You might also like
- Ishihara ChartDocument5 pagesIshihara ChartThalani NarasiyaNo ratings yet
- Part 380. Occupational Noise Exposure Example STS Calculation From Federal OSHA Request For Consultative Assistance (RCA)Document1 pagePart 380. Occupational Noise Exposure Example STS Calculation From Federal OSHA Request For Consultative Assistance (RCA)Thalani NarasiyaNo ratings yet
- Locker 1Document2 pagesLocker 1Thalani NarasiyaNo ratings yet
- Klinik Mediviron Setia AlamDocument2 pagesKlinik Mediviron Setia AlamThalani NarasiyaNo ratings yet
- Geriatric Handbook08Document152 pagesGeriatric Handbook08natalia anggraeniNo ratings yet
- IP-PRO Installer ManualDocument2 pagesIP-PRO Installer ManualThalani NarasiyaNo ratings yet
- GP Manual FinalDocument111 pagesGP Manual Finalskumara0% (1)
- 2015 - Week 1 Year 5Document2 pages2015 - Week 1 Year 5Thalani NarasiyaNo ratings yet
- Association of Systolic and Diastolic Blood Pressure On MortalityDocument10 pagesAssociation of Systolic and Diastolic Blood Pressure On MortalityThalani NarasiyaNo ratings yet
- Frank Shann PDFDocument118 pagesFrank Shann PDFThalani Narasiya67% (9)
- Dyspepsia AIPDocument6 pagesDyspepsia AIPIulia NiculaeNo ratings yet
- ASSIGNMENT 2-Haemato N OncoDocument2 pagesASSIGNMENT 2-Haemato N OncoThalani Narasiya0% (3)
- Children With Cancer PDFDocument92 pagesChildren With Cancer PDFThalani NarasiyaNo ratings yet
- 290 DistinguishingBetweenAsbestosisandSilicosisDocument9 pages290 DistinguishingBetweenAsbestosisandSilicosisThalani NarasiyaNo ratings yet
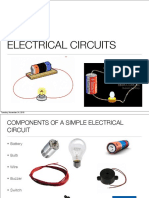
- Introduction To Electrical Circuit Year 6Document15 pagesIntroduction To Electrical Circuit Year 6Thalani NarasiyaNo ratings yet
- E-Machine GuideDocument70 pagesE-Machine GuideTaizenziggyNo ratings yet
- X Ray PositionDocument8 pagesX Ray PositionThalani NarasiyaNo ratings yet
- ASSIGNMENT 2-Kidney DiseaseDocument3 pagesASSIGNMENT 2-Kidney DiseaseThalani NarasiyaNo ratings yet
- Burns Management PDFDocument7 pagesBurns Management PDFRoh Bungaria N Garingging100% (1)
- Urinary Catheterization PrintableDocument8 pagesUrinary Catheterization PrintableThalani NarasiyaNo ratings yet
- 1.syllabus Regulations - ICSE - 2014 PDFDocument12 pages1.syllabus Regulations - ICSE - 2014 PDFThalani NarasiyaNo ratings yet
- Nilai Normal Vital PediatriDocument4 pagesNilai Normal Vital PediatriEkaPutri AzizNo ratings yet
- HODocument2 pagesHOThalani NarasiyaNo ratings yet
- JVPDocument5 pagesJVPThalani NarasiyaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Drugs and BruxismDocument14 pagesDrugs and BruxismAnthony HartonoNo ratings yet
- 1-Agenda of Meeting ECOO 2010 (CH)Document3 pages1-Agenda of Meeting ECOO 2010 (CH)tarikeopsNo ratings yet
- York County Court Schedule For Aug. 20Document15 pagesYork County Court Schedule For Aug. 20York Daily Record/Sunday NewsNo ratings yet
- Hemophilia: Factor IX (Hemophilia B)Document38 pagesHemophilia: Factor IX (Hemophilia B)Jhvhjgj JhhgtyNo ratings yet
- ChoreaDocument4 pagesChoreaapi-19973386No ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval Fasting Plasma Glucose: 102Document3 pagesLaboratory Test Report: Test Name Result Biological Reference Interval Fasting Plasma Glucose: 102Ramesh KumarNo ratings yet
- Alternative Treatment Strategies For Pseudo-Class III Malocclusion With Mild AsymmetryDocument17 pagesAlternative Treatment Strategies For Pseudo-Class III Malocclusion With Mild AsymmetrySchwan AbdulkareemNo ratings yet
- 香港脊醫 Hong Kong Chiropractors Dec 2017Document10 pages香港脊醫 Hong Kong Chiropractors Dec 2017CDAHKNo ratings yet
- Amy WebDocument62 pagesAmy WebAnotherAnonymomNo ratings yet
- Best Evidence Statement (Best)Document6 pagesBest Evidence Statement (Best)AleCsss123No ratings yet
- Safety For LabDocument14 pagesSafety For LabAravind B PatilNo ratings yet
- Tugas B Inggris IrmaDocument4 pagesTugas B Inggris IrmaIrma AprilNo ratings yet
- AA Dermatologia in MCC 2018Document61 pagesAA Dermatologia in MCC 2018marviNo ratings yet
- What You Need To Know About Your PsoasDocument3 pagesWhat You Need To Know About Your PsoasMihaela Banica100% (1)
- Preventive Resin Restorations: Review ArticlesDocument3 pagesPreventive Resin Restorations: Review ArticlesClaypella MaskNo ratings yet
- Vishal Sachan: Current Address: Permanent AddressDocument4 pagesVishal Sachan: Current Address: Permanent Addressvishal sachanNo ratings yet
- Islamic Method of Slaughtering Animals Is BetterDocument2 pagesIslamic Method of Slaughtering Animals Is Betterapi-26133437No ratings yet
- Chapter 4 Marketing Department: Company 1-Apollo Hospitals Enterprises LTD (Apollo)Document20 pagesChapter 4 Marketing Department: Company 1-Apollo Hospitals Enterprises LTD (Apollo)TYB92BINDRA GURSHEEN KAUR R.No ratings yet
- Directions: Choose The Letter of The Correct Answer. Write Your Answer On A Separate Sheet. STRICTLY NO Erasures and Write Capital Letters Only!Document3 pagesDirections: Choose The Letter of The Correct Answer. Write Your Answer On A Separate Sheet. STRICTLY NO Erasures and Write Capital Letters Only!Diane CiprianoNo ratings yet
- Dealing With PatientDocument14 pagesDealing With PatientAnggih PriyantoNo ratings yet
- European Pharmacopoeia 7 0 PDFDocument1 pageEuropean Pharmacopoeia 7 0 PDFMercedesNo ratings yet
- The 100 Most Influential Publications in Paracetamol Poisoning TreatmentDocument81 pagesThe 100 Most Influential Publications in Paracetamol Poisoning TreatmentPetrov MihaelaNo ratings yet
- Grand Halad Sa Kapamilya: List of ServicesDocument2 pagesGrand Halad Sa Kapamilya: List of ServicesLeo LastimosaNo ratings yet
- 10 - Cognitive TherapyDocument32 pages10 - Cognitive TherapymartinjeanellNo ratings yet
- Sitagliptin Slide Set Specialist - 1Document31 pagesSitagliptin Slide Set Specialist - 1Fannia Setiani100% (1)
- Patient Medical Records: Discharge and Home-Care InstructionsDocument27 pagesPatient Medical Records: Discharge and Home-Care InstructionsAnamaria ManceraNo ratings yet
- Walgreens SWOTDocument17 pagesWalgreens SWOTJoey LiewNo ratings yet
- Nursing Management of Patients With AutismDocument30 pagesNursing Management of Patients With AutismPolPelonio100% (1)
- Nursing Care Plan Problem Nursing Diagnosis Rationale Objective of Care Nursing Intervention Rationale EvaluationDocument1 pageNursing Care Plan Problem Nursing Diagnosis Rationale Objective of Care Nursing Intervention Rationale Evaluationplug06100% (1)
- CPR and Aed: Quiz #2 ResultsDocument2 pagesCPR and Aed: Quiz #2 ResultsNathan WhiteNo ratings yet