Professional Documents
Culture Documents
Kolik Abdomen
Uploaded by
uflah_Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Kolik Abdomen
Uploaded by
uflah_Copyright:
Available Formats
CLINICAL PRACTICE
Diagnostic Approach and Management of Acute Abdominal Pain
Murdani Abdullah, M. Adi Firmansyah
Department of Internal Medicine, Faculty of Medicine, University of Indonesia - Cipto Mangunkusumo Hospital. Jl. Diponegoro no. 71, Jakarta Pusat 10430, Indonesia. Correspondence mail: murdani.abdullah@ui.ac.id; murdani@hotmail.com.
ABSTRAK Insiden nyeri abdomen akut dilaporkan berkisar 510% pada kunjungan pasien ke unit gawat darurat. Kegawatan abdomen yang datang ke rumah sakit dapat berupa kegawatan bedah atau kegawatan non bedah. Penyebab tersering dari akut abdomen antara lain appendisitis, kolik bilier, kolisistitis, divertikulitis, obstruksi usus, perforasi viskus, pankreatitis, peritonitis, salpingitis, adenitis mesenterika dan kolik renal. Kemampuan yang baik dalam identifikasi awal memerlukan pengetahuan yang baik pula terutama mengenai anatomi dan fisiologi saluran cerna yang tercermin saat melakukan anamnesis dan pemeriksaan fisis khususnya pemeriksaan fisis abdomen. Dengan semakin canggihnya pemeriksaan, baik pemeriksaan radiologi dan endoskopi, tata laksana pasien dengan akut abdomen juga semakin luas selain terapi farmakologi dan terapi bedah. Endoskopi teraupetik, terapi radiologi intervensi dan terapi melalui laparoskopi dewasa ini merupakan modalitas yang biasa dilakukan pada pasien dengan akut abdomen. Kata kunci: nyeri abdomen, akut abdomen, anamnesis, pemeriksaan fisis abdomen. ABSTRACT The incidence of acute abdominal pain ranges between 5-10% of all visits at emergency department. Abdominal emergencies of hospital visits may include surgical and non-surgical emergencies. The most common causes of acute abdomen are appendicitis, biliary colic, cholecystitis, diverticulitis, bowel obstruction, visceral perforation, pancreatitis, peritonitis, salpingitis, mesenteric adenitis and renal colic. Good skills in early diagnosis require a sound knowledge of basic anatomy and physiology of gastrointestinal tract, which are reflected during history taking and particularly, physical examination of the abdomen. Advanced diagnostic approaches such as radiography and endoscopy enhance the treatment for acute abdomen including pharmacological and surgical treatment. Therapeutic endoscopy, interventional radiology treatment and therapy using adult laparoscopy are the common modalities for treating patients with acute abdomen. Key words: abdominal pain, acute abdomen, history taking, abdominal physical examination.
INTRODUCTION
Abdominal pain is one of common problems encountered by doctors, either in primary or secondary health care (specialists). It may be mild, but it may also a life-threatening sign. It has been estimated that almost 50% adults have experienced abdominal pain1,2 and it accounts for 510% of all emergency visits.3-6 Cautious care should be taken when dealing with elderly
patients (>65 years) who suffered from abdominal pain since they are at 6-8 times greater risk for mortality,7 especially if the final diagnosis cannot be established in the Emergency Department.8 In general, abdominal pain is categorized based on the onset as acute or chronic pain. Sudden onset of abdominal pain that lasts for less than 24 hours is considered as acute abdominal pain. This article will have greater focus on acute
344
Acta Medica Indonesiana - The Indonesian Journal of Internal Medicine
Vol 44 Number 4 October 2012
Diagnostic approach and management of acute abdominal pain
abdominal pain as it is one of gastroenterology emergencies.
DEFINITION
Acute abdominal pain or better known as acute abdomen is defined as tremendous severe pain (which has maximal score when being described through VAS visual analog score scoring system) arising the abdominal area and requires immediate care. It is an abdominal emergency situation that may be caused by surgical or non-surgical problems. Therefore, as clinicians, especially those who provide primary health care must be able to identify the case as either surgical or non-surgical case. Good skills in early diagnosis require a sound knowledge of basic anatomy and physiology of gastrointestinal tract, which are reflected during history taking and physical examination. When dealing with acute abdominal pain, a series of questions should be automatically come to our thought that will help us to establish the
diagnosis, such as: what are the characteristics of pain? (Is the pain localized or diffused all over the abdomen?); which organs that possibly involved by considering the location of abdominal pain? which kind of pain receptors that probably involved? (visceral or somatic); are there any gastrointestinal dysfunction associated with the pain?; what are the possible cause of the pain? Moreover, the most important question includes whether it requires surgical intervention or only need conservative treatment.
ANATOMY AND PHYSIOLOGY
Generally, abdominal pain is divided into visceral and parietal components. Visceral pain is transmitted by C nerve fibers that commonly found in muscle, periosteum, mesentery, peritoneum and viscera. Most of nociception from abdominal visceral is conveyed by this type of fiber and tends to be interpreted as dull, cramping, burning sensation, poorly localized. It is also more likely to have greater variation and
Heart
midbrain medulla Larynx Trachea Bronchi Lungs
Vagal nerve
Superior cervical ganglion
Esophagus Stomach
Celiac ganglion
Abdominal blood vessels Liver Bile ducts Pancreas
Superior mesentric ganglion
Adrenal Small intestines Large intestines
Inferior mesentric ganglion
Kidney
bladder Pelvic nerves Reproductive organ
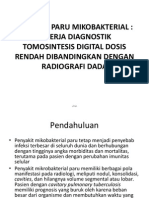
Figure 1. Pathways of visceral sensory innervation. Afferent fibers that mediate pain travel with autonomic nerve system to communicate with the central nervous system. In the abdomen, these nerves include both vagal and pelvic parasympathetic nerves and thoracolumbar sympathetic nerves. Sympathetic nerve fibers (red line); parasympathetic nerve fibers (blue lines).
345
Murdani Abdullah
Acta Med Indones-Indones J Intern Med
duration compared to the somatic pain. Visceral pain is usually perceived to be in the epigastrium, periumbilical or hypogastrium. It occurs since the visceral organs in the abdomen transmit sensory afferent stimuli to both side of the spinal cord (Figure 1).9,10 Moreover, visceral pain is poorly localized due to lower number of nerve endings in visceral organ than other organs such as the skin and since the innervations of viscera is multisegmental. Parietal pain is conveyed by A- fibers, which are abundantly found in the skin and muscle. The stimuli of this nerve pathway are perceived as the sharp, sudden and well-localized pain mimicking the pain that follows acute injury. The pain is often aggravated by movement or vibration. Parietal pain due to inflammation of parietal peritoneum is usually more intense and localized than visceral. For example, in acute appendicitis, the early pain is periumbilical visceral pain, which is followed by the localized somatoparietal pain at McBurneys point produced by inflammatory process of the parietal peritoneum. The term of referred pain is defined as the pain felt far from the involved organs. It occurs when there is a convergence of visceral afferent neurons with parietal afferent neurons from different anatomic regions on second-order neurons in the spinal cord at the same spinal segment. The abovementioned Figure 2 illustrates how the inflammatory process in diaphragm due to spleen rupture or subphrenic hematoma can be perceived as shoulder pain (the Kehr sign); while Table 1 demonstrates the common sites of referred pain that mostly have been reported.9,10
ETIOLOGY
to brain
spinal cord
Visceral afferent first order neuron (A) Spinal cord second order neuron (B) Somatic afferent first order neuron C
Figure 2. Illustration of the neuroanatomic basis of referred pain. Visceral afferent fibers innervating the diaphragm can be stimulated by local irritation (e.g. the presence of subdiaphragmatic abscess: the circle sign). These nerve fibers (A) synapse with second-order neurons in the spinal cord (B) together with somatic afferent fibers (C) arising from the left shoulder area. The brain subsequently interprets the pain to be parietal or somatic in origin and localizes it to the shoulder.
Table 1. Location and causes of referred pain10 Right Shoulder -- Liver -- Bile duct -- Right hemidiaphragm Left Shoulder -- Heart -- Caudal pancreas -- Spleen -- Left hemidiaphragm Scrotum and Testis -- Ureter
Acute abdominal pain may be caused by various etiologies as indicated by the following Table 2. A study conducted by Irvin found that the most common causes of acute abdominal pain in the Emergency Department are non-specific abdominal pain (35%), appendicitis (17%), bowel obstruction (15%), urology causes (6%), biliary disorder (5%), diverticular disease (4%) and pancreatitis (2%).9 The most common causes of acute abdomen are appendicitis, biliary colic, cholecystitis, diverticulitis, bowel obstruction, visceral perforation, pancreatitis, peritonitis, salpingitis, mesenteric adenitis, and renal colic. Moreover, there are less common causes of acute abdomen
including hepatoma necrosis, splenic infarction, myocardial infarction, diabetic ketoacidosis, inflammatory aneurysma, sigmoid, caecum or stomach volvulus and a manifestation of herpes zoster.9,11 Occasionally, the etiology of abdominal pain can be predicted based on its location and the type of pain, which may help doctors in establishing the diagnosis. The etiologies of pain based on the location is illustrated in Figure 3 (3-1 up to 3-3) and the following Figure 4. In addition to abdominal pain, the presence of other complaints should also be noticed. Patients may have other problems including nausea, vomiting, anorexia, bloating, watery stool or constipation. Anorexia occurs in almost all causes of acute abdomen, particularly acute appendicitis and acute cholecystitis; however, it is rarely found in urology or gynecology cases. Vomiting
346
Vol 44 Number 4 October 2012
Diagnostic approach and management of acute abdominal pain
Table 2. Comparison of common causes of abdominal pain Causes Appendicitis Cholecystitis Pancreatitis Diverticulitis Perforated peptic ulcer Small bowel obstruction Ruptured abdominal aortic aneurysm Mesenteric ischemia/infraction Gastroenteritis Pelvic inflammation Ruptured ectopic pregnancy Onset Gradual Acute Acute Gradual Sudden Gradual Sudden Sudden Gradual Gradual Sudden Location Periumbilical early; RLQ late RUQ Epigastric, back LLQ Epigastric Periumbilical Abdominal, back, flank Periumbilical Periumbilical LQ, pelvic LQ, pelvic Characteristics Diffuse early, localized late Localized Localized Localized Localized early, diffuse late Diffuse Diffuse Diffuse Diffuse Localized Localized Description Ache Constricting Blunt Ache Burning sensation Cramping Tearing Sharp Spasmodic Blunt Sharp Radiation None Scapula Back None None None None None None Upper thigh None +++ ++ +++ +++ + to ++ ++ ++ Intensity ++ ++ ++ to +++
+ = mild; ++ = moderate; +++ = severe; LLQ = left lower quadrant; RLQ = right lower quadrant; RUQ = right upper quadrant
is a common early complaint of acute abdominal pain. It is assumed that this condition is due to reflex stimulation of medullary vomiting center. Vomiting reflex in early acute abdomen usually is not progressive. Nevertheless, bowel obstruction should be considered when there is progressive and continuous vomiting accompanied with severe abdominal pain. Abdominal pain, which is accompanied with abdominal distention due to excessive gas, should be considered as a sign of ileus or bowel obstruction. Other complaints of obstipation resulted from disrupted bowel passage that associated with absence of flatus and the presence of abdominal distention should increase our awareness on the possibility of ileus or bowel obstruction. In contrast, abdominal pain that accompanied with constipation but without distention, which often occur in elderly, should be considered as possible diverticulitis. If abdominal pain is accompanied with bloody watery stools, then the possibility of IBD (inflammatory bowel disease) should be considered along with differential diagnosis of mesenteric ischemia or possible thrombosis of mesenteric veins.8,9,11
PHYSICAL EXAMINATION
Besides a thorough history taking, abdominal physical examination is the main key assistance in establishing the diagnosis. We should begin
physical examination by assessing the patients general appearance and the ABC (Airway, Breathing, Circulation) status. The patients ability to converse, breathing pattern, potion in bed and facial expression should be observed carefully. Obese patient should be asked about unusual abdominal enlargement. Assessment of bowel sound (auscultation) should be conducted before doing other examination maneuvers (palpation or percussion). Perform auscultation for at least two minutes and on more than one abdominal region before concluding any diminished bowel sound. Several characteristic signs are often used to assist doctors in considering the causes of abdominal pain. For example, the Murphys sign, i.e. right upper quadrant tenderness during palpation produced when the patient takes a deep inspiration. It is a sensitive, but not a specific sign for acute cholecystitis. Another sign, e.g. the presence of tenderness during palpation and patients reaction after the palpation accompanied with rigidity at McBurneys point (1/3 of the way between the umbilicus and spina iliaca anterior superior) is quite sensitive to indicate acute appendicitis. Corvoisier sign (a palpable gallbladder) in patient with clinical jaundice is sensitive enough to bring the suspicion for possible pancreatic periampula tumor. The presence of Cullens sign, i.e. periumbilical ecchymosis may
347
Murdani Abdullah
Acta Med Indones-Indones J Intern Med
cholecystitis hepatitis
pancreatitis biliary colic ureteric colic (kidney stone) diverticulitis small intestinal obstruction colon obstruction
perforated ulcer pielonephritis, renal or ureteric colic
appendicitis
tuboovarian abscess or ectopic pregnancy
cholecystitis
pancreatitis
perforated ulcer pielonephritis, renal or ureteric colic
appendicitis
Figure 3. A) Pain characteristics: gradual, progressive; B) Pain characteristics: colic, cramping, intermitten; C) Pain characteristics: sudden, severe pain; D) Referred pain. The circles indicate primary source or area with very intense pain.10
be useful to indicate hemoperitoneum. In the endemic area of tuberculosis such as Indonesia, the presence of chest board phenomenon may suggest tuberculosis peritonitis.9-11 The pelvic organs and external genitalia should be also examined in every patient with acute abdominal pain. Rectal touch (digital rectal examination) or vaginal touch may occationally provide additional valued information. Evaluation of gynecologic abnormality should be performed in all female patients with acute abdominal pain.
LABORATORY TESTS
Although meticulous history taking and appropriate physical examination have major part in establishing the etiology of acute abdominal pain, but the role of laboratory tests cannot be disregarded. In fact, all patients with acut abdominal pain should have a complete peripheral blood count (including differential count of leukocytes), determination of serum electrolyte, ureum, creatinine, blood glucose and urinalysis. Pregnancy testing should be
performed in all women of reproductive age with abdominal pain. Liver function tests and determination of serum amylase level should be ordered in patients with abdominal pain of upper right quadrant, either with or without clinical jaundice.9-11 Three-position plain abdominal radiographs should be done to determine the presence of perforation signs, ileus and bowel obstruction. Plain abdominal radiographs may be helpful in evaluating pancreatic calcification, vertebral fracture and radioluscent stone of renal contour. Another routine test is abdominal ultrasonography (abdominal USG), which may reveal disrupted hepatobiliary system, urinary tract and gynecologic tract as well as the acute appendicitis. Nowadays, other imaging tests such as colon in loop, gastrointestinal endoscopy, abdominal CT-scan, MRI CT arteriography have been increasingly used. However, those tests should be ordered appropriately and consistent with the indication considering that the cost is still relatively high.
348
Vol 44 Number 4 October 2012
Diagnostic approach and management of acute abdominal pain
Right upper quadrant Lung: effusion, empyema, pneumonia Liver: hepatitis, liver congestion, abscess, hematoma, malignancy Biliary: cholecystitis, choledocolithiasis, cholangitis Duodenum: perforated ulcer
Epigastrium Heart: ischemia, pericardial effusion Esophagus: esophagitis, rupture Stomach/duodenum: dyspepsia, gastritis, ulcer, obstruction, volvulus Pancrease: pandreatitis, pseudocysts, malignancy Aortic aneurysm
Left upper quadrant Lung: effusion, empyema Heart: ischemia Spleen: abscess, rupture Stomach: perforated ulcer
Right hypochondrium Kidney: pielonephritis, infarction, abscess Ureter: stone, hydronephrosis
Lower right quadrant Right small intestines & colon: appendicitis (late stage) ileitis, ischemia, mesenteric adenitis, diverticulitis Gynecology: ectopic pregnancy, salpingitis, tuboovarian abscess, torsion, endometriosis Inguinal: pelvic disease, hernia, lymphadenopathy Duodenum: perforated ulcer
Periumbilical Small intestines: enteritis, appendicitis (early stage), ileus, obstruction, ischemia, ileitis (Crohn disease) Right colon: appendicitis (early stage), colitis, caecum volvulus Aortic aneurysm
Left hypochondrium Kidney: pielonephritis, infarction, abscess Ureter: stone, hydronephrosis Spleen: abscess, rupture, splenomegaly
Hypogastrium Colon: diverticulitis, colitis (infection,IBD, ischemia), irritable bowel syndrome Bladder: cystitis, acute urine retention Gynecology: ectopic pregnancy
Left lower quadrant Left colon: diverticulitis, sigmoid volvulus, ischemia, colitis (IBD), irritable bowel syndrome Gynecology: ectopic pregnancy, salpingitis, tuboovarian abscess, torsion, endometriosis Inguinal: pelvic disease, hernia, lymphadenopathy
Figure 4. Summary of differential diagnosis for abdominal pain based on its location. IBD=inflammatory bowel disease.12
The summary of diagnostic approach and the necessary diagnostic tests for patients with abdominal pain is presented in Figure 5.
TREATMENT
the surgery may not be performed immediately, we should decide when the surgery will be performed.
REFERENCES
1. Hyams JS, Burke G, Davis PM, et al. Abdominal pain and irritable bowel syndrome in adolescents: a community-based study. J Pediatr. 1996;129:220. 2. Heading RC. Prevalence of upper gastrointestinal symptoms in the general population: a systematic review. Scand J Gastroenterol Suppl. 1999;231:3. 3. Brewer BJ, Golden GT, Hitch DC, et al. Abdominal pain. An analysis of 1,000 consecutive cases in a University Hospital emergency room. Am J Surg. 1976; 131:219. 4. Powers RD, Guertler AT. Abdominal pain in the ED: stability and change over 20 years. Am J Emerg Med. 1995;13:301. 5. Kamin RA, Nowicki TA, Courtney DS, Powers RD. Pearls and pitfalls in the emergency department evaluation of abdominal pain. Emerg Med Clin North Am. 2003;21:61. 6. An G, West M. Abdominal compartment syndrome: A concise clinical review. Crit Care Med. 2008;36:130410. 7. Hustey FM, Meldon SW, Banet GA, et al. The use of abdominal computed tomography in older ED patients with acute abdominal pain. Am J Emerg Med. 2005; 23:259. 8. Fenyo G. Acute abdominal disease in the elderly: experience from two series in Stockholm. Am J Surg. 1992;143:751.
In keeping with advanced diagnostic approaches such as radiography and endoscopy enhance the treatment for acute abdomen including pharmacological and surgical treatment. Therapeutic endoscopy, interventional radiology treatment and therapy using adult laparoscopy are the common modalities for treating patients with acute abdomen. Several studies reported that early treatment by administering analgesics may provide pain relief and does not obscure diagnosis. The analgesics that frequently used are opioids. In addition, appropriate antibiotics should be provided in accordance with the indication, e.g. for peritonitis. In some conditions, empirical antibiotic treatment may be given when establishing the working diagnosis of abdominal pain without waiting for the results of culture tests.9 In general, the management of patient with acute abdomen ultimately includes the determination whether the case is surgical case which requires surgical treatment. Moreover, if
349
Murdani Abdullah
Acta Med Indones-Indones J Intern Med
acute abdominal pain ABC Limitation: unstable hemodynamic no yes
evaluation
possible diagnosis
Resuscitation Consult immidiate surgery Consider FAST Consider laparatomy
Visceral perforation Severe pancreatitis Spleen rupture/hemoperitoneum Ruptured abdominal aortic aneurysm
yes RLQ pain (gradual): Tenderness during palpation on RLQ Positive reaction of tenderness after palpation USG/CT Examination on appendix Appendicitis*
For female patients, consider pelvic USG/CT
Tuboovarian abscess Ovarian torsion Ectopic pregnancy
no
RUQ pain (gradual): the presence of discomfort after having meal
yes
USG of right upper quadrant
Cholelithiasis Cholecystitis Gallbladder obstruction Cholangitis
no
Nausea, vomiting, obstipation, constipation, abdominal distention, history of previous surgery no
yes For female patients, consider pelvic USG/CT Small bowel obstruction
Sudden onset, diffused pain, tenderness during palpation, peritonitis signs
Plain abdominal radiographs or CT scan with oral contrast
Visceral perforation Diverticulitis Mesentric infarction Acute pancreatitis
Figure 5. Algorithm of evaluation approach in patients with abdominal pain ABC=airway, breathing, circulation; CT=computed tomography; FAST=focused abdominal sonogram for trauma; RLQ=right lower quadrant; RUQ=right upper quadrant; USG=ultrasonography. *For Left Lower Quadrant pain, the possible diagnosis is diverticulitis.9
9. Millham FH. Acute abdominal pain. In: Feldman M, Friedman LS, Brandt LJ, eds. Feldman: sleisenger and fordtran's gastrointestinal and liver disease. 9th ed. Philadelphia: Elvesier; 2010. p. 151-62. 10. Squires RA, Postier RG. Acute abdomen. In: Towsend CM, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston textbook of surgery: the biological basis of modern surgical practice. 19th ed. Philadelphia: Elvesier; 2012. p. 1141-59. 11. McQuaid K. Approach to the patient with gastrointestinal disease. In: Goldman L, Schafer AI, eds. Goldman: Goldmans cecil medicine. 24th ed. Philadelphia: Elvesier; 2012. p. 828-44.
350
You might also like
- 5.2.2.4 Contoh FmeaDocument10 pages5.2.2.4 Contoh Fmeauflah_No ratings yet
- Doa BerbukaDocument1 pageDoa Berbukauflah_No ratings yet
- PRC Puskesmas Ketapang II SampitDocument1 pagePRC Puskesmas Ketapang II Sampituflah_No ratings yet
- SongsDocument4 pagesSongsuflah_No ratings yet
- Hbsag 1Document1 pageHbsag 1uflah_No ratings yet
- 6 Langkah Cuci TanganDocument1 page6 Langkah Cuci Tanganuflah_No ratings yet
- Rujukan Umum 1Document2 pagesRujukan Umum 1uflah_No ratings yet
- Jefferson FrakturDocument2 pagesJefferson Frakturuflah_No ratings yet
- SongsDocument4 pagesSongsuflah_No ratings yet
- Blanko Rujukan GeneralDocument9 pagesBlanko Rujukan Generaluflah_No ratings yet
- Soal Akper d3Document6 pagesSoal Akper d3Muhamad AnwarNo ratings yet
- Poster 1Document3 pagesPoster 1uflah_No ratings yet
- 6 Langkah Cuci TanganDocument1 page6 Langkah Cuci Tanganuflah_No ratings yet
- Koles TrolDocument4 pagesKoles Troluflah_No ratings yet
- Tugas PKMDocument27 pagesTugas PKMuflah_No ratings yet
- Monitoring Penyediaan Obat EmergensiDocument2 pagesMonitoring Penyediaan Obat Emergensiuflah_No ratings yet
- Deskripsi RadiologiDocument8 pagesDeskripsi Radiologiuflah_No ratings yet
- Evaluasi Ketersediaan Obat Terhadap Formularium, Hasil Evaluasi Dan Tindak LanjutDocument3 pagesEvaluasi Ketersediaan Obat Terhadap Formularium, Hasil Evaluasi Dan Tindak LanjutIndra Nurita OctaviaNo ratings yet
- Ular BisaDocument14 pagesUlar Bisauflah_No ratings yet
- Jurnal TipoidDocument3 pagesJurnal TipoidNdHaa Anag CerewetNo ratings yet
- Kasus KPP AtermDocument17 pagesKasus KPP Atermuflah_No ratings yet
- Jurnal HepatitisDocument7 pagesJurnal Hepatitisputraelfauzi67% (6)
- Penyakit Paru Mikobakterial Dts Dengan Radiografi DadaDocument14 pagesPenyakit Paru Mikobakterial Dts Dengan Radiografi Dadauflah_No ratings yet
- Hubungan Merokok Dengan Kejadian Penyakit TBC Yang Berobat Di Puskesmas PrambonDocument3 pagesHubungan Merokok Dengan Kejadian Penyakit TBC Yang Berobat Di Puskesmas Prambonuflah_No ratings yet
- Myoma RizkiDocument54 pagesMyoma Rizkiuflah_No ratings yet
- Terminologi Sistem Produksi WanitaDocument41 pagesTerminologi Sistem Produksi Wanitauflah_No ratings yet
- Kasus KPP AtermDocument31 pagesKasus KPP Atermuflah_No ratings yet
- Referat GinekomastiaDocument15 pagesReferat Ginekomastiadr.tam tam putra panturaNo ratings yet
- De Bride MenDocument3 pagesDe Bride MenMalvino GiovanniNo ratings yet
- Dermatplogi Cleft Left and Lip CheftDocument30 pagesDermatplogi Cleft Left and Lip Cheftuflah_No ratings yet