You might also like
- Tvs HowsDocument1 pageTvs HowsshahbazNo ratings yet
- Pathogenesis of Bacterial InfectionDocument38 pagesPathogenesis of Bacterial Infectionshahbaz100% (2)
- IMMUNODEFICIENCIESDocument75 pagesIMMUNODEFICIENCIESshahbazNo ratings yet
- StaphylococciDocument73 pagesStaphylococcishahbaz100% (5)
- Neisseriae: February 8, 2008Document87 pagesNeisseriae: February 8, 2008shahbazNo ratings yet
- The StreptococciDocument16 pagesThe Streptococcishahbaz100% (5)
- ANTIBIOTICSDocument57 pagesANTIBIOTICSshahbazNo ratings yet
- Vaccines Part 2Document82 pagesVaccines Part 2shahbaz100% (1)
- ImmunizationDocument36 pagesImmunizationshahbaz100% (8)
- Normal Flora of The Human BodyDocument37 pagesNormal Flora of The Human Bodyshahbaz100% (6)
- The NeisseriaDocument16 pagesThe Neisseriashahbaz100% (1)
- Normal Flora of The Human BodyDocument7 pagesNormal Flora of The Human Bodyshahbaz88% (16)
- The StaphylococciDocument14 pagesThe Staphylococcishahbaz100% (2)
- Vaccines PART 1Document57 pagesVaccines PART 1shahbaz100% (1)
- Immunologic MethodsDocument6 pagesImmunologic Methodsshahbaz100% (1)
- Infection and ImmunityDocument15 pagesInfection and Immunityshahbaz100% (2)
- Sterilization and DisinfectionDocument5 pagesSterilization and Disinfectionshahbaz100% (14)
- Bacterial GrowthDocument6 pagesBacterial Growthshahbaz100% (1)
- Bacterial Structure - Lecture 1Document6 pagesBacterial Structure - Lecture 1shahbaz100% (2)
- Bacterial GeneticsDocument8 pagesBacterial Geneticsshahbaz100% (1)
- Pathogenesis of Bacterial InfectionDocument5 pagesPathogenesis of Bacterial Infectionshahbaz100% (4)
- AntibioticsDocument7 pagesAntibioticsshahbaz100% (3)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Natural Alternative Medicine 2013Document2 pagesNatural Alternative Medicine 2013kitianahelloNo ratings yet
- BIOLOGY AssessmemtDocument4 pagesBIOLOGY AssessmemtMei Joy33% (3)
- Connective TissuesstudDocument53 pagesConnective TissuesstudDanial Sharizul100% (1)
- The Massive Fraud Behind HIV Tests by Jon Rappoport PDFDocument9 pagesThe Massive Fraud Behind HIV Tests by Jon Rappoport PDFDan Bo100% (2)
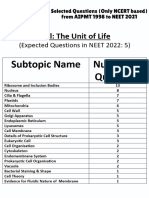
- Cell - The Unit of Life - NCERT Based PYQsDocument9 pagesCell - The Unit of Life - NCERT Based PYQsAkhil singhNo ratings yet
- Science Part 2Document1 pageScience Part 2Sheenlou Eian BartolomeNo ratings yet
- DNA Extraction and Polymerase Chain ReactionDocument2 pagesDNA Extraction and Polymerase Chain ReactionDudungNo ratings yet
- CMO No.15 s2007Document13 pagesCMO No.15 s2007John Michael BlancaflorNo ratings yet
- Human Anatomy and PhysiologyDocument136 pagesHuman Anatomy and PhysiologyLuis Margarejo91% (11)
- 02 Photosynthesis Calvin Cycle Light Independent ReactionsDocument38 pages02 Photosynthesis Calvin Cycle Light Independent ReactionsLaeliaMunawarohNo ratings yet
- Transgenics For Abiotic StressDocument46 pagesTransgenics For Abiotic StressAmit BallaniNo ratings yet
- Chapter 10 Non-Specific Host Defense MechanismDocument5 pagesChapter 10 Non-Specific Host Defense MechanismEanna ParadoNo ratings yet
- Agricultural MicrobiologyDocument256 pagesAgricultural MicrobiologyJay JayakumarNo ratings yet
- Heredity and Variation.Document6 pagesHeredity and Variation.AnweNo ratings yet
- Molecular Pathology of Endocrine Diseases - J. Hunt (Springer, 2010) WW PDFDocument268 pagesMolecular Pathology of Endocrine Diseases - J. Hunt (Springer, 2010) WW PDFMoldovan Tiberiu100% (1)
- Grade 11 - Mango Vaccination InformationDocument2 pagesGrade 11 - Mango Vaccination InformationKENNEDY VAGAYNo ratings yet
- Lympathic, Immune, Respiratory and Digestive Systems Homework (Key)Document14 pagesLympathic, Immune, Respiratory and Digestive Systems Homework (Key)Tuna BöncüNo ratings yet
- Inheritance (Multiple Choice) 1 QP PDFDocument16 pagesInheritance (Multiple Choice) 1 QP PDFCollins JimNo ratings yet
- MAKALAH. Struktur Dan Fungsi Sel, Jaringan Dan Sistem Tubuh ManusiaDocument23 pagesMAKALAH. Struktur Dan Fungsi Sel, Jaringan Dan Sistem Tubuh ManusiadediNo ratings yet
- LESSON PLAN Food Chains and Food Webs - AFT - Putri Dyah Astari (Quiz Only)Document13 pagesLESSON PLAN Food Chains and Food Webs - AFT - Putri Dyah Astari (Quiz Only)AfnestyaNo ratings yet
- Animal Kingdom Classification GuideDocument91 pagesAnimal Kingdom Classification GuideJoanna Susan JojiNo ratings yet
- G049 ColorectalDataset Sep07Document27 pagesG049 ColorectalDataset Sep07Gobinda RoyNo ratings yet
- Genetic diversity analysis of colored and white rice genotypes using Microsatellite (SSR) and Insertion-Deletion (INDEL) markersDocument11 pagesGenetic diversity analysis of colored and white rice genotypes using Microsatellite (SSR) and Insertion-Deletion (INDEL) markersMehvish ChNo ratings yet
- 69 Haines Ely-Is Psoriasis A Bowel DiseaseDocument14 pages69 Haines Ely-Is Psoriasis A Bowel DiseaseJoe DoeNo ratings yet
- Nutrition in Plants Class 7 Science NotesDocument4 pagesNutrition in Plants Class 7 Science NotesshravandownloadNo ratings yet
- Distribution, Morphology, Seasonal Dynamics, and Molecular Characterization of Tylenchulus Semipenetrans From Citrus Orchards in Southern IranDocument11 pagesDistribution, Morphology, Seasonal Dynamics, and Molecular Characterization of Tylenchulus Semipenetrans From Citrus Orchards in Southern IranSarai Olmedo CruzNo ratings yet
- Pandemics - What Everyone Needs To Know® (PDFDrive)Document268 pagesPandemics - What Everyone Needs To Know® (PDFDrive)arquivoslivros100% (1)
- ChlorophytaDocument13 pagesChlorophytamandow85No ratings yet
- Extract-N-Amp™ Tissue PCR Kit: Rapid Genomic DNA Extraction From Tissue Coupled With PCRDocument6 pagesExtract-N-Amp™ Tissue PCR Kit: Rapid Genomic DNA Extraction From Tissue Coupled With PCRSigma-Aldrich100% (2)
- BLOOD PRODUCTS COLLECTION & STORAGEDocument14 pagesBLOOD PRODUCTS COLLECTION & STORAGESathish SizzyNo ratings yet