You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Diagnosis and Treatment of Hair PDFDocument11 pagesThe Diagnosis and Treatment of Hair PDFSpica AdharaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Diagnosis and Treatment of Hair PDFDocument11 pagesThe Diagnosis and Treatment of Hair PDFSpica AdharaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Mesenteric Cyst in InfancyDocument27 pagesMesenteric Cyst in InfancySpica AdharaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Not All Acne Is Acne VulgarisDocument14 pagesNot All Acne Is Acne VulgarisSpica AdharaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Chemical Peels in The Treatment of Acne PDFDocument8 pagesChemical Peels in The Treatment of Acne PDFSpica AdharaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Acne Scars Pathogenesis Classification and TreatmentDocument10 pagesAcne Scars Pathogenesis Classification and TreatmentSpica AdharaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Acne Scars Pathogenesis Classification and TreatmentDocument10 pagesAcne Scars Pathogenesis Classification and TreatmentSpica AdharaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Truncal Pruritus PDFDocument6 pagesTruncal Pruritus PDFSpica AdharaNo ratings yet
- A Diagnostic Approach To PruritusDocument8 pagesA Diagnostic Approach To PruritusSpica AdharaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Intertrochanteric MEDSCAPEDocument5 pagesIntertrochanteric MEDSCAPESpica AdharaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Nasa ThesisDocument8 pagesNasa Thesisdnr3krf8100% (2)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- 9500 MPR Wireless TransmissionDocument46 pages9500 MPR Wireless TransmissionMahdi AhmadiNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Tugas Topic 4 Devi PermatasariDocument8 pagesTugas Topic 4 Devi PermatasariMartinaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Who Has Allergies & Why: Allergies, Also Known As Allergic Diseases, Are A Number of Conditions Caused byDocument6 pagesWho Has Allergies & Why: Allergies, Also Known As Allergic Diseases, Are A Number of Conditions Caused byJun Dl CrzNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- MHFU Hunter RankDocument5 pagesMHFU Hunter RankGustin PrayogoNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- First Periodical Exam Math 8Document2 pagesFirst Periodical Exam Math 8Joanne88% (8)
- Mardi Gras Recipe Sampler by Mitchell Rosenthal, Author of Cooking My Way Back HomeDocument13 pagesMardi Gras Recipe Sampler by Mitchell Rosenthal, Author of Cooking My Way Back HomeThe Recipe Club100% (1)
- LEVEL 2-Anxiety-Adult (PROMIS Emotional Distress-Anxiety - Short Form)Document1 pageLEVEL 2-Anxiety-Adult (PROMIS Emotional Distress-Anxiety - Short Form)alemsaudementalNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Global Environment Unit 2Document13 pagesGlobal Environment Unit 2Se SathyaNo ratings yet
- BTS "Whalien 52" Lyrics Romanization, English and Indonesian TranslationDocument11 pagesBTS "Whalien 52" Lyrics Romanization, English and Indonesian TranslationEmaFediFeniNo ratings yet
- Ap Art and Design Drawing Sustained Investigation Samples 2019 2020 PDFDocument102 pagesAp Art and Design Drawing Sustained Investigation Samples 2019 2020 PDFDominic SandersNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Infant of A Diabetic MotherDocument17 pagesInfant of A Diabetic MotherLovina Falendini AndriNo ratings yet
- Form 03B Heritage Bell 1Document2 pagesForm 03B Heritage Bell 1ValNo ratings yet
- BDSM List FixedDocument4 pagesBDSM List Fixedchamarion100% (3)
- People at Virology: Dmitri Iosifovich Ivanovsky - Founders of VirologyDocument2 pagesPeople at Virology: Dmitri Iosifovich Ivanovsky - Founders of VirologyFae BladeNo ratings yet
- Ref Manual - Additives For MA Spinel PDFDocument5 pagesRef Manual - Additives For MA Spinel PDFRITWIK SARKARNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- CMR ArtifactDocument51 pagesCMR ArtifactAdel SALLAMNo ratings yet
- 2004 - Quality of Life in Romania I MargineanDocument206 pages2004 - Quality of Life in Romania I Margineandale_titiNo ratings yet
- MECH0018.1 Assignment 2 QP Fall 2021Document17 pagesMECH0018.1 Assignment 2 QP Fall 2021saleem razaNo ratings yet
- Okumas Guide To Gaijin 1Document90 pagesOkumas Guide To Gaijin 1Diogo Monteiro Costa de Oliveira SilvaNo ratings yet
- DinmjgDocument10 pagesDinmjghaker linkisNo ratings yet
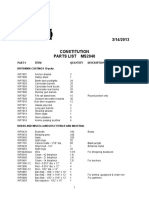
- MS2040 Constitution Parts ListDocument6 pagesMS2040 Constitution Parts ListTemptationNo ratings yet
- EPTT5100 - Pressure - Temperature Sensor - 1308 - GDocument2 pagesEPTT5100 - Pressure - Temperature Sensor - 1308 - GHendry Putra RahadiNo ratings yet
- Advance Probability and Statistics - 2014 - 2da Edición - Ottman PDFDocument383 pagesAdvance Probability and Statistics - 2014 - 2da Edición - Ottman PDFAdan Graus RiosNo ratings yet
- Unit II Construction PracticesDocument61 pagesUnit II Construction PracticesiploguNo ratings yet
- Type of TrucksDocument8 pagesType of TrucksYojhan VelezNo ratings yet
- B11 - Overload Relays (Ref) ENDocument20 pagesB11 - Overload Relays (Ref) ENAhmed AbazaNo ratings yet
- Better Place - Heaven or HellDocument3 pagesBetter Place - Heaven or HellToto SammyNo ratings yet
- SuctioningDocument58 pagesSuctioningAyusa PradhanNo ratings yet
- 9trffi&hpr.! Ni-: Use E EDocument2 pages9trffi&hpr.! Ni-: Use E ERafi ZulfiNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)