You might also like
- M. Gabriel Khan - Cardiac Drug Therapy, Calcium Channel BlockersDocument21 pagesM. Gabriel Khan - Cardiac Drug Therapy, Calcium Channel BlockersluongcongthucNo ratings yet
- Calcium Antagonists in HypertensionDocument1 pageCalcium Antagonists in HypertensionIntan SyamimiNo ratings yet
- How Calcium Channel Blockers Work to Treat Heart ConditionsDocument1 pageHow Calcium Channel Blockers Work to Treat Heart ConditionsrajeshmangalNo ratings yet
- Dihydropyridine Calcium-Channel Blockers (Such As Nifedipine) Act On Slow, L-TypeDocument4 pagesDihydropyridine Calcium-Channel Blockers (Such As Nifedipine) Act On Slow, L-TypeTrương Văn HiếuNo ratings yet
- Calcium Channel Blockers PharmacologyDocument31 pagesCalcium Channel Blockers PharmacologyBusy worldNo ratings yet
- 1 s2.0 S0019483213003386 MainDocument5 pages1 s2.0 S0019483213003386 MainNK KJNo ratings yet
- Bihs PDFDocument4 pagesBihs PDFFredrikus Lay Berkh MansNo ratings yet
- Drugs For Systemic Hypertension and Angina: What's New?Document6 pagesDrugs For Systemic Hypertension and Angina: What's New?Diana GarcíaNo ratings yet
- Antihypertensive Drugs: HypertensionDocument8 pagesAntihypertensive Drugs: Hypertensionalmastar officeNo ratings yet
- PharmaAntianginal DrugsDocument175 pagesPharmaAntianginal DrugsNidal AbboudNo ratings yet
- Calcium Channel Blockers: Mechanisms, Types, Uses & Side EffectsDocument6 pagesCalcium Channel Blockers: Mechanisms, Types, Uses & Side EffectsManyal Kutin KoakNo ratings yet
- Dihydropiridines IndicationsDocument1 pageDihydropiridines IndicationsrajeshmangalNo ratings yet
- Lecture 1 antihypertensionSDSDocument7 pagesLecture 1 antihypertensionSDSSara AbbasNo ratings yet
- Lectures Combined CardiologieDocument143 pagesLectures Combined CardiologiedocsNo ratings yet
- Calcium Channel Blockers: Symposium On: Antihypertensive Drugs.Document16 pagesCalcium Channel Blockers: Symposium On: Antihypertensive Drugs.sathishelakkiyaNo ratings yet
- L7 heart failure practice essayDocument2 pagesL7 heart failure practice essaymoshlingmomoNo ratings yet
- Pharmacology PerfusionDocument1 pagePharmacology PerfusionkatrinasdNo ratings yet
- Calcium Channel Blockers (CCBS)Document3 pagesCalcium Channel Blockers (CCBS)Yohanes SutrisnoNo ratings yet
- Calcium Channel Blockers Mechanism of Action and UsesDocument19 pagesCalcium Channel Blockers Mechanism of Action and UsesanojanNo ratings yet
- Calcium Channel Blockers inDocument15 pagesCalcium Channel Blockers inAnonymous NeRC5JYiSNo ratings yet
- Franz H. Messerli - Cardiac Effects of Calcium Antagonists in HypertensionDocument8 pagesFranz H. Messerli - Cardiac Effects of Calcium Antagonists in HypertensionluongcongthucNo ratings yet
- Anoosha Roll#21Document19 pagesAnoosha Roll#21Anusha ZubairNo ratings yet
- Case Study Number 1Document5 pagesCase Study Number 1Kevin Kyle RizarriNo ratings yet
- Generic Name Brand Name Drug Class Mechanism of Action StructureDocument4 pagesGeneric Name Brand Name Drug Class Mechanism of Action StructurenoelkiddoNo ratings yet
- Angina PectorisDocument4 pagesAngina PectorisKrishnendu RayNo ratings yet
- Antiangina 2016Document40 pagesAntiangina 2016Indra Mahaputra100% (1)
- Pharmacology of The Cardiovascular SystemsDocument4 pagesPharmacology of The Cardiovascular SystemsMark Russel Sean LealNo ratings yet
- ACE Inhibitors and ARBsDocument20 pagesACE Inhibitors and ARBsMylene MendozaNo ratings yet
- 10 5772@intechopen 90778Document18 pages10 5772@intechopen 90778Arbi SulaimanNo ratings yet
- A Review On: Nicardipine HydrochlorideDocument5 pagesA Review On: Nicardipine HydrochloridekiranNo ratings yet
- beta-blockers-and-calcium-channel-blockersDocument34 pagesbeta-blockers-and-calcium-channel-blockersnevena.stankovic986No ratings yet
- Ischemic Heart Disease Revised LMKDocument50 pagesIschemic Heart Disease Revised LMKLateef KhanNo ratings yet
- Anti-Anginal Drugs ExplainedDocument19 pagesAnti-Anginal Drugs ExplainedAnusha ZubairNo ratings yet
- Drugs Used in Heart FailureDocument27 pagesDrugs Used in Heart Failurealeah morenoNo ratings yet
- Advance Concept in Nursing Unit 3Document34 pagesAdvance Concept in Nursing Unit 3Kamran AltafNo ratings yet
- Chapter 17 Cardiovascular DrugsDocument35 pagesChapter 17 Cardiovascular Drugsaisyahasrii_No ratings yet
- Cardio PharmacologyDocument21 pagesCardio Pharmacologyb.bethel2003No ratings yet
- Antianginal Drugs DR Hussam 2023Document12 pagesAntianginal Drugs DR Hussam 2023ManWol JangNo ratings yet
- Antianginal DrugsDocument3 pagesAntianginal DrugsSarah MendozaNo ratings yet
- Prepared By: Shukri Yusuf ElmiDocument17 pagesPrepared By: Shukri Yusuf ElmiabdishakurNo ratings yet
- CVS (HF, HTN) PharmacologyDocument99 pagesCVS (HF, HTN) PharmacologyCherenet TomaNo ratings yet
- Agents For Angina - IODocument12 pagesAgents For Angina - IOJoël N PaulNo ratings yet
- CALCIUM CHANNEL BLOCKER OVERDOSE: SIGNS, DIAGNOSIS, TREATMENTDocument6 pagesCALCIUM CHANNEL BLOCKER OVERDOSE: SIGNS, DIAGNOSIS, TREATMENTfaradillaNo ratings yet
- 10 and 11 Treatment of Hypertension and AnginaDocument10 pages10 and 11 Treatment of Hypertension and AnginaBrandon AviciiNo ratings yet
- Drug Study ON Calcium Channel BlockerDocument3 pagesDrug Study ON Calcium Channel BlockerDaily DoseNo ratings yet
- Calcium Channel Blockers EncyclopediaDocument5 pagesCalcium Channel Blockers EncyclopediaReiNo ratings yet
- FARMAKOGNOSI - Obat AntihipertensiDocument7 pagesFARMAKOGNOSI - Obat AntihipertensiTrianisa FebyNo ratings yet
- Vasodilator Drugs: Therapeutic Use and Rationale Therapeutic Uses of VasodilatorsDocument6 pagesVasodilator Drugs: Therapeutic Use and Rationale Therapeutic Uses of VasodilatorsHuy NguyễnNo ratings yet
- Antihypertensive Drugs ٠١١٦٥٨Document10 pagesAntihypertensive Drugs ٠١١٦٥٨mohnad806mNo ratings yet
- Chapter - 024 Heart Failure DrugsDocument7 pagesChapter - 024 Heart Failure DrugsthubtendrolmaNo ratings yet
- Anti-Anginal Drugs PharmacologyDocument24 pagesAnti-Anginal Drugs PharmacologyDharun RanganathanNo ratings yet
- VASODILATORSDocument30 pagesVASODILATORSEvangelin MelvinNo ratings yet
- Katzung 12th EditionDocument1,245 pagesKatzung 12th EditionAvin Guptha28% (87)
- Antiarrhythmic Drugs: Dr. Sachana KC 1 Year Resident Department of AnesthesiaDocument67 pagesAntiarrhythmic Drugs: Dr. Sachana KC 1 Year Resident Department of AnesthesiaKshitizma GiriNo ratings yet
- Anti Arrhythmic DrugsDocument91 pagesAnti Arrhythmic DrugsAlex beharuNo ratings yet
- Cilnidipine 1Document62 pagesCilnidipine 1dkhandke0% (1)
- AmlodipineDocument2 pagesAmlodipineAlexis Abigail de LeonNo ratings yet
- Cardiovascular Agents PDFDocument118 pagesCardiovascular Agents PDFgherlethrNo ratings yet
- Jurnal Kimed 5Document4 pagesJurnal Kimed 5Zilmaida SalomNo ratings yet
- Baker RC Armstrong Ma Young Is Mcclean E O Rourke D Campbell FC Dsa Aa Mcbride WTDocument5 pagesBaker RC Armstrong Ma Young Is Mcclean E O Rourke D Campbell FC Dsa Aa Mcbride WTrajeshmangalNo ratings yet
- Antiplatlet MechanismDocument3 pagesAntiplatlet MechanismrajeshmangalNo ratings yet
- School Name CalicutDocument3 pagesSchool Name CalicutrajeshmangalNo ratings yet
- Reference Literature ReviewDocument1 pageReference Literature ReviewrajeshmangalNo ratings yet
- LiverDocument6 pagesLiverrajeshmangalNo ratings yet
- HeartDocument2 pagesHeartrajeshmangalNo ratings yet
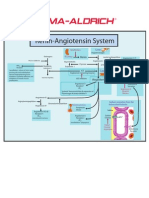
- Angio Ren inDocument1 pageAngio Ren inEndang Dwi KurniaNo ratings yet
- Neuro 1Document1 pageNeuro 1rajeshmangalNo ratings yet
- Normal ValuesDocument3 pagesNormal ValuesSubir DasNo ratings yet
- Angio Ren inDocument1 pageAngio Ren inEndang Dwi KurniaNo ratings yet
- Foodborne Illnes1Document2 pagesFoodborne Illnes1rajeshmangalNo ratings yet
- Gamma Amino Butyric AcidDocument1 pageGamma Amino Butyric AcidrajeshmangalNo ratings yet
- Infectious DoseDocument1 pageInfectious DoserajeshmangalNo ratings yet
- Normal Process of 5-HT and Noradrenaline NeurotransmissionDocument1 pageNormal Process of 5-HT and Noradrenaline NeurotransmissionrajeshmangalNo ratings yet
- Paecilomyces Fungal Species, Associated With A Range of Moldy and Rotting Fruits andDocument2 pagesPaecilomyces Fungal Species, Associated With A Range of Moldy and Rotting Fruits andrajeshmangalNo ratings yet
- Jejuni 77.3%, Salmonella 20.9%, Escherichia Coli O157:H7 1.4%, and All Others Less ThanDocument1 pageJejuni 77.3%, Salmonella 20.9%, Escherichia Coli O157:H7 1.4%, and All Others Less ThanrajeshmangalNo ratings yet
- Risks From Smoking During Pregnancy: Effects On MothersDocument1 pageRisks From Smoking During Pregnancy: Effects On MothersrajeshmangalNo ratings yet
- Bacterial Foodborne Pathogens: Causes and EffectsDocument1 pageBacterial Foodborne Pathogens: Causes and EffectsrajeshmangalNo ratings yet
- Aflatoxin SDocument1 pageAflatoxin SrajeshmangalNo ratings yet
- Exo ToxinsDocument1 pageExo ToxinsrajeshmangalNo ratings yet
- Incubation PeriodDocument1 pageIncubation PeriodrajeshmangalNo ratings yet
- Arasites: The Scolex of Tenia Solium, A Pork TapewormDocument1 pageArasites: The Scolex of Tenia Solium, A Pork TapewormrajeshmangalNo ratings yet
- Chloroquine: Adverse EffectsDocument1 pageChloroquine: Adverse EffectsrajeshmangalNo ratings yet
- 60 Minute Yoga Program for Centering, Breathing & Warm UpsDocument1 page60 Minute Yoga Program for Centering, Breathing & Warm UpsrajeshmangalNo ratings yet
- Pathogenic Agents that Cause Foodborne IllnessDocument1 pagePathogenic Agents that Cause Foodborne IllnessrajeshmangalNo ratings yet
- Preventing Bacterial Food PoisoningDocument1 pagePreventing Bacterial Food PoisoningrajeshmangalNo ratings yet
- Mycotoxins and Alimentary MycotoxicosesDocument1 pageMycotoxins and Alimentary MycotoxicosesrajeshmangalNo ratings yet
- VirusesDocument1 pageVirusesrajeshmangalNo ratings yet
- Foodborne Illness (Also Foodborne Disease and Referred To As Food Poisoning) IsDocument1 pageFoodborne Illness (Also Foodborne Disease and Referred To As Food Poisoning) IsrajeshmangalNo ratings yet
- Iso 128-34-2001 PDFDocument18 pagesIso 128-34-2001 PDFAhmed MaaloulNo ratings yet
- HissDocument17 pagesHissJuan Sánchez López67% (3)
- Starch and Cereals RecipeDocument20 pagesStarch and Cereals RecipeWinsher Pitogo100% (1)
- Carbon Monoxide Poisoning - Wikipedia, The Free EncyclopediaDocument19 pagesCarbon Monoxide Poisoning - Wikipedia, The Free EncyclopediaSundar SugumarNo ratings yet
- Java Interview Guide - 200+ Interview Questions and Answers (Video)Document5 pagesJava Interview Guide - 200+ Interview Questions and Answers (Video)Anand ReddyNo ratings yet
- Cabarroguis CLUP SEA ReportDocument91 pagesCabarroguis CLUP SEA ReportAlvin Lee Cucio Asuro100% (3)
- Stewart Paul Lucky Luke and Other Very Short Stories With ExDocument111 pagesStewart Paul Lucky Luke and Other Very Short Stories With ExЕлена Сидлаковская100% (1)
- Asmo Kilo - PL Area BPP Juni 2023 v1.0 - OKDocument52 pagesAsmo Kilo - PL Area BPP Juni 2023 v1.0 - OKasrulNo ratings yet
- A Project About Wild Animals Protection Week and Kalakad Mundanthurai Tiger ReserveDocument50 pagesA Project About Wild Animals Protection Week and Kalakad Mundanthurai Tiger ReserveSweetNo ratings yet
- Unit Weight or Density of Different Construction MaterialsDocument2 pagesUnit Weight or Density of Different Construction MaterialsHari RNo ratings yet
- William Shakespeare's: The Comedy of ErrorsDocument19 pagesWilliam Shakespeare's: The Comedy of ErrorsAsjsjsjsNo ratings yet
- ML QB Unit WiseDocument11 pagesML QB Unit WiseyogeshNo ratings yet
- BRM 2.Document10 pagesBRM 2.Sehar AzharNo ratings yet
- DRT, Drat & Sarfaesi Act (2002Document17 pagesDRT, Drat & Sarfaesi Act (2002Mayank DandotiyaNo ratings yet
- Who Would Think That Love - LyricDocument1 pageWho Would Think That Love - LyricNatália RamosNo ratings yet
- Lviv in Your Pocket - October December 2009Document23 pagesLviv in Your Pocket - October December 2009Anti FreezeNo ratings yet
- Reduce Blind Zones and Improve Safety With Proper Side Mirror AdjustmentDocument7 pagesReduce Blind Zones and Improve Safety With Proper Side Mirror AdjustmentjhoniNo ratings yet
- Car Parking - Rules and Regulations For Patients and Visitors - SOP0084Document2 pagesCar Parking - Rules and Regulations For Patients and Visitors - SOP0084in123No ratings yet
- Diverse Russian and US missiles specifications comparedDocument121 pagesDiverse Russian and US missiles specifications comparedandyt10No ratings yet
- Glenn GreenbergDocument3 pagesGlenn Greenbergannsusan21No ratings yet
- CNS Cellular Reactions and Classical Disease PatternsDocument184 pagesCNS Cellular Reactions and Classical Disease Patternsdray2bigNo ratings yet
- Wells Fargo Preferred CheckingDocument4 pagesWells Fargo Preferred Checkingjames50% (2)
- DFA and DOLE Not Liable for Repatriation Costs of Undocumented OFWDocument80 pagesDFA and DOLE Not Liable for Repatriation Costs of Undocumented OFWdhanty20No ratings yet
- Fromm, Erich - Working Class in Weimar Germany (Berg, 1980)Document302 pagesFromm, Erich - Working Class in Weimar Germany (Berg, 1980)RyadStarXWNo ratings yet
- Poe. Ligeia PDFDocument12 pagesPoe. Ligeia PDFClaudia Henríquez FaríasNo ratings yet
- Automata and Complexity Theory ModuleDocument104 pagesAutomata and Complexity Theory ModuleSurafelNo ratings yet
- BRCC Selection Policy HP Sept 2014 by Vijay Kumar Heer PDFDocument7 pagesBRCC Selection Policy HP Sept 2014 by Vijay Kumar Heer PDFVIJAY KUMAR HEERNo ratings yet
- Leading From A Distance: 5 Lessons For Successful Virtual TeamingDocument6 pagesLeading From A Distance: 5 Lessons For Successful Virtual TeamingFARIDNo ratings yet
- India's Elite Anti-Naxalite Force CoBRADocument6 pagesIndia's Elite Anti-Naxalite Force CoBRAhumayunsagguNo ratings yet