Manuscript FinalDocument12 pagesResearch Manuscript FinalTHESSNAVARRONo ratings yet
- Subdural Hematoma in Adults - Prognosis and Management - UpToDate PDFDocument17 pagesSubdural Hematoma in Adults - Prognosis and Management - UpToDate PDFLinda RoldánNo ratings yet
- Assis 2017Document19 pagesAssis 2017widyadariNo ratings yet
- ISN KDIGO Early Screening Booklet PRINT UpdatedDocument14 pagesISN KDIGO Early Screening Booklet PRINT Updatedheba.barkasiehNo ratings yet
- CT Brain GuidelinesDocument6 pagesCT Brain GuidelinesMurali G RaoNo ratings yet
- ESCP CraniopharyngiomaDocument21 pagesESCP CraniopharyngiomaHermawan Pramudya IINo ratings yet
- 2020 Article 3403Document11 pages2020 Article 3403Gaetano De BiaseNo ratings yet
- NEJM JW TopGuidelineWatches 2013Document30 pagesNEJM JW TopGuidelineWatches 2013Hoàng TháiNo ratings yet
- 2022 Non-Cardiac SurgeryDocument105 pages2022 Non-Cardiac Surgeryhosameldin ahmedNo ratings yet
- Acute Stroke Intervention: The Heart of The Matter: SciencedirectDocument2 pagesAcute Stroke Intervention: The Heart of The Matter: SciencedirectMarianaPlataNo ratings yet
- FINAL Ranking Top 30 v2Document6 pagesFINAL Ranking Top 30 v2rajayasminNo ratings yet
- Management of Mild and Moderate Head Injuries in Adults: Dana Turliuc, A. CucuDocument11 pagesManagement of Mild and Moderate Head Injuries in Adults: Dana Turliuc, A. CucuSarrah Kusuma DewiNo ratings yet
- Neurosurgery 4 Mental DisordersDocument82 pagesNeurosurgery 4 Mental DisordersTomChristianNo ratings yet
- Minor Ped Head TraumaDocument25 pagesMinor Ped Head Traumalaila.forestaNo ratings yet
- MonitoreoicpnoinvasivoDocument7 pagesMonitoreoicpnoinvasivoCristianMP96No ratings yet
- Tuberous SclerosisDocument17 pagesTuberous SclerosiswardahkhattakNo ratings yet
- Int Forum Allergy Rhinol - 2018 - Mattos - Establishing The Minimal Clinically Important Difference For The QuestionnaireDocument6 pagesInt Forum Allergy Rhinol - 2018 - Mattos - Establishing The Minimal Clinically Important Difference For The QuestionnaireSid TNo ratings yet
- Slide Jurnal NeuroDocument16 pagesSlide Jurnal NeuroWilla MutiaNo ratings yet
- Diagnosis of Idiopathic Normal Pressure Hydrocephalus Is Supported by MRI-based Scheme: A Prospective Cohort StudyDocument11 pagesDiagnosis of Idiopathic Normal Pressure Hydrocephalus Is Supported by MRI-based Scheme: A Prospective Cohort StudyDini NanamiNo ratings yet
- Journal Bedah SarafDocument4 pagesJournal Bedah SarafWisnuardhyHendrawardhanaNo ratings yet
- CPG Management of Percutaneous Coronory Intervention (PCI) 2009Document92 pagesCPG Management of Percutaneous Coronory Intervention (PCI) 2009umiraihana1No ratings yet
- The Management and Outcome For Patients With Chronic Subdural Hematoma: A Prospective, Multicenter, Observational Cohort Study in The United KingdomDocument8 pagesThe Management and Outcome For Patients With Chronic Subdural Hematoma: A Prospective, Multicenter, Observational Cohort Study in The United KingdomRosario RosarioNo ratings yet
- NON CARDIAC SURGERY. ESC POCKET GLS.2022. Larger FontDocument63 pagesNON CARDIAC SURGERY. ESC POCKET GLS.2022. Larger FontGeoNo ratings yet
- Brain Death Scintigraphy V2.0 Final Draft For ApprovalDocument6 pagesBrain Death Scintigraphy V2.0 Final Draft For ApprovalLeticia PortilloNo ratings yet
- ESUR Guidelines On Contrast MediaDocument10 pagesESUR Guidelines On Contrast MediatsimitselisNo ratings yet
- Euro J of Neurology - 2017 - Ferro - European Stroke Organization Guideline For The Diagnosis and Treatment of CerebralDocument11 pagesEuro J of Neurology - 2017 - Ferro - European Stroke Organization Guideline For The Diagnosis and Treatment of CerebralIvan MihailovicNo ratings yet
- Gala TrialDocument11 pagesGala TrialRichard ZhuNo ratings yet
- Testing The Impact of Protocolized Care Of.5Document9 pagesTesting The Impact of Protocolized Care Of.5Nelson Da VegaNo ratings yet
- CPG Unstable AnginaDocument58 pagesCPG Unstable AnginaAmir HassenNo ratings yet
- Cancer de Pulmon Up To DateDocument197 pagesCancer de Pulmon Up To DateFernando HuertasNo ratings yet
- Which CT Features Help Predict Outcome After Head Injury?: PaperDocument5 pagesWhich CT Features Help Predict Outcome After Head Injury?: PaperLady KweeNo ratings yet
- STITCH Protocol 2011Document9 pagesSTITCH Protocol 2011Crhistian GarcíaNo ratings yet
- Outcomes of Prophylactic Cranial Irradiation in Patients With Small Cell Lung Cancer in The Modern Era of Baseline Magnetic Resonance Imaging of TheDocument9 pagesOutcomes of Prophylactic Cranial Irradiation in Patients With Small Cell Lung Cancer in The Modern Era of Baseline Magnetic Resonance Imaging of Theband pulmounandNo ratings yet
- 17.PLDD Vs Surgery RCTDocument9 pages17.PLDD Vs Surgery RCTBeata SviantickaNo ratings yet
- Jurnal CT ScanDocument9 pagesJurnal CT ScanPungki Putra TamaraNo ratings yet
- Clinical Neurology and Neurosurgery: SciencedirectDocument3 pagesClinical Neurology and Neurosurgery: SciencedirectGd SuarantaNo ratings yet
- 2018 Article 1048Document18 pages2018 Article 1048hectorNo ratings yet
- Chronic SDHDocument8 pagesChronic SDHAnonymous A9R0aLsNo ratings yet
- ClinKidneyJ 2015 Marcelli CKJ - Sfu145Document7 pagesClinKidneyJ 2015 Marcelli CKJ - Sfu145Bung HerryNo ratings yet
- Jurnal Syifa 4Document9 pagesJurnal Syifa 4cornelia cindy SRDNo ratings yet
- Rajajee - 2019 PDFDocument91 pagesRajajee - 2019 PDFAlexNo ratings yet
- Treggiari Miriam M Guidelines For The NeurocriticalDocument28 pagesTreggiari Miriam M Guidelines For The NeurocriticalBelén Fabbrizi100% (1)
- Drug-Eluting Stents: A Systematic Review and Economic EvaluationDocument6 pagesDrug-Eluting Stents: A Systematic Review and Economic EvaluationAleksandar CokanovicNo ratings yet
- Department of Brain Repair & RehabilitationDocument23 pagesDepartment of Brain Repair & Rehabilitationkuruvagadda sagarNo ratings yet
- Cerebral Oximetry Monitoring To Maintain Normal Cerebral ExplainDocument11 pagesCerebral Oximetry Monitoring To Maintain Normal Cerebral ExplainDaniel EllerNo ratings yet
- Jer 206 BBBDocument31 pagesJer 206 BBBVina SalsabilaNo ratings yet
- Journal 4 - Management of Traumatic Brain Injury A Narrative Review of Current EvidenceDocument11 pagesJournal 4 - Management of Traumatic Brain Injury A Narrative Review of Current EvidenceNatalindah Jokiem Woecandra T. D.No ratings yet
- 2023 Guideline Aneurysmal Subarachnoid HemorrhageDocument165 pages2023 Guideline Aneurysmal Subarachnoid Hemorrhagewmy6rf7nypNo ratings yet
- JofIMAB 2019 25 2p2471 2475Document5 pagesJofIMAB 2019 25 2p2471 2475afriskha bulawanNo ratings yet
- 2023 Guideline For The Management of Patients With Aneurysmal Subarachnoid Hemorrhage - A Guideline From The American Heart Association - American Stroke Association - StrokeDocument145 pages2023 Guideline For The Management of Patients With Aneurysmal Subarachnoid Hemorrhage - A Guideline From The American Heart Association - American Stroke Association - StrokeDaniel AraujoNo ratings yet
- Prehospital Stroke Care: New Prospects For Treatment and Clinical ResearchDocument8 pagesPrehospital Stroke Care: New Prospects For Treatment and Clinical ResearchmiriamneuroNo ratings yet
- 2004 Echo Standards PDFDocument25 pages2004 Echo Standards PDFMiki MarzukiNo ratings yet
- Stroke Nursing DissertationDocument4 pagesStroke Nursing DissertationBestCollegePaperWritingServiceCanada100% (1)
- Aneurysmal SAHDocument19 pagesAneurysmal SAHlakshminivas PingaliNo ratings yet
- ARTG - 2022 - Long-Term Outcomes of Patients With Primary Brain Tumors After Acute RehabilitationDocument11 pagesARTG - 2022 - Long-Term Outcomes of Patients With Primary Brain Tumors After Acute RehabilitationSM199021No ratings yet
- Computed-Tomography a Powerful Tool for Diagnosis of Pediatric and Adult Congenital Heart Disease: Methodology and Interpretation GuideFrom EverandComputed-Tomography a Powerful Tool for Diagnosis of Pediatric and Adult Congenital Heart Disease: Methodology and Interpretation GuideNo ratings yet
- State of the Art Techniques in Critical Care Echocardiography: 3D, Tissue, ContrastFrom EverandState of the Art Techniques in Critical Care Echocardiography: 3D, Tissue, ContrastKonstantin YastrebovNo ratings yet
- Daftar Kelulusan MCQSCBT Periode November 2018Document58 pagesDaftar Kelulusan MCQSCBT Periode November 2018larasNo ratings yet
- 3) Karakteristik Anak Yang Menderita Leukemia Akut Rawat Inap Di Rsup H. Adam Malik Medan Tahun 2011-2012 (Sulastriana)Document10 pages3) Karakteristik Anak Yang Menderita Leukemia Akut Rawat Inap Di Rsup H. Adam Malik Medan Tahun 2011-2012 (Sulastriana)Desy RusianaNo ratings yet
- TransDocument52 pagesTransDesy RusianaNo ratings yet
- 9) How I Treat Pediatric AML (Rubnitz JE)Document10 pages9) How I Treat Pediatric AML (Rubnitz JE)Desy RusianaNo ratings yet
- AML (Lymphoma Society)Document56 pagesAML (Lymphoma Society)Desy RusianaNo ratings yet
- Drugs PregnancyDocument9 pagesDrugs PregnancyPamelaS9No ratings yet
- End PointsDocument15 pagesEnd PointsDesy RusianaNo ratings yet
- Self-Induced Water Intoxication Treated With RisperidoneDocument3 pagesSelf-Induced Water Intoxication Treated With RisperidoneAlexi LaxiusNo ratings yet
- sglt2 InhibitorDocument6 pagessglt2 InhibitorDesy RusianaNo ratings yet
- Faril Elderly As Disaster Victims. Emergency Managment StrategiesDocument8 pagesFaril Elderly As Disaster Victims. Emergency Managment StrategiesJuliana SartoriNo ratings yet
- Diagnosis and Classification of Diabetes 2013Document8 pagesDiagnosis and Classification of Diabetes 2013Armando ATNo ratings yet
- sglt2 InhibitorDocument5 pagessglt2 InhibitorDesy RusianaNo ratings yet
- Effect of Heavy Metal On Malondialdehyde and Advanced Oxidation Protein Produtcs Concentration A Focus On Arsenic, Cadmium, and MercuryDocument6 pagesEffect of Heavy Metal On Malondialdehyde and Advanced Oxidation Protein Produtcs Concentration A Focus On Arsenic, Cadmium, and MercuryDesy RusianaNo ratings yet
- Effect of Heavy Metal On Malondialdehyde and Advanced Oxidation Protein Produtcs Concentration A Focus On Arsenic, Cadmium, and MercuryDocument6 pagesEffect of Heavy Metal On Malondialdehyde and Advanced Oxidation Protein Produtcs Concentration A Focus On Arsenic, Cadmium, and MercuryDesy RusianaNo ratings yet
- LyricsDocument29 pagesLyricsDesy RusianaNo ratings yet
- Long Term Sequelae From Childhood Pneumonia Systematic Review and Meta-AnalysisDocument9 pagesLong Term Sequelae From Childhood Pneumonia Systematic Review and Meta-AnalysisDesy RusianaNo ratings yet
- Ichard: Daftar PustakaDocument4 pagesIchard: Daftar PustakaDesy RusianaNo ratings yet
- AntithrombotikDocument18 pagesAntithrombotikDesy RusianaNo ratings yet
- Emerg Med J 2004 Wittenberg 429 32Document5 pagesEmerg Med J 2004 Wittenberg 429 32Desy RusianaNo ratings yet
- Ichard: Daftar PustakaDocument4 pagesIchard: Daftar PustakaDesy RusianaNo ratings yet
- Sims 3Document1 pageSims 3Desy RusianaNo ratings yet
- LyricsDocument29 pagesLyricsDesy RusianaNo ratings yet
- Ebook Development Infancy Through Adolescence 1St Edition Steinberg Test Bank Full Chapter PDFDocument61 pagesEbook Development Infancy Through Adolescence 1St Edition Steinberg Test Bank Full Chapter PDFbastmedalist8t2a100% (9)
- ATLS 10th Edition Update Summary - Banana Bag Blog - Emergency Medicine BlogDocument21 pagesATLS 10th Edition Update Summary - Banana Bag Blog - Emergency Medicine BlogapisaraearthNo ratings yet
- Color Trail TestDocument13 pagesColor Trail Testallexa726083100% (4)
- Classification of Trauma in Children - UpToDateDocument15 pagesClassification of Trauma in Children - UpToDateLeonardo Tavares de OliveiraNo ratings yet
- TCCC Handbook Fall 2013Document192 pagesTCCC Handbook Fall 2013AMG_IA100% (4)
- Airway and Ventilatory ManagementDocument19 pagesAirway and Ventilatory ManagementChynthea ParamithaNo ratings yet
- Prelims: - Intro To Calvarium and Head/brain Imaging Modalities - Craniofacial TraumaDocument97 pagesPrelims: - Intro To Calvarium and Head/brain Imaging Modalities - Craniofacial TraumaRica AriasNo ratings yet
- Epidemiology of Traumatic Brain Injury-Associated Epilepsy in WesternDocument7 pagesEpidemiology of Traumatic Brain Injury-Associated Epilepsy in Westernhermalina sabruNo ratings yet
- Polytrauma - Student's PresentationDocument24 pagesPolytrauma - Student's PresentationabdulazizNo ratings yet
- Trauma Care Manual-CRC Press Ian Greaves (Editor), Sir Keith Porter (Editor), Jeff Garner (Editor) - (2021)Document595 pagesTrauma Care Manual-CRC Press Ian Greaves (Editor), Sir Keith Porter (Editor), Jeff Garner (Editor) - (2021)Silvio danteNo ratings yet
- Occupational Therapy Assessment ToolsDocument19 pagesOccupational Therapy Assessment ToolsThirdy BullerNo ratings yet
- Raised ICP, SOL, HerniationDocument5 pagesRaised ICP, SOL, HerniationGrilled CroweNo ratings yet
- University of Cebu Lapu-Lapu and Mandaue: A.C. Cortes Ave., Looc, Mandaue, PhilippinesDocument12 pagesUniversity of Cebu Lapu-Lapu and Mandaue: A.C. Cortes Ave., Looc, Mandaue, PhilippinesZel ZozobradoNo ratings yet
- ConcussionsDocument3 pagesConcussionsKarlie CapozzoliNo ratings yet
- Subdural HematomaDocument5 pagesSubdural Hematomaluisse ann100% (1)
- Perfusion 1Document12 pagesPerfusion 1zixdiddyNo ratings yet
- Head Injury: Manali H. Solanki F.Y. M.Sc. Nursing J G College of NursingDocument31 pagesHead Injury: Manali H. Solanki F.Y. M.Sc. Nursing J G College of NursingWaqar AhmedNo ratings yet
- COT - June 2015 - Conference ProgrammeDocument42 pagesCOT - June 2015 - Conference ProgrammeBeccaNo ratings yet
- Early Outcomes of Assault Injuries Among Trauma Patients Presenting at Kampala International University Teaching Hospital and Jinja Regional Referral HospitalDocument11 pagesEarly Outcomes of Assault Injuries Among Trauma Patients Presenting at Kampala International University Teaching Hospital and Jinja Regional Referral HospitalKampala International UniversityNo ratings yet
- Gabbatore 2015Document15 pagesGabbatore 2015GsNo ratings yet
- Management of Acute Moderate and Severe Traumatic Brain InjuryDocument34 pagesManagement of Acute Moderate and Severe Traumatic Brain InjuryAndra MariaNo ratings yet
- Managing - Patients - With - Severe - Traumatic - Brain WITH HIGHLIGHTSDocument8 pagesManaging - Patients - With - Severe - Traumatic - Brain WITH HIGHLIGHTSTre OfficialNo ratings yet
- Perinatology Clinics 2008, Vol.35, Issues 4, Neuroprotection in The NewbornDocument210 pagesPerinatology Clinics 2008, Vol.35, Issues 4, Neuroprotection in The NewbornJhonny MarquezNo ratings yet
- WSES Consensus Conference Guidelines - TCEDocument9 pagesWSES Consensus Conference Guidelines - TCEDr. Victor Alonso Hernández HernándezNo ratings yet
- Prospectus: Auckland University of Technology, New ZealandDocument60 pagesProspectus: Auckland University of Technology, New ZealandPeram Amarnath 7147No ratings yet