You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Emergency Department Case Management: Second EditionDocument39 pagesEmergency Department Case Management: Second EditionsadikinNo ratings yet
- 125.6 (Medicine) DISCHARGE PLANDocument1 page125.6 (Medicine) DISCHARGE PLANNadja Jamilah100% (1)
- Sap Fi-Ar - DunningDocument18 pagesSap Fi-Ar - DunningDeepa Nagaraju100% (1)
- Homeopathic Remedy Pictures Alexander Gothe Julia Drinnenberg.04000 1Document6 pagesHomeopathic Remedy Pictures Alexander Gothe Julia Drinnenberg.04000 1BhargavaNo ratings yet
- Evaluation of Outpatient Department in A Public Super Speciality Hospital in IndiaDocument4 pagesEvaluation of Outpatient Department in A Public Super Speciality Hospital in IndiaMadhusudan MNo ratings yet
- BPC OverView 3Document1 pageBPC OverView 3Anil DuggalNo ratings yet
- Chemotherapy DrugsDocument1 pageChemotherapy DrugsAnil DuggalNo ratings yet
- PokerDocument1 pagePokerAnil DuggalNo ratings yet
- BPC Ove 13Document1 pageBPC Ove 13Anil DuggalNo ratings yet
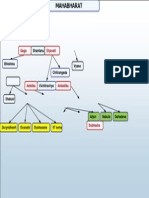
- Key Characters of the Mahabharat EpicDocument1 pageKey Characters of the Mahabharat EpicAnil DuggalNo ratings yet
- VirtualProvider: MultiProvider: InfoSet: Updates and AttributesDocument12 pagesVirtualProvider: MultiProvider: InfoSet: Updates and AttributesAnil DuggalNo ratings yet
- BPC OverView 3Document1 pageBPC OverView 3Anil DuggalNo ratings yet
- BPC OverView 3Document1 pageBPC OverView 3Anil DuggalNo ratings yet
- BPC OverView 3Document1 pageBPC OverView 3Anil DuggalNo ratings yet
- GAST1PJAN10Document1 pageGAST1PJAN10Anil DuggalNo ratings yet
- %%BPC OverViewDocument1 page%%BPC OverViewAnil DuggalNo ratings yet
- Gita SummaryDocument1 pageGita SummaryAnil DuggalNo ratings yet
- %%BPC OverViewDocument1 page%%BPC OverViewAnil DuggalNo ratings yet
- SAP Memory ManagementDocument11 pagesSAP Memory ManagementShobhit GargNo ratings yet
- GAST1PJAN10Document1 pageGAST1PJAN10Anil DuggalNo ratings yet
- RickettsiaDocument1 pageRickettsiaAnil DuggalNo ratings yet
- Bhagavad-Gita Summary: Krishna's Guidance to ArjunaDocument36 pagesBhagavad-Gita Summary: Krishna's Guidance to ArjunaAnil DuggalNo ratings yet
- Gita SummaryDocument1 pageGita SummaryAnil DuggalNo ratings yet
- $$AD GlossaryDocument10 pages$$AD GlossaryAnil DuggalNo ratings yet
- GradeSaver Bhagavad WithoutQuizDocument24 pagesGradeSaver Bhagavad WithoutQuizAnil DuggalNo ratings yet
- ChakraDocument7 pagesChakraAnil DuggalNo ratings yet
- GradeSaver Bhagavad WithoutQuizDocument24 pagesGradeSaver Bhagavad WithoutQuizAnil DuggalNo ratings yet
- Bhagavad-Gita Summary: Krishna's Guidance to ArjunaDocument36 pagesBhagavad-Gita Summary: Krishna's Guidance to ArjunaAnil DuggalNo ratings yet
- GradeSaver Bhagavad WithoutQuizDocument24 pagesGradeSaver Bhagavad WithoutQuizAnil DuggalNo ratings yet
- Bhagavad-Gita Quiz 1-4Document12 pagesBhagavad-Gita Quiz 1-4Anil DuggalNo ratings yet
- Bhagavad-Gita Quiz 1-4Document12 pagesBhagavad-Gita Quiz 1-4Anil DuggalNo ratings yet
- GradeSaver Bhagavad WithoutQuizDocument24 pagesGradeSaver Bhagavad WithoutQuizAnil DuggalNo ratings yet
- Bhagavad-Gita Summary: Krishna's Guidance to ArjunaDocument36 pagesBhagavad-Gita Summary: Krishna's Guidance to ArjunaAnil DuggalNo ratings yet
- WVSU Adult Nursing ProcessDocument9 pagesWVSU Adult Nursing ProcessMark ArconadaNo ratings yet
- Logbook GIDocument15 pagesLogbook GIAna BorodinaNo ratings yet
- Growing Demand for Home Dialysis in the UAEDocument6 pagesGrowing Demand for Home Dialysis in the UAEMuhammad Usman AsgherNo ratings yet
- Shalya Paper-I PDFDocument17 pagesShalya Paper-I PDFSusmita VinupamulaNo ratings yet
- Piis1470204520302722 PDFDocument2 pagesPiis1470204520302722 PDFkayegi8666No ratings yet
- Food Safety Case - The Fat Duck Norovirus Outbreak, UK - 2009Document16 pagesFood Safety Case - The Fat Duck Norovirus Outbreak, UK - 2009OPGJrNo ratings yet
- Foreword: OIE Terrestrial Manual 2008 IIIDocument8 pagesForeword: OIE Terrestrial Manual 2008 IIIWormInchNo ratings yet
- LUCAS Brochure 3303294 BDocument16 pagesLUCAS Brochure 3303294 BForum PompieriiNo ratings yet
- Managed Care, Hospitals' Hit Tolerable When Covid Emergency EndsDocument5 pagesManaged Care, Hospitals' Hit Tolerable When Covid Emergency EndsCarlos Mendoza DomínguezNo ratings yet
- Veinuino RiceDocument10 pagesVeinuino RiceAshley NacarNo ratings yet
- Periapical GranulomaDocument6 pagesPeriapical GranulomaEzza RiezaNo ratings yet
- Chronic Gastritis and Peptic Ulcer Disease GuideDocument32 pagesChronic Gastritis and Peptic Ulcer Disease GuideDian Ekawati100% (2)
- Chapter 9: Opinions On Professional Self-RegulationDocument27 pagesChapter 9: Opinions On Professional Self-RegulationSISIRA MOHANNo ratings yet
- Anaesthetic Considerations for Day Care SurgeryDocument8 pagesAnaesthetic Considerations for Day Care SurgerySirisha Ckv100% (1)
- Supreme Court Directs UP Govt to Stop Unqualified Medical PractitionersDocument12 pagesSupreme Court Directs UP Govt to Stop Unqualified Medical PractitionersShakshi MehtaNo ratings yet
- Dual Antiplatelet Therapy Vs Alteplase For Patients With Minor NondisablingDocument10 pagesDual Antiplatelet Therapy Vs Alteplase For Patients With Minor Nondisablingbetongo Bultus Ocultus XVNo ratings yet
- Aa 11Document5 pagesAa 11Eriekafebriayana RNo ratings yet
- Chemoregimen - Testicular CancerDocument2 pagesChemoregimen - Testicular CancerNanda Asyura RizkyaniNo ratings yet
- NUTR4320FINAL11Document10 pagesNUTR4320FINAL11rijzNo ratings yet
- Body temperature, vital signs, anthropometric measurementsDocument23 pagesBody temperature, vital signs, anthropometric measurementsWYNE BRENT M CORPUZNo ratings yet
- 4 . CVS 2023Document6 pages4 . CVS 2023Chipego NyirendaNo ratings yet
- USP of Revolution EVODocument2 pagesUSP of Revolution EVOStrategy AZ TeamNo ratings yet
- Rush University HCQDocument24 pagesRush University HCQJuana Atkins100% (1)
- Study Guide: MandatoryDocument21 pagesStudy Guide: Mandatoryyolanda fransiskaNo ratings yet
- Aesthetic Medicine Training CourseDocument8 pagesAesthetic Medicine Training Coursedrdahabra3No ratings yet
- RRL Caring TITLE: Impact of Nursing Care in The Nursing Profession ObjectivesDocument13 pagesRRL Caring TITLE: Impact of Nursing Care in The Nursing Profession ObjectivesroblesNo ratings yet