You might also like
- Agreement To Care For and Return Company EquipmentDocument1 pageAgreement To Care For and Return Company EquipmentUbuntu Linux100% (2)
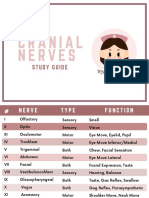
- Cranial NervesDocument6 pagesCranial Nervesvienny kayeNo ratings yet
- KM Ebook 15FatLossStrategiesDocument18 pagesKM Ebook 15FatLossStrategiesfoof faafNo ratings yet
- On The Charge of Rape: Under Article 266-A of The RPC, Rape IsDocument3 pagesOn The Charge of Rape: Under Article 266-A of The RPC, Rape IsTricia SandovalNo ratings yet
- Nursing Health Assessment: Akram Mohammad Abusalah BNS, MSN, Ph. D. Islamic University of Gaza StripDocument262 pagesNursing Health Assessment: Akram Mohammad Abusalah BNS, MSN, Ph. D. Islamic University of Gaza StripBheru LalNo ratings yet
- AdpieDocument11 pagesAdpieChucky Vergara0% (1)
- Madeleine LeiningerDocument15 pagesMadeleine LeiningerYolanda SPNo ratings yet
- Evaluating Health Education PlanDocument5 pagesEvaluating Health Education PlanPerly joy SeguraNo ratings yet
- Maternal Health ServicesDocument24 pagesMaternal Health ServicesMuna Hassan MustafaNo ratings yet
- Presentation On Community Health Nursing Intoduction, Definitions, Aims, Philosophy and Roles of Community Health NurseDocument20 pagesPresentation On Community Health Nursing Intoduction, Definitions, Aims, Philosophy and Roles of Community Health Nursekuruvagadda sagarNo ratings yet
- Orem TheoryDocument34 pagesOrem TheoryTerefe KetoNo ratings yet
- Florence Nightingale-Modern NursingDocument25 pagesFlorence Nightingale-Modern NursingRanah Julia Garchitorena Ayo100% (1)
- Health Belief ModelDocument8 pagesHealth Belief ModelRUIZ JAKE CANCILLER. VELARDENo ratings yet
- Case Study Mr. MDocument8 pagesCase Study Mr. MBettNo ratings yet
- Home Visit PDFDocument18 pagesHome Visit PDFSaad AlkhathamiNo ratings yet
- Health Belief ModelDocument5 pagesHealth Belief ModelKasem AhmedNo ratings yet
- Chapter 1 - Introduction To Nursing ResearchDocument5 pagesChapter 1 - Introduction To Nursing ResearchKathrina Ioannou100% (3)
- Mental Health Nursing Case Study - CompleteDocument12 pagesMental Health Nursing Case Study - Completeapi-546486919No ratings yet
- Cultural Diversity in Nursing PracticeDocument3 pagesCultural Diversity in Nursing PracticeEli Xma100% (2)
- 1-Significance and Purposes of Nursing ResearchDocument22 pages1-Significance and Purposes of Nursing ResearchPrincess Ivan Gayagoy100% (1)
- Process RecordingDocument6 pagesProcess RecordingteuuuuNo ratings yet
- The Battle Against Covid-19 Filipino American Healthcare Workers on the Frontlines of the Pandemic ResponseFrom EverandThe Battle Against Covid-19 Filipino American Healthcare Workers on the Frontlines of the Pandemic ResponseNo ratings yet
- Acute Gastro Enteritis 1Document42 pagesAcute Gastro Enteritis 1MichaelKimDugenia0% (1)
- Family Case Study FinalDocument39 pagesFamily Case Study Final2AVALOROSO, Grace Divine B.No ratings yet
- Example Health Promotion Teaching PlanDocument6 pagesExample Health Promotion Teaching PlanfaizaNo ratings yet
- Role of Community Health Nurses in Sustainable Development Goals in Good Health and Well BeingDocument14 pagesRole of Community Health Nurses in Sustainable Development Goals in Good Health and Well BeingLoi CrespoNo ratings yet
- Angeles University Foundation: CholelithiasisDocument1 pageAngeles University Foundation: CholelithiasisKate Laxamana GuinaNo ratings yet
- Clinical PracticumDocument57 pagesClinical Practicumapi-27446294No ratings yet
- Functional Health PatternsDocument6 pagesFunctional Health PatternsBrianne SheldonNo ratings yet
- Nola PenderDocument26 pagesNola PenderNoel S.BernalNo ratings yet
- Scope of Community Health Nursing PracticeDocument2 pagesScope of Community Health Nursing Practicechuniadsuar50% (2)
- Care of Older Persons With Dementia and DepressionDocument28 pagesCare of Older Persons With Dementia and DepressionAnthony RiggsNo ratings yet
- Villarin Alessandro N40 TMA1Document15 pagesVillarin Alessandro N40 TMA1Zhiela Esteban AbivaNo ratings yet
- Professional Nursing Case Study TemplateDocument3 pagesProfessional Nursing Case Study TemplateShane Aileen AngelesNo ratings yet
- GORDON Manuscript For CPDocument7 pagesGORDON Manuscript For CPStephNo ratings yet
- Process Recording 1Document7 pagesProcess Recording 1api-314099202No ratings yet
- 10 Aschool Health PRGRM DoneDocument166 pages10 Aschool Health PRGRM DoneHarshitha100% (1)
- Principles of Health EducationDocument7 pagesPrinciples of Health EducationSonu SubbaNo ratings yet
- Appendectomy Case Presentation of JaysonDocument20 pagesAppendectomy Case Presentation of JaysonJaysonPangilinanAban100% (1)
- Syndicated Seminar ProposalDocument44 pagesSyndicated Seminar ProposalBeanncaAngelesNo ratings yet
- Pneumonia Case StudyDocument3 pagesPneumonia Case StudyKayla Callahan50% (2)
- Review of Related Literature and Studies: EducationDocument19 pagesReview of Related Literature and Studies: EducationKatherine 'Chingboo' Leonico LaudNo ratings yet
- Teaching Plan On DMDocument2 pagesTeaching Plan On DMdiane_mananganNo ratings yet
- Abdellah's TheoryDocument14 pagesAbdellah's Theoryanon_387100722100% (1)
- CHN Process NotesDocument9 pagesCHN Process NotesJohn Lawrence YbanezNo ratings yet
- MH Nursing Clinical Case StudyDocument10 pagesMH Nursing Clinical Case Studyapi-546041293No ratings yet
- Teaching Competency of Nursing Educators and Caring Attitude of Nursing StudentsDocument26 pagesTeaching Competency of Nursing Educators and Caring Attitude of Nursing StudentsJaine NicolleNo ratings yet
- Nurse Case StudyDocument6 pagesNurse Case Studyprateeksha16No ratings yet
- Nursing Informatics 1Document5 pagesNursing Informatics 1Elonna Anne100% (1)
- Mental Retardation Treatment and ManagementDocument12 pagesMental Retardation Treatment and ManagementMelchoniza CalagoNo ratings yet
- 104-3 Journaling EssayDocument6 pages104-3 Journaling Essayapi-288504264No ratings yet
- Reflective ExemplarDocument2 pagesReflective Exemplarapi-531834240No ratings yet
- Lydia HallDocument23 pagesLydia HallJeah Jacob100% (1)
- Leisure and Its Impact On Well Being in School ChildrenDocument1 pageLeisure and Its Impact On Well Being in School Childrenesinu27No ratings yet
- Comprehensive Study of Paranoid Schizophrenia: Submitted byDocument39 pagesComprehensive Study of Paranoid Schizophrenia: Submitted byPatricia Lingad RNNo ratings yet
- Comprehensive School Health AssessmentDocument8 pagesComprehensive School Health Assessmentapi-308397176No ratings yet
- ThesisDocument11 pagesThesismae santosNo ratings yet
- Health Promotion ModelDocument2 pagesHealth Promotion ModelpatrickarvinNo ratings yet
- Psychiatric Mental Health Case StudyDocument11 pagesPsychiatric Mental Health Case Studyapi-402701741100% (1)
- Nationnal Adult Health ProgrammesDocument12 pagesNationnal Adult Health Programmesdevyani meshramNo ratings yet
- Process Recording, Suicide Assesment and Psyche-Med ConditionDocument44 pagesProcess Recording, Suicide Assesment and Psyche-Med ConditionShy Dela PuertaNo ratings yet
- Application - of - Theory - in - NursingDocument9 pagesApplication - of - Theory - in - Nursingako at ang exo100% (1)
- Nurse Patient Relationship Research PaperDocument11 pagesNurse Patient Relationship Research PaperLen ZinxNo ratings yet
- Form 1 Nutrition in Animals A Teacher - Co .KeDocument6 pagesForm 1 Nutrition in Animals A Teacher - Co .Kelydiaciru01No ratings yet
- Guide in Filling Up The Competency Assessment FormDocument5 pagesGuide in Filling Up The Competency Assessment FormJOSEPH CAJOTENo ratings yet
- Micro InsuranceDocument27 pagesMicro Insurancedrishya3No ratings yet
- US8236919Document4 pagesUS8236919Billy FowlerNo ratings yet
- People in OrganisationsDocument8 pagesPeople in OrganisationsBritney valladares100% (1)
- Reference Texts - Textes de RéférenceDocument7 pagesReference Texts - Textes de RéférenceSid PatelNo ratings yet
- Red Oxide PrimerDocument2 pagesRed Oxide Primermarsha.fsdNo ratings yet
- Digital Voltmeter (DVM) : Elementary Measurement SystemDocument4 pagesDigital Voltmeter (DVM) : Elementary Measurement SystemRounakNo ratings yet
- Autopsy Case For HEMODYNAMIC DISORDERS PDFDocument8 pagesAutopsy Case For HEMODYNAMIC DISORDERS PDFpixiedustNo ratings yet
- Resume - Shady Brook Assistant PrincipalDocument1 pageResume - Shady Brook Assistant Principalapi-359951158No ratings yet
- Treatment Plan 3Document8 pagesTreatment Plan 3Kathy Lee Hornbeck KendrickNo ratings yet
- Group Mediclaim Tailormade - Endorsement ScheduleDocument2 pagesGroup Mediclaim Tailormade - Endorsement ScheduleSneha SinghNo ratings yet
- PENC N BONDIDocument5 pagesPENC N BONDIYLND100% (1)
- Brammer Standard Company, Inc.: Bs Su LAS-14Document3 pagesBrammer Standard Company, Inc.: Bs Su LAS-14Ali MohsinNo ratings yet
- Summary of Cutting Data For Plain Surface: DegrosareDocument4 pagesSummary of Cutting Data For Plain Surface: DegrosareAndrei MihaiNo ratings yet
- WinesDocument15 pagesWinesRose ann rodriguezNo ratings yet
- Rebar Cutting List SampleDocument7 pagesRebar Cutting List SampleAndrea MagtutoNo ratings yet
- MotherDocument11 pagesMotherMuhammad Lucky AlfaridzyNo ratings yet
- Lecture 06 What Is Avalanche and Causes of Avalanche CSS PMS General Science and AbilityDocument13 pagesLecture 06 What Is Avalanche and Causes of Avalanche CSS PMS General Science and Abilityabdul samiNo ratings yet
- Lost Youth Assignment-2Document2 pagesLost Youth Assignment-2api-363462333No ratings yet
- PSC Solar Uk Xantra Inverter With Avr User ManualDocument11 pagesPSC Solar Uk Xantra Inverter With Avr User Manualnwizu100% (1)
- Unit 11 - Late AdulthoodDocument14 pagesUnit 11 - Late AdulthoodEvet VaxbmNo ratings yet
- Problem Set 4 SolutionDocument16 pagesProblem Set 4 SolutionJana PaduaNo ratings yet
- Toilet PPR Pipe & FittingDocument4 pagesToilet PPR Pipe & FittingFaysal ahmedNo ratings yet
- Presence of Oxalative Ions in GuavaDocument12 pagesPresence of Oxalative Ions in GuavapozozgamingNo ratings yet
- PPLS Seri A Februari 2020 PDFDocument33 pagesPPLS Seri A Februari 2020 PDFhedriansyah edNo ratings yet