You might also like
- The Passive Aggressive Disorder PDFDocument13 pagesThe Passive Aggressive Disorder PDFPhany Ezail UdudecNo ratings yet
- Appendicitis Management and Nursing Care PlanDocument37 pagesAppendicitis Management and Nursing Care PlanAlva AlfaNo ratings yet
- Self-Learning Home Task (SLHT) : Key Drawings and Animation BreakdownsDocument6 pagesSelf-Learning Home Task (SLHT) : Key Drawings and Animation BreakdownsRUFINO MEDICONo ratings yet
- NCP Impaired SkinDocument2 pagesNCP Impaired Skinarjay2306_obcq100% (1)
- Year 8 - Higher - Autumn 2019Document16 pagesYear 8 - Higher - Autumn 2019nooraNo ratings yet
- Safe Handling of Chlorine From Drums and Cylinders (Second Edition)Document63 pagesSafe Handling of Chlorine From Drums and Cylinders (Second Edition)kapil 11No ratings yet
- Worcester Vs Ocampo - DigestDocument1 pageWorcester Vs Ocampo - DigestMaria Raisa Helga YsaacNo ratings yet
- Nursing Care Plan (Acute Pain)Document1 pageNursing Care Plan (Acute Pain)kyaw100% (2)
- Knapp TestDocument2 pagesKnapp TestGeorge Litu67% (3)
- Chap 9 Special Rules of Court On ADR Ver 1 PDFDocument8 pagesChap 9 Special Rules of Court On ADR Ver 1 PDFambahomoNo ratings yet
- NCP HemothoraxDocument3 pagesNCP HemothoraxMichael John F. NatividadNo ratings yet
- DLL Ict 9 1st Quarter Week 5Document3 pagesDLL Ict 9 1st Quarter Week 5Bernadeth Irma Sawal Caballa100% (2)
- CHED Memorandum Order # 5 (2008)Document121 pagesCHED Memorandum Order # 5 (2008)wiredpsyche100% (69)
- AppendectomyDocument6 pagesAppendectomyapi-3797941100% (10)
- Assessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation GoalDocument2 pagesAssessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation GoalI Am SmilingNo ratings yet
- ADDICTED (The Novel) Book 1 - The Original English TranslationDocument1,788 pagesADDICTED (The Novel) Book 1 - The Original English TranslationMónica M. Giraldo100% (7)
- Appendectomy Nursing Care Plan - Risk For InfectionDocument2 pagesAppendectomy Nursing Care Plan - Risk For InfectionChebz Zy0% (1)
- Nursing Care Plan Impaired ComfortDocument3 pagesNursing Care Plan Impaired ComfortAldwin Louis EstradaNo ratings yet
- 4 Appendectomy Nursing Care PlansDocument8 pages4 Appendectomy Nursing Care PlansMarin Andrei100% (1)
- NCP AppendicitisDocument6 pagesNCP AppendicitisRirin Ajeng Kartiningsih100% (1)
- NCP For Acute PainDocument2 pagesNCP For Acute PainEmman RamosNo ratings yet
- Assessment Diagnosis Planning Intervention Evaluation: VIII. Nursing Care PlanDocument1 pageAssessment Diagnosis Planning Intervention Evaluation: VIII. Nursing Care PlanKriz_sakuradreamNo ratings yet
- Cancer Care NCPDocument2 pagesCancer Care NCPMaverick LimNo ratings yet
- Nursing Care Plan Risk For InjuryDocument1 pageNursing Care Plan Risk For InjuryAce Dioso TubascoNo ratings yet
- R.O. Appendicitis.: Nursing Care Plan (NCP)Document2 pagesR.O. Appendicitis.: Nursing Care Plan (NCP)Karen Joy ItoNo ratings yet
- NCP 2 LRDR For PrintDocument2 pagesNCP 2 LRDR For PrintGeorge PandaNo ratings yet
- NCP Acute PainDocument5 pagesNCP Acute PainMicah Jonah Elicaño0% (1)
- Cues Nursing Diagnosis Scientific Reason Objective Nursing Intervention Rationale EvaluationDocument4 pagesCues Nursing Diagnosis Scientific Reason Objective Nursing Intervention Rationale Evaluationjomsportg0% (1)
- Nursing Care Plan TophiDocument2 pagesNursing Care Plan TophiAndrea Isabel U. O'DellNo ratings yet
- NCP Self CaRE DeficitDocument1 pageNCP Self CaRE Deficitnicole pageNo ratings yet
- Assessment Explanation of The Problem Planning Nursing Intervention Rationale EvaluationDocument2 pagesAssessment Explanation of The Problem Planning Nursing Intervention Rationale EvaluationRodolfo Bong SemaneroNo ratings yet
- Rabies PJ NCPDocument3 pagesRabies PJ NCPFredrick PaderangaNo ratings yet
- Drug Study Cefazolin and Vit KDocument2 pagesDrug Study Cefazolin and Vit KFrancis Lawrence AlexanderNo ratings yet
- NCP Inactivity ToleranceDocument16 pagesNCP Inactivity ToleranceChrisTine M. MoralesNo ratings yet
- Generic Name: Classification Indication:: Hema KDocument2 pagesGeneric Name: Classification Indication:: Hema KKristine YoungNo ratings yet
- NCP - Acute PainDocument2 pagesNCP - Acute PainsAm_300% (1)
- Case IcuDocument5 pagesCase IcuTrisha SuazoNo ratings yet
- Health Teaching Plan: Learning Objectives Content Rationale MethodologyDocument5 pagesHealth Teaching Plan: Learning Objectives Content Rationale Methodologyjoyrena ochondraNo ratings yet
- Drug Study, NCP, and Discharge Plan For AppendectomyDocument12 pagesDrug Study, NCP, and Discharge Plan For AppendectomyApril80% (5)
- NURSING CARE PLAN (Disturbed Body Image)Document1 pageNURSING CARE PLAN (Disturbed Body Image)Kay D. BeredoNo ratings yet
- Impaired Physical Mobility...Document3 pagesImpaired Physical Mobility...Christy BerryNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationRomeo Avecilla CabralNo ratings yet
- CHAPTER VIII Drug StudyDocument14 pagesCHAPTER VIII Drug StudyAnonymous opu4ls27No ratings yet
- NCP and DrugsDocument13 pagesNCP and DrugsApRil ANn ChUa BingcangNo ratings yet
- Case Presentation Station 3B Drug Study TramadolDocument3 pagesCase Presentation Station 3B Drug Study TramadolhahahahaaaaaaaNo ratings yet
- Subjective: Objective: Short Term: Independent: Independent: Short TermDocument2 pagesSubjective: Objective: Short Term: Independent: Independent: Short TermJohn Patrick CuencoNo ratings yet
- Concept MapDocument2 pagesConcept Mapjunifer laynoNo ratings yet
- AppendectomyDocument4 pagesAppendectomyKyre LandinginNo ratings yet
- NCP PainDocument2 pagesNCP PainJun TangonanNo ratings yet
- NCP Skin IntegityDocument3 pagesNCP Skin Integityclydell joyce masiarNo ratings yet
- Nursing Care Plan Acute PainDocument2 pagesNursing Care Plan Acute PainAdelaine LorestoNo ratings yet
- DP Discharge Plan@@@@@@@@Document6 pagesDP Discharge Plan@@@@@@@@Maemae SumalinogNo ratings yet
- Nursing Care Plan Student Nurse: Diestro, Angela Mae BSN 2BDocument3 pagesNursing Care Plan Student Nurse: Diestro, Angela Mae BSN 2BAngela Mae DiestroNo ratings yet
- NCP Impaired ComfortDocument2 pagesNCP Impaired ComfortGia P. de VeyraNo ratings yet
- NCP Risk For InjuryDocument2 pagesNCP Risk For Injurycristina_galang_2No ratings yet
- NCP (Or) ThyroidectomyDocument3 pagesNCP (Or) ThyroidectomyChiz CorreNo ratings yet
- Subjective:: Assessment Diagnosis Planning Implementation Rationale EvaluationDocument2 pagesSubjective:: Assessment Diagnosis Planning Implementation Rationale EvaluationAyra PunzalanNo ratings yet
- Assessment Healt H Patte RN Nursing Diagnosis Desired Outcome (Edit) Intervention (Edit) Evaluation (EDIT) Rema RKSDocument3 pagesAssessment Healt H Patte RN Nursing Diagnosis Desired Outcome (Edit) Intervention (Edit) Evaluation (EDIT) Rema RKStflorenzNo ratings yet
- Nursing Care Plan Spontaneous AbortionDocument2 pagesNursing Care Plan Spontaneous AbortionAbigael Rubio de LeonNo ratings yet
- Goal/s: After 20 Minutes of Nurse-Client Interaction, Client Will Be Knowledgeable About Newly Diagnosed Condition (Acute Appendicitis)Document3 pagesGoal/s: After 20 Minutes of Nurse-Client Interaction, Client Will Be Knowledgeable About Newly Diagnosed Condition (Acute Appendicitis)Rhn pjtNo ratings yet
- NCP InfectionDocument3 pagesNCP InfectionPrince AhmirNo ratings yet
- NCP (Postpartum Hemmorhage)Document3 pagesNCP (Postpartum Hemmorhage)Anne DyNo ratings yet
- NCPDocument3 pagesNCPNika LoNo ratings yet
- NCP PainDocument1 pageNCP Painsitz04No ratings yet
- Assessment Nursing Diagnosis Scientific Explanation Planning Intervention Rationale Evaluation IndeoendentDocument3 pagesAssessment Nursing Diagnosis Scientific Explanation Planning Intervention Rationale Evaluation IndeoendentDiane Sarino CabonceNo ratings yet
- NCPDocument3 pagesNCPLuiji Amor TiamzonNo ratings yet
- NCP LeptospirosisDocument6 pagesNCP LeptospirosisJean Marie DavidNo ratings yet
- Practical Nursing Diploma Program Pre-Clinical Nursing Care Research Assignment "Prep and Plan"Document7 pagesPractical Nursing Diploma Program Pre-Clinical Nursing Care Research Assignment "Prep and Plan"Jeremy ThomasNo ratings yet
- Nursing Care Plans: Cholecystitis CholelithiasisDocument8 pagesNursing Care Plans: Cholecystitis CholelithiasisAnnisa Fitriani NasutionNo ratings yet
- Nursing Diagnosis May Be Related To Possibly Evidenced byDocument37 pagesNursing Diagnosis May Be Related To Possibly Evidenced byLea TanNo ratings yet
- Connectors in Speaking: I Think (Opening Cues)Document4 pagesConnectors in Speaking: I Think (Opening Cues)Irish Nicole DCNo ratings yet
- Firstname M.I. Lastname, RN: Qualifications SummaryDocument4 pagesFirstname M.I. Lastname, RN: Qualifications SummaryIrish Nicole DCNo ratings yet
- MODULE 1: Overview MODULE 2: Understanding OSH MODULE 3: Recognizing Safety and Health Hazards and Appropriate Control MeasuresDocument2 pagesMODULE 1: Overview MODULE 2: Understanding OSH MODULE 3: Recognizing Safety and Health Hazards and Appropriate Control MeasuresIrish Nicole DCNo ratings yet
- 2021 RN Requirements ChecklistDocument1 page2021 RN Requirements ChecklistIrish Nicole DCNo ratings yet
- Connectors in Speaking: I Think (Opening Cues)Document4 pagesConnectors in Speaking: I Think (Opening Cues)Irish Nicole DCNo ratings yet
- 1-2 Setences Present Tense Time Element Place Participants: Writing Task 1Document7 pages1-2 Setences Present Tense Time Element Place Participants: Writing Task 1Irish Nicole DCNo ratings yet
- December 9, 2020 To: Dfa Robinsons SantiagoDocument1 pageDecember 9, 2020 To: Dfa Robinsons SantiagoIrish Nicole DCNo ratings yet
- Generic Name Stock Dose (Available in PH) Preparation Dose: InotropesDocument2 pagesGeneric Name Stock Dose (Available in PH) Preparation Dose: InotropesIrish Nicole DCNo ratings yet
- Explain The Term "Glycemic Index"Document3 pagesExplain The Term "Glycemic Index"Irish Nicole DCNo ratings yet
- Liliane Action PlanDocument2 pagesLiliane Action PlanIrish Nicole DCNo ratings yet
- Happy Pill: Yussef Carlisle Dela Cruz Grade IV - DiamondDocument1 pageHappy Pill: Yussef Carlisle Dela Cruz Grade IV - DiamondIrish Nicole DCNo ratings yet
- Baguio ItineraryDocument4 pagesBaguio ItineraryIrish Nicole DCNo ratings yet
- DSJHSDHFDJSHFFJKDSJHFDocument1 pageDSJHSDHFDJSHFFJKDSJHFIrish Nicole DCNo ratings yet
- Com-Tally 111Document60 pagesCom-Tally 111Irish Nicole DCNo ratings yet
- Substance AbuseDocument13 pagesSubstance AbuseIrish Nicole DCNo ratings yet
- LFD Trends 2016Document1 pageLFD Trends 2016Irish Nicole DCNo ratings yet
- Liver Cirrhosis: Irish Nicole Dela Cruz Gessel Ann BoguenDocument79 pagesLiver Cirrhosis: Irish Nicole Dela Cruz Gessel Ann BoguenIrish Nicole DCNo ratings yet
- CDH XXXXXXXDocument1 pageCDH XXXXXXXIrish Nicole DCNo ratings yet
- General Pathophysiology: Predisposing Factors: Precipitating FactorsDocument2 pagesGeneral Pathophysiology: Predisposing Factors: Precipitating FactorsIrish Nicole DCNo ratings yet
- Narrative ReportDocument1 pageNarrative ReportIrish Nicole DCNo ratings yet
- Questionnaire ThesisDocument5 pagesQuestionnaire ThesisIrish Nicole DCNo ratings yet
- Drug Use in LeprosyDocument23 pagesDrug Use in LeprosyIrish Nicole DCNo ratings yet
- Philippine CivilizationDocument4 pagesPhilippine CivilizationIrish Nicole DCNo ratings yet
- Diagnostic and Laboratory ExaminationsDocument4 pagesDiagnostic and Laboratory ExaminationsIrish Nicole DCNo ratings yet
- Gen PathoDocument2 pagesGen PathoIrish Nicole DCNo ratings yet
- Pillarican Rescuers Secured The Top SpotDocument1 pagePillarican Rescuers Secured The Top SpotIrish Nicole DCNo ratings yet
- Nursing ResearchDocument37 pagesNursing ResearchIrish Nicole DC100% (8)
- Drugs TableDocument1 pageDrugs TableIrish Nicole DCNo ratings yet
- Emcee - Graduation DayDocument5 pagesEmcee - Graduation DayBharanisri VeerendiranNo ratings yet
- Project Level 2Document5 pagesProject Level 2Alexa GonzalezNo ratings yet
- Last Speech of Shri Raghavendra SwamyDocument5 pagesLast Speech of Shri Raghavendra SwamyRavindran RaghavanNo ratings yet
- 4 Transistor Miniature FM TransmitterDocument2 pages4 Transistor Miniature FM Transmitterrik206No ratings yet
- DIALOGUE Samples B2 JUNE EXAMDocument4 pagesDIALOGUE Samples B2 JUNE EXAMIsabel María Hernandez RuizNo ratings yet
- Tips On Being A Successful StudentDocument2 pagesTips On Being A Successful Studentshimbir100% (3)
- High Court Judgment On Ex Party DecreeDocument2 pagesHigh Court Judgment On Ex Party Decreeprashant pathakNo ratings yet
- Internship Report-2020Document77 pagesInternship Report-2020Hossen ImamNo ratings yet
- Lista Materijala WordDocument8 pagesLista Materijala WordAdis MacanovicNo ratings yet
- Ebook PDF The Irony of Democracy An Uncommon Introduction To American Politics 17th Edition PDFDocument42 pagesEbook PDF The Irony of Democracy An Uncommon Introduction To American Politics 17th Edition PDFscott.stokley449100% (39)
- Integrating Intuition and Analysis Edward Deming Once SaidDocument2 pagesIntegrating Intuition and Analysis Edward Deming Once SaidRimsha Noor ChaudaryNo ratings yet
- Sepulveda v. de Las CasasDocument2 pagesSepulveda v. de Las CasasNova GaveNo ratings yet
- LRL Rudy Acuna On Neftali DeLeon - I Am Proud To Be The Grandson Son and Husband of Immigrants.Document9 pagesLRL Rudy Acuna On Neftali DeLeon - I Am Proud To Be The Grandson Son and Husband of Immigrants.EditorNo ratings yet
- Ahimsa From MahabharataDocument70 pagesAhimsa From MahabharataGerman BurgosNo ratings yet
- 5 Reported Speech - T16-6 PracticeDocument3 pages5 Reported Speech - T16-6 Practice39 - 11A11 Hoàng Ái TúNo ratings yet
- Rizal Course ReviewerDocument6 pagesRizal Course ReviewerMarianne AtienzaNo ratings yet
- Equilibrium of Firm Under Perfect Competition: Presented by Piyush Kumar 2010EEE023Document18 pagesEquilibrium of Firm Under Perfect Competition: Presented by Piyush Kumar 2010EEE023a0mittal7No ratings yet
- Revision Notes On Section 1.6 - Belief, Uncertainty & UnbeliefDocument5 pagesRevision Notes On Section 1.6 - Belief, Uncertainty & Unbeliefnisalielisha rodrigoNo ratings yet
- SjshagavDocument6 pagesSjshagavindah ayu lestariNo ratings yet
- Parathyroid Agents PDFDocument32 pagesParathyroid Agents PDFRhodee Kristine DoñaNo ratings yet
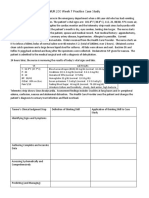
- NUR 200 Week 7 Practice Case StudyDocument2 pagesNUR 200 Week 7 Practice Case StudyJB NicoleNo ratings yet