You might also like
- W 8ben TdaDocument1 pageW 8ben TdaAnamaria Suciu100% (1)
- Member's Data Form (MDF) PAG-IBIGDocument3 pagesMember's Data Form (MDF) PAG-IBIGSimplyIreneNo ratings yet
- SLF066 CalamityLoanApplicationForm V04Document2 pagesSLF066 CalamityLoanApplicationForm V04marta100% (4)
- Certificate of Death 1Document2 pagesCertificate of Death 1Charley Labicani BurigsayNo ratings yet
- 2022 T1 Form - CompletedDocument8 pages2022 T1 Form - CompletedARSH GROVERNo ratings yet
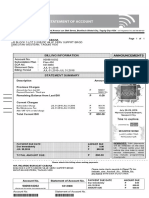
- Phil Ports Authority: Statement of AccountDocument6 pagesPhil Ports Authority: Statement of AccountPPA PUERTONo ratings yet
- Itr 2316Document1 pageItr 2316joshua158150% (2)
- Ebron, Dexter Jan Tago Gomez Bldg.,Fortich ST Sumpong Malaybalay City BUKIDNON, Northern Mindanao PhilippinesDocument3 pagesEbron, Dexter Jan Tago Gomez Bldg.,Fortich ST Sumpong Malaybalay City BUKIDNON, Northern Mindanao PhilippinesJan Karlyle Stefan EbronNo ratings yet
- BillingStatement - REY PJ S. BENDANA PDFDocument2 pagesBillingStatement - REY PJ S. BENDANA PDFLea BacalaoloyoNo ratings yet
- View Payslip: Personal Information Job InformationDocument1 pageView Payslip: Personal Information Job InformationJeffreyNo ratings yet
- Client Application DetailsDocument6 pagesClient Application DetailsSaran Kumar RamarNo ratings yet
- Ein Confirmation LetterDocument2 pagesEin Confirmation LetterzoneequizNo ratings yet
- Tax Return Enclosures List: FEDERAL T1 2009Document16 pagesTax Return Enclosures List: FEDERAL T1 2009Christine TemplemanNo ratings yet
- Proof of AccountDocument1 pageProof of AccountJonas SayconNo ratings yet
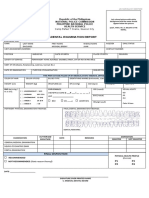
- Final Physical Medical-Dental Examination ReportDocument1 pageFinal Physical Medical-Dental Examination ReportmillerNo ratings yet
- Application For Visitor Visa (Temporary Resident Visa) : Validate Clear FormDocument4 pagesApplication For Visitor Visa (Temporary Resident Visa) : Validate Clear FormJorge Andres AvendañoNo ratings yet
- Australian Maritime VisaDocument5 pagesAustralian Maritime VisaShah HrNo ratings yet
- Personal Data Sheet UpdatedDocument7 pagesPersonal Data Sheet UpdatedEduard Jhourell Basilio100% (1)
- Table of ContentsDocument1 pageTable of ContentsMacLaw MacOfficeNo ratings yet
- W2 Matthew RussellDocument2 pagesW2 Matthew Russellmatthewrussell661No ratings yet
- Notice of AwardDocument54 pagesNotice of AwardJasmin UrbanozoNo ratings yet
- Rosemarie Sumalpong Indonto: Statement of AccountDocument4 pagesRosemarie Sumalpong Indonto: Statement of Accountpaul dave manaitNo ratings yet
- Annual Income Tax Return: (DonotentercentavosDocument2 pagesAnnual Income Tax Return: (DonotentercentavosKuhramaNo ratings yet
- Itr Rosare RobertoDocument8 pagesItr Rosare RobertoRafael ZamoraNo ratings yet
- Statement of Account: 681285458 24-Oct-2020 1,999.00 PDocument2 pagesStatement of Account: 681285458 24-Oct-2020 1,999.00 PELben RescoberNo ratings yet
- PDFDocument4 pagesPDFRomel VerdugoNo ratings yet
- Proof of BillingDocument1 pageProof of BillingSatoru Gojo100% (1)
- Affidavit of Exempt Status Under The Workers' Compensation ActDocument2 pagesAffidavit of Exempt Status Under The Workers' Compensation ActArlyn Jane PingolNo ratings yet
- Job Order Form: Converge Information and Communications Technology Solutions, IncDocument6 pagesJob Order Form: Converge Information and Communications Technology Solutions, IncJillNo ratings yet
- Official MDR PDFDocument1 pageOfficial MDR PDFBesarioLouiseCassandraNo ratings yet
- Kadena, Kaddex - RWL S.R.L. - Company Registration ReportDocument4 pagesKadena, Kaddex - RWL S.R.L. - Company Registration ReportJason M. RiveraNo ratings yet
- Cignal BillDocument1 pageCignal BillMark Bitoon100% (1)
- Statement of Account 16 01 Jul 19 To 31 Jul 19 875691478: Total Amount Due: P1,855.63Document3 pagesStatement of Account 16 01 Jul 19 To 31 Jul 19 875691478: Total Amount Due: P1,855.63jeraldenNo ratings yet
- Shunzeric Farm LLCDocument2 pagesShunzeric Farm LLCtcamon26No ratings yet
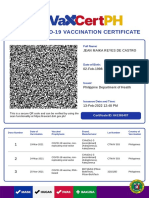
- Vaccination CertificateDocument1 pageVaccination CertificateJean MaikaNo ratings yet
- Undergrad Resumes and Cover LettersDocument10 pagesUndergrad Resumes and Cover LettersNandon RoyNo ratings yet
- Leo ResumeDocument2 pagesLeo Resumejao CentinoNo ratings yet
- Certificate of Business Name Registration: Lynmed PharmacyDocument1 pageCertificate of Business Name Registration: Lynmed PharmacyJuan Miguel PangilinanNo ratings yet
- Smart EE June 2022 - Service Application FormDocument10 pagesSmart EE June 2022 - Service Application FormMercy FeNo ratings yet
- Primewater BillDocument1 pagePrimewater BillMark Fel PunoNo ratings yet
- Statement of Account: 673916953 16-Jul-2019 748.00 PDocument2 pagesStatement of Account: 673916953 16-Jul-2019 748.00 PAldrin Admana AsuncionNo ratings yet
- Statement of Account: 678170259 16-Jul-2019 588.84 PDocument2 pagesStatement of Account: 678170259 16-Jul-2019 588.84 PIvy PantalunanNo ratings yet
- PTC 1Document2 pagesPTC 1Shierly Arciaga ProtacioNo ratings yet
- R A 7836Document4 pagesR A 7836Les Camacho SorianoNo ratings yet
- Account Summary: Credit Card NumberDocument6 pagesAccount Summary: Credit Card Numberanilvishaka7621No ratings yet
- Member Data Record: Philippine Health Insurance CorporationDocument1 pageMember Data Record: Philippine Health Insurance CorporationKristine OgalescoNo ratings yet
- Branchless Account Opening FormDocument2 pagesBranchless Account Opening FormCarmel DobleNo ratings yet
- Statement of Account: 981532811 04 - 2021 Mar 2,092.00 PDocument3 pagesStatement of Account: 981532811 04 - 2021 Mar 2,092.00 PLeonidas SpartacusNo ratings yet
- E Liwag 01312007 OLDDocument2 pagesE Liwag 01312007 OLDdaqs06No ratings yet
- Statement of Account 2 16 Apr 19 To 15 May 19 880757036: Total Amount Due: P1,684.16Document2 pagesStatement of Account 2 16 Apr 19 To 15 May 19 880757036: Total Amount Due: P1,684.16Dat Doria PalerNo ratings yet
- NYS - 45 Fill inDocument2 pagesNYS - 45 Fill inSalameh LaurieNo ratings yet
- Statement of Account: Dap-Dap Blk-40 Lot-32 Anupul Bamban TarlacDocument1 pageStatement of Account: Dap-Dap Blk-40 Lot-32 Anupul Bamban TarlacJoyce Gregorio ZamoraNo ratings yet
- Globe Postpaid Oct 2020 PDFDocument3 pagesGlobe Postpaid Oct 2020 PDFJasper GicaNo ratings yet
- Karl Lone S. Rivera B7 L30 Pavia St. Camella Milan, Cuyab, San Pedro, Laguna Mobile No.: 0916-278-7392Document2 pagesKarl Lone S. Rivera B7 L30 Pavia St. Camella Milan, Cuyab, San Pedro, Laguna Mobile No.: 0916-278-7392Karl Lone RiveraNo ratings yet
- 2019-H-294-01023 Acosta Bridge Decorative Lighting Permit - RedactedDocument28 pages2019-H-294-01023 Acosta Bridge Decorative Lighting Permit - RedactedAnne SchindlerNo ratings yet
- Smart Aug 2018Document6 pagesSmart Aug 2018Ash MangueraNo ratings yet
- So A 900920160610Document1 pageSo A 900920160610Francisco Oringo Sr ESNo ratings yet
- Document PDFDocument2 pagesDocument PDFMining AdminNo ratings yet
- BillingStatement - GENEVIEVE G. ANDAS PDFDocument2 pagesBillingStatement - GENEVIEVE G. ANDAS PDFGenevieve AndasNo ratings yet
- 24-7 Intouch PH IncDocument1 page24-7 Intouch PH Incflordeluna100% (1)
- 2551q BIR FormDocument2 pages2551q BIR FormJenniferFajutnaoArcos0% (1)
- Go Green and Receive Your Income Tax Notices Electronically: WWW - Iras.gov - SG Mytax - Iras.gov - SGDocument2 pagesGo Green and Receive Your Income Tax Notices Electronically: WWW - Iras.gov - SG Mytax - Iras.gov - SGJinchi WeiNo ratings yet
- BillingStatement - LOLITA P. AREVALO - 2Document2 pagesBillingStatement - LOLITA P. AREVALO - 2Franco Evale YumulNo ratings yet
- Member's Data Form (MDF) Print (NoDocument3 pagesMember's Data Form (MDF) Print (NoMitch LimNo ratings yet
- E-Commerce 070422Document18 pagesE-Commerce 070422Kate PotinganNo ratings yet
- Business ResearchDocument1 pageBusiness ResearchKate PotinganNo ratings yet
- Accomplishment Report 1Document12 pagesAccomplishment Report 1Kate PotinganNo ratings yet
- 2019 Convention - Confirmation FormDocument2 pages2019 Convention - Confirmation FormKate PotinganNo ratings yet
- IpcrDocument25 pagesIpcrKate PotinganNo ratings yet
- Info Update Form Aug2016Document3 pagesInfo Update Form Aug2016Kate PotinganNo ratings yet
- List of Allowances/Benefits As To Nature of Account Titles As Received by Officers Under Report On Salaries and Allowances (ROSA) SystemDocument3 pagesList of Allowances/Benefits As To Nature of Account Titles As Received by Officers Under Report On Salaries and Allowances (ROSA) SystemKate PotinganNo ratings yet
- 2016 Bar Results PDFDocument31 pages2016 Bar Results PDFKate PotinganNo ratings yet
- Final 2017 Roll-Out Training - ProgramDocument2 pagesFinal 2017 Roll-Out Training - ProgramKate PotinganNo ratings yet
- Bingo Socials Sales and Expenses (May 30,2017)Document4 pagesBingo Socials Sales and Expenses (May 30,2017)Kate PotinganNo ratings yet
- Mail Merge in ExcelDocument20 pagesMail Merge in ExcelNarayan ChhetryNo ratings yet
- Numeric Code AppDocument7 pagesNumeric Code AppIbelieve Ican FlyNo ratings yet
- Pag-Ibig MDF PDFDocument2 pagesPag-Ibig MDF PDFHG GalausNo ratings yet
- Imm 544 eDocument0 pagesImm 544 edesitoronto100% (1)
- GH Postcodes Jul19 v1 150719Document5 pagesGH Postcodes Jul19 v1 150719Addae MununkumNo ratings yet
- Pincode Serviceability Covid 18 4 2022 5 27Document292 pagesPincode Serviceability Covid 18 4 2022 5 27vragavhNo ratings yet
- GGDocument5 pagesGGjose lopezNo ratings yet
- QWT BusinessIntelligencePlan PDFDocument20 pagesQWT BusinessIntelligencePlan PDFGheorghe Ioan Pascu-GoNo ratings yet
- Rga Irs Pre GenDocument135 pagesRga Irs Pre Genpaul weichNo ratings yet
- Admission FormDocument1 pageAdmission FormHector AgudeloNo ratings yet
- Formal Correspondence WritingDocument17 pagesFormal Correspondence WritingJohn Baptist John BoscoNo ratings yet
- N 400Document21 pagesN 400Paul DalenNo ratings yet
- Post CodesDocument62 pagesPost Codesmuhad42762No ratings yet
- QWT BusinessIntelligencePlanDocument21 pagesQWT BusinessIntelligencePlanjnilson71No ratings yet
- Notification of Change of OwnershipDocument3 pagesNotification of Change of OwnershipMark BurkeNo ratings yet
- Application For Registration As A Vendor: Next PageDocument4 pagesApplication For Registration As A Vendor: Next PageMark KNo ratings yet
- Renub Research: Yammer - Product Analysis of Yammer IncDocument12 pagesRenub Research: Yammer - Product Analysis of Yammer Incapi-114525849No ratings yet
- Degree FormDocument2 pagesDegree FormAmmar Yaqoob MughalNo ratings yet
- Peoplesoft Human Resources: Prepared by The Office of Human Resources Updated April 2011Document116 pagesPeoplesoft Human Resources: Prepared by The Office of Human Resources Updated April 2011Dana MichaudNo ratings yet
- Sample Recommendation LettersDocument2 pagesSample Recommendation LettersChavanga AbelNo ratings yet
- Denmark's Basic Data Register Road MapDocument40 pagesDenmark's Basic Data Register Road MapePSI PlatformNo ratings yet
- PCC Application Form Instructions V2.0Document2 pagesPCC Application Form Instructions V2.0Aakshay KumarNo ratings yet
- Postal Codes All Pakistan Cities Zip Code / Postcode - Pakistan Postal Codes List - The Educationist HubDocument121 pagesPostal Codes All Pakistan Cities Zip Code / Postcode - Pakistan Postal Codes List - The Educationist HubAleena AhmedNo ratings yet
- Postcode List Jan 2014Document38 pagesPostcode List Jan 2014abdol1987No ratings yet
- KKU Scholar III Letter of PermissionDocument3 pagesKKU Scholar III Letter of PermissionekaNo ratings yet