You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pdhpe Term 1 KindergratenDocument26 pagesPdhpe Term 1 Kindergratenapi-249015874No ratings yet
- MQ 63392Document130 pagesMQ 63392neeraj goyalNo ratings yet
- Psychology of Meditation by DR Siripala LeelaratnaDocument14 pagesPsychology of Meditation by DR Siripala LeelaratnaVisita LeelaratnaNo ratings yet
- Bangor University - EnglandDocument11 pagesBangor University - Englandmartinscribd7No ratings yet
- Presentation - Education in EmergenciesDocument31 pagesPresentation - Education in EmergenciesCharlie ViadoNo ratings yet
- Personnel Planning and RecruitmentDocument17 pagesPersonnel Planning and RecruitmentPiper FaustusNo ratings yet
- Assignment Form 2Document3 pagesAssignment Form 2api-290458252No ratings yet
- 2006-2007 CUNY Law Admin GoalsDocument7 pages2006-2007 CUNY Law Admin GoalscunylawblogNo ratings yet
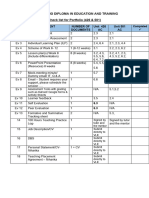
- Checklist For Portfolio Evidence (426 & 501) (Final)Document1 pageChecklist For Portfolio Evidence (426 & 501) (Final)undan.uk3234No ratings yet
- Computer Applications in ChemistryDocument16 pagesComputer Applications in ChemistryGanesh NNo ratings yet
- IE468 Multi Criteria Decision MakingDocument2 pagesIE468 Multi Criteria Decision MakingloshidhNo ratings yet
- Ethical Issues in The Health Care of OlderDocument14 pagesEthical Issues in The Health Care of Olderedward osae-oppongNo ratings yet
- Question Bank: Student Check-Ins: 80 Questions Across Well-Being, SEL Skills, Relationships, and Classroom FeedbackDocument15 pagesQuestion Bank: Student Check-Ins: 80 Questions Across Well-Being, SEL Skills, Relationships, and Classroom FeedbackTemporary 241No ratings yet
- CCE-English PrimaryDocument69 pagesCCE-English PrimaryShanthi Meena Kumari63% (8)
- Regional Ecology Center (REC) GuidelinesDocument48 pagesRegional Ecology Center (REC) GuidelinesKarlou BorjaNo ratings yet
- Knowledge: Skills: Attitude: ValuesDocument3 pagesKnowledge: Skills: Attitude: ValuesVincent Paul TepaitNo ratings yet
- CMV RulesDocument174 pagesCMV Rulessunithascribd100% (1)
- Pinpdf Com 91 Colour Prediction Trick 91 ClubDocument3 pagesPinpdf Com 91 Colour Prediction Trick 91 Clubsaimkhan8871340% (1)
- Personal Development: High School Department Culminating Performance TaskDocument3 pagesPersonal Development: High School Department Culminating Performance TaskLLYSTER VON CLYDE SUMODEBILANo ratings yet
- Curriculum Map - Math8Document5 pagesCurriculum Map - Math8api-242927075No ratings yet
- Curriculum and Materials CbliDocument9 pagesCurriculum and Materials CbliNAZIRA SANTIAGO ESCAMILLANo ratings yet
- Edval - Good Moral and Right Conduct: Personhood DevelopmentDocument9 pagesEdval - Good Moral and Right Conduct: Personhood DevelopmentSophia EspañolNo ratings yet
- TOSSCIENCE12Document2 pagesTOSSCIENCE12Xyrix GapasinNo ratings yet
- Amsterdam University College: Application Guidelines 2021-2022Document16 pagesAmsterdam University College: Application Guidelines 2021-2022Vinod TanwaniNo ratings yet
- A Crash Course in Media LiteracyDocument4 pagesA Crash Course in Media LiteracyAkan D YazganNo ratings yet
- NBC September 2023 Poll For Release 92423Document24 pagesNBC September 2023 Poll For Release 92423Veronica SilveriNo ratings yet
- EAPP DebateDocument3 pagesEAPP DebateAyessa JordanNo ratings yet
- Evidence Law Reading ListDocument9 pagesEvidence Law Reading ListaronyuNo ratings yet
- Module 5 Curriculum ImplementationDocument38 pagesModule 5 Curriculum ImplementationRen Ren100% (5)
- UWTSD BABS 5 ENT SBLC6001 Assignment and Case Study Apr-Jul 2019Document16 pagesUWTSD BABS 5 ENT SBLC6001 Assignment and Case Study Apr-Jul 2019Hafsa IqbalNo ratings yet