You might also like
- EEG Brain Signal Classification for Epileptic Seizure Disorder DetectionFrom EverandEEG Brain Signal Classification for Epileptic Seizure Disorder DetectionNo ratings yet
- Query Processing inDocument10 pagesQuery Processing inAnita Sofia KeyserNo ratings yet
- Classification of Heart Disease Dataset Using Multilayer Feed Forward Backpropogation AlgorithmDocument7 pagesClassification of Heart Disease Dataset Using Multilayer Feed Forward Backpropogation AlgorithmInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- EEG Based Authentication Using Binary CLDocument13 pagesEEG Based Authentication Using Binary CLRazan AlNo ratings yet
- Automated Anomaly and Root Cause Detection in Distributed SystemsDocument6 pagesAutomated Anomaly and Root Cause Detection in Distributed Systemssurendiran123No ratings yet
- Paper5 LibreDocument4 pagesPaper5 LibreKarthik KihtrakNo ratings yet
- A Thin Client Interface To A High Performance Multi-Modal Image Analytics SystemDocument8 pagesA Thin Client Interface To A High Performance Multi-Modal Image Analytics SystemLeonardo Lozano-RojasNo ratings yet
- Efficient Use of Hybrid Adaptive Neuro-Fuzzy Inference System Combined With Nonlinear Dimension Reduction Method in Production ProcessesDocument15 pagesEfficient Use of Hybrid Adaptive Neuro-Fuzzy Inference System Combined With Nonlinear Dimension Reduction Method in Production ProcessesCS & ITNo ratings yet
- SSRN Id3668220Document13 pagesSSRN Id3668220Minh VươngNo ratings yet
- Real-Time Activity Recognition System Using Motion and Physiological SensorsDocument4 pagesReal-Time Activity Recognition System Using Motion and Physiological SensorsonigasNo ratings yet
- Virtual Instrumentation Interface For SRRC Control System: The Is AsDocument3 pagesVirtual Instrumentation Interface For SRRC Control System: The Is AsJulio CésarNo ratings yet
- Hot Gas Path Management Control Level (Part 27)Document4 pagesHot Gas Path Management Control Level (Part 27)Gasser ElfahamNo ratings yet
- Fault Detection System For Centrifugal Pumps Using Neural Networks and Neuro-Fuzzy TechniquesDocument9 pagesFault Detection System For Centrifugal Pumps Using Neural Networks and Neuro-Fuzzy TechniquesTetria AdwineldaNo ratings yet
- Define The ProblemDocument10 pagesDefine The ProblemmohammedelshafieNo ratings yet
- Human Activities Classifier Using SVMDocument19 pagesHuman Activities Classifier Using SVMBsef19m012-IQRA SARWARNo ratings yet
- Application of Artificial Neural Network (ANN) Technique For The Measurement of Voltage Stability Using FACTS Controllers - ITDocument14 pagesApplication of Artificial Neural Network (ANN) Technique For The Measurement of Voltage Stability Using FACTS Controllers - ITpradeep9007879No ratings yet
- Energy Saving in P2P Oriented Wireless Sensor Network (WSN) Using The Approach of Various Compression TechniquesDocument4 pagesEnergy Saving in P2P Oriented Wireless Sensor Network (WSN) Using The Approach of Various Compression TechniquesInternational Organization of Scientific Research (IOSR)No ratings yet
- Automated Substation Monitoring System Requirements & EvaluationDocument11 pagesAutomated Substation Monitoring System Requirements & Evaluationpvenky_kkdNo ratings yet
- PythonHeartDisease-FirstReviewDocument4 pagesPythonHeartDisease-FirstReviewMeenachi SundaramNo ratings yet
- Multi-Layer PerceptronsDocument8 pagesMulti-Layer PerceptronswarrengauciNo ratings yet
- MLP ReportDocument4 pagesMLP Reporthxrxr880No ratings yet
- A Novel Web Based Expert System Architecture For On-Line and Off-Line Fault Diagnosis and Control (FDC) of TransformersDocument5 pagesA Novel Web Based Expert System Architecture For On-Line and Off-Line Fault Diagnosis and Control (FDC) of TransformersVickyNo ratings yet
- Use of AANN For Signal ValidationDocument11 pagesUse of AANN For Signal ValidationSohom DattaNo ratings yet
- Wireless Medical-Embedded Systems: A Review of Signal-Processing Techniques For ClassificationDocument15 pagesWireless Medical-Embedded Systems: A Review of Signal-Processing Techniques For Classificationsanketh07No ratings yet
- Eye Disease Classification - Teksun Inc.Document24 pagesEye Disease Classification - Teksun Inc.Yash AminNo ratings yet
- Using A Neural Network in The Software Testing Process: International Journal of Intelligent Systems January 2002Document18 pagesUsing A Neural Network in The Software Testing Process: International Journal of Intelligent Systems January 2002asaNo ratings yet
- Literature ReviewDocument18 pagesLiterature Reviewrahul mishraNo ratings yet
- Rajeev Insttitute of Technology: Dept. of Electronics & Communication EngineeringDocument18 pagesRajeev Insttitute of Technology: Dept. of Electronics & Communication EngineeringSharadhiNo ratings yet
- Evaluacion InstrumentacionDocument5 pagesEvaluacion InstrumentacionCamila SarabiaNo ratings yet
- A 1 TOPS - W Analog Deep Machine-Learning Engine With Floating-Gate Storage in 0.13 Μm CMOSDocument12 pagesA 1 TOPS - W Analog Deep Machine-Learning Engine With Floating-Gate Storage in 0.13 Μm CMOSKjfsa TuNo ratings yet
- Medical Data Mining with WEKADocument4 pagesMedical Data Mining with WEKAShafayet UddinNo ratings yet
- Configurable Data LoogerDocument4 pagesConfigurable Data LoogerKen IdanwekhaiNo ratings yet
- DOTNET PROJECTSDocument12 pagesDOTNET PROJECTSreaderjsNo ratings yet
- Sensors 07Document21 pagesSensors 07mzdeqNo ratings yet
- Artificial Neural Network Approach For Classification of Heart Disease DatasetDocument5 pagesArtificial Neural Network Approach For Classification of Heart Disease DatasetInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Applications of Neural Networks in Data Mining: M.Charles ArockiarajDocument4 pagesApplications of Neural Networks in Data Mining: M.Charles ArockiarajresearchinventyNo ratings yet
- Neural Networks Embed DDocument6 pagesNeural Networks Embed DL S Narasimharao PothanaNo ratings yet
- In Particular, Herein We Deal With Those Related To Telediagnosis Through Multiple-Lead Electrocardiographic SignalsDocument17 pagesIn Particular, Herein We Deal With Those Related To Telediagnosis Through Multiple-Lead Electrocardiographic SignalsRoberto Bob BrunéNo ratings yet
- Research Projects - Dr. B.R. UpadhyayaDocument3 pagesResearch Projects - Dr. B.R. UpadhyayaprabuNo ratings yet
- Vulnerability Assessment of A Large Sized Power System Using Neural Network Considering Various Feature Extraction MethodsDocument10 pagesVulnerability Assessment of A Large Sized Power System Using Neural Network Considering Various Feature Extraction MethodsMarysol AyalaNo ratings yet
- Designing A Neural Network For Forecasting Financial and Economic Time SerieDocument22 pagesDesigning A Neural Network For Forecasting Financial and Economic Time SerieFaisal KhalilNo ratings yet
- Real-Time Gesture Mapping in PD Environment Using Neural NetworksDocument4 pagesReal-Time Gesture Mapping in PD Environment Using Neural NetworkslupustarNo ratings yet
- Nero Solution Litreture From HelpDocument6 pagesNero Solution Litreture From Helpvijay_dhawaleNo ratings yet
- Artificial Neural Networks for Intrusion DetectionDocument5 pagesArtificial Neural Networks for Intrusion Detections.pawar.19914262No ratings yet
- Dissertation On Wireless Sensor NetworkDocument4 pagesDissertation On Wireless Sensor NetworkDoMyPaperForMoneyDesMoines100% (1)
- AI Agents at Different Data Centers of A Specific Company To Minimize The Energy Spending ModulesDocument3 pagesAI Agents at Different Data Centers of A Specific Company To Minimize The Energy Spending Moduleshumritha kNo ratings yet
- IoT-Based EHealth Data Acquisition SystemDocument5 pagesIoT-Based EHealth Data Acquisition SystemBHARAT RAJ GeddamNo ratings yet
- Efficient Comparison Based Self Diagnosis Using Backpropagation Artificial Neural NetworksDocument6 pagesEfficient Comparison Based Self Diagnosis Using Backpropagation Artificial Neural Networkssri248No ratings yet
- Data Acquisition System of 16-Channel EEG Based On ATSAM3X8E ARM Cortex-M3 32-Bit Microcontroller and ADS1299Document7 pagesData Acquisition System of 16-Channel EEG Based On ATSAM3X8E ARM Cortex-M3 32-Bit Microcontroller and ADS1299tony starkNo ratings yet
- Information Extraction From Sensor Networks Using The Watershed Transform AlgorithmDocument11 pagesInformation Extraction From Sensor Networks Using The Watershed Transform Algorithm- -No ratings yet
- NETEXTRACT - Extracting Belief Networks in Telecommunications DataDocument9 pagesNETEXTRACT - Extracting Belief Networks in Telecommunications Datansantos5847No ratings yet
- Estimation of Difficult-to-Measure Process Variables Using Neural NetworksDocument4 pagesEstimation of Difficult-to-Measure Process Variables Using Neural NetworksWalid AbidNo ratings yet
- First PaperDocument4 pagesFirst Paperachaparala4499No ratings yet
- Journal Pre-Proof: Microprocessors and MicrosystemsDocument29 pagesJournal Pre-Proof: Microprocessors and MicrosystemsarjetaNo ratings yet
- Practical File Cloud Computing IT-704Document27 pagesPractical File Cloud Computing IT-704Vikas DandotiyaNo ratings yet
- Ann Case StudyDocument14 pagesAnn Case StudysuryaysNo ratings yet
- Improved Data Discrimination in Wireless Sensor Networks: B. A. Sabarish, S. ShanmugapriyaDocument3 pagesImproved Data Discrimination in Wireless Sensor Networks: B. A. Sabarish, S. Shanmugapriyamurthy_siri22No ratings yet
- Stock Value Prediction SystemDocument3 pagesStock Value Prediction SystemEditor IJRITCCNo ratings yet
- Wireless Sensor Networks Research Papers 2014Document8 pagesWireless Sensor Networks Research Papers 2014afedetbma100% (1)
- AWP Lecture Notes-FinalDocument110 pagesAWP Lecture Notes-FinalgopichandNo ratings yet
- Random Thoughts - . .: The Ten Worst Teaching MistakesDocument2 pagesRandom Thoughts - . .: The Ten Worst Teaching MistakesfamtaluNo ratings yet
- Abet Paper (Jee)Document7 pagesAbet Paper (Jee)famtaluNo ratings yet
- Antenna NoiseDocument11 pagesAntenna NoiseRashid BhattiNo ratings yet
- Relationship of FIR and IIR filtersDocument5 pagesRelationship of FIR and IIR filtersfamtaluNo ratings yet
- Blending Engineering Modeling, Industrial Design, Thesis-46972722-MIT PDFDocument71 pagesBlending Engineering Modeling, Industrial Design, Thesis-46972722-MIT PDFfamtaluNo ratings yet
- Abet Paper (Jee)Document19 pagesAbet Paper (Jee)MohsenMahroosNo ratings yet
- Forcesofnaturepo00guilrich PDFDocument750 pagesForcesofnaturepo00guilrich PDFfamtaluNo ratings yet
- C/OS-II Reference Manual: #DefineDocument128 pagesC/OS-II Reference Manual: #DefineVramesh4545No ratings yet
- Creativity in Engineering Education: Richard M. Felder North Carolina State UniversityDocument7 pagesCreativity in Engineering Education: Richard M. Felder North Carolina State UniversityfamtaluNo ratings yet
- Random Thoughts - . .: The Ten Worst Teaching MistakesDocument2 pagesRandom Thoughts - . .: The Ten Worst Teaching MistakesfamtaluNo ratings yet
- FM Mod DemodDocument21 pagesFM Mod DemodOsama Abou ZaidNo ratings yet
- Top Ten Skills in 2020 PDFDocument4 pagesTop Ten Skills in 2020 PDFfamtaluNo ratings yet
- Learning and Teaching StylesDocument10 pagesLearning and Teaching StylesCiobaniuc AdinaNo ratings yet
- Learning by DoingDocument2 pagesLearning by DoingRicardoCostaNo ratings yet
- Learning and Teaching StylesDocument10 pagesLearning and Teaching StylesCiobaniuc AdinaNo ratings yet
- Led ckt-1Document37 pagesLed ckt-1famtaluNo ratings yet
- Abet Paper (Jee)Document19 pagesAbet Paper (Jee)MohsenMahroosNo ratings yet
- ASEE International Forum Paper ID 8242 by M Rashid Final GoodDocument9 pagesASEE International Forum Paper ID 8242 by M Rashid Final GoodfamtaluNo ratings yet
- Led CKTDocument13 pagesLed CKTfamtaluNo ratings yet
- CLD Course Participant ManualDocument20 pagesCLD Course Participant ManualfamtaluNo ratings yet
- 311198main Art and Sci of SE LONG 1-20-09Document22 pages311198main Art and Sci of SE LONG 1-20-09famtaluNo ratings yet
- Systems Engineering FondamentalsDocument222 pagesSystems Engineering Fondamentalsisaac2008100% (29)
- 102 OBE Impact-1Document10 pages102 OBE Impact-1famtaluNo ratings yet
- Rosenburg1983engineeringpresentation PDFDocument3 pagesRosenburg1983engineeringpresentation PDFfamtaluNo ratings yet
- 3D 06 Paper 36 MalaysiaDocument5 pages3D 06 Paper 36 MalaysiafamtaluNo ratings yet
- SEFI Annual Report 2012 2013Document20 pagesSEFI Annual Report 2012 2013famtaluNo ratings yet
- Competency Based CurriculumDocument88 pagesCompetency Based CurriculumfamtaluNo ratings yet
- HowToWriteObjectivesOutcomes PDFDocument0 pagesHowToWriteObjectivesOutcomes PDFJay Sunga VillanNo ratings yet
- P-Cad 2004 PCB User's GuideDocument619 pagesP-Cad 2004 PCB User's GuideJohn BrowerNo ratings yet
- Electrostatic and Electromagnetic Forces: Electronic Address: Tim - Henley@mail - Utoronto.caDocument9 pagesElectrostatic and Electromagnetic Forces: Electronic Address: Tim - Henley@mail - Utoronto.caTimothy Murray HenleyNo ratings yet
- CPU Vs vCPUDocument14 pagesCPU Vs vCPUainseanNo ratings yet
- Contactor Cap Lc1dDocument4 pagesContactor Cap Lc1dAlfiansyah Dharma Setia DjaketraNo ratings yet
- Rectify Binary Plate Efficiency BubblesDocument4 pagesRectify Binary Plate Efficiency BubblesCsaba AndrásNo ratings yet
- Preliminary Pin-out for 12 Cylinder Engine Control UnitDocument6 pagesPreliminary Pin-out for 12 Cylinder Engine Control UnitSUELENNo ratings yet
- Phase Diagrams IntroductionDocument76 pagesPhase Diagrams IntroductionGikiTopiNo ratings yet
- Oral and Practical Tests: MechanicDocument19 pagesOral and Practical Tests: MechanicHugo AlmeidaNo ratings yet
- Torque Specifications: Service Specifications - Ra60F Manual TransmissionDocument1 pageTorque Specifications: Service Specifications - Ra60F Manual TransmissionPedro Javier Castro SanchezNo ratings yet
- Vacuum Chill BlockDocument2 pagesVacuum Chill BlockAditheya Varthan MNo ratings yet
- Hoarding Guide 2020Document46 pagesHoarding Guide 2020Mohammed HafizNo ratings yet
- Industrial Insulation Applications: Green Engineering-1 Insulation Spreadsheets - ContentDocument55 pagesIndustrial Insulation Applications: Green Engineering-1 Insulation Spreadsheets - ContentRashel HasanNo ratings yet
- KALEKİMDocument18 pagesKALEKİMqaisalkurdyNo ratings yet
- GM300 SMDocument46 pagesGM300 SMSrboljub Milosavljevic100% (1)
- Ball MillsDocument8 pagesBall MillsBoy Alfredo PangaribuanNo ratings yet
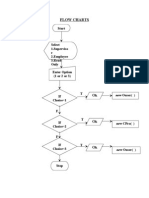
- Flow Charts Option: StartDocument13 pagesFlow Charts Option: StartbalabooksNo ratings yet
- Instruction Manual STR 155 RL-1Document24 pagesInstruction Manual STR 155 RL-1VENDI100% (3)
- Udayanandan, Notes On Tensors PDFDocument56 pagesUdayanandan, Notes On Tensors PDFhristos314No ratings yet
- Plant Cost EstimationDocument49 pagesPlant Cost EstimationAlpianto100% (1)
- Human-Environment InteractionDocument3 pagesHuman-Environment Interactionapi-299100358No ratings yet
- Partitioned Data Set Extended Usage Guide Guide: Front CoverDocument364 pagesPartitioned Data Set Extended Usage Guide Guide: Front CoverCsutka PocsNo ratings yet
- Standardization of Welding ElectrodesDocument8 pagesStandardization of Welding ElectrodesAqsa BanoNo ratings yet
- SLTRT Service Level Testing Reporting ToolDocument110 pagesSLTRT Service Level Testing Reporting ToolChedli Dhouibi50% (2)
- Fassmer Freefall - Lifeboat Type CFL (-T) 49 ManualDocument55 pagesFassmer Freefall - Lifeboat Type CFL (-T) 49 Manualkayhan aytugNo ratings yet
- LB2 UC30 Data Sheet enUS 80218564235Document5 pagesLB2 UC30 Data Sheet enUS 80218564235Ahmed ShawkyNo ratings yet
- BlowersDocument58 pagesBlowersmahmad61100% (1)
- Environmental Quality Control of Emission From Diesel Engines Regulations 1996 - P.U.a 429-96Document22 pagesEnvironmental Quality Control of Emission From Diesel Engines Regulations 1996 - P.U.a 429-96scribdledeeNo ratings yet
- The Magnaflux Advantage (Whole Catalog)Document51 pagesThe Magnaflux Advantage (Whole Catalog)Andy StkNo ratings yet
- GRAS 46BE 1/4Document9 pagesGRAS 46BE 1/4nino16041973No ratings yet
- Capacitor Banks - Schedules FILLEDDocument11 pagesCapacitor Banks - Schedules FILLEDyahyaNo ratings yet
- 2020 Can Am Off Road - Apache Track Kits Leaflet - enDocument7 pages2020 Can Am Off Road - Apache Track Kits Leaflet - enNicolas VillamayorNo ratings yet