You might also like
- ECG ReviewDocument146 pagesECG ReviewThea DinoNo ratings yet
- Approach: A. How The Kidney Handle The Proteins?Document9 pagesApproach: A. How The Kidney Handle The Proteins?Rashed ShatnawiNo ratings yet
- Approach To Ventricular ArrhythmiasDocument18 pagesApproach To Ventricular ArrhythmiasDavid CruzNo ratings yet
- ARRHYTHMIADocument82 pagesARRHYTHMIAjiluNo ratings yet
- PericarditisDocument29 pagesPericarditisPavin KumarNo ratings yet
- Tachyarrhythmia SDocument46 pagesTachyarrhythmia SAsif HameedNo ratings yet
- Spectrum of Acute Coronary Syndrome: Milagros Estrada-Yamamoto, MDDocument62 pagesSpectrum of Acute Coronary Syndrome: Milagros Estrada-Yamamoto, MDAnonymous HH3c17osNo ratings yet
- Ecg Pathology 02Document95 pagesEcg Pathology 02Andi MP Manurung100% (1)
- Free Medical ECG Interpretation PresentationsDocument30 pagesFree Medical ECG Interpretation PresentationsRohini SelvarajahNo ratings yet
- 6 Sec ECG Rhythm Strips Analysis GuideDocument10 pages6 Sec ECG Rhythm Strips Analysis GuideMalcum TurnbullNo ratings yet
- Focal Atrial Tachycardia I: Clinical Features, DiagnosisDocument10 pagesFocal Atrial Tachycardia I: Clinical Features, Diagnosisapi-26166949No ratings yet
- Ngaji Arrythmia Cordis 3Document122 pagesNgaji Arrythmia Cordis 3Dhita Dwi NandaNo ratings yet
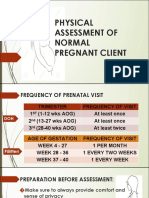
- Physical Assessment of a Pregnant ClientDocument25 pagesPhysical Assessment of a Pregnant ClientDe Leon, Austine Sydney D.No ratings yet
- BBB EcgDocument33 pagesBBB EcgLokbre YoasNo ratings yet
- ECG Learning ModulesDocument150 pagesECG Learning ModulesdodiNo ratings yet
- Essential Cardiac Electrophysiology: The Self-Assessment ApproachFrom EverandEssential Cardiac Electrophysiology: The Self-Assessment ApproachNo ratings yet
- Ekg Panum or OsceDocument69 pagesEkg Panum or OsceGladish RindraNo ratings yet
- Right Side EcgDocument4 pagesRight Side EcgDragos CirsteaNo ratings yet
- Wellen EcgDocument9 pagesWellen EcgElokNo ratings yet
- 4 5994641624901094407Document20 pages4 5994641624901094407Success100% (1)
- ECG Master Class-3Document97 pagesECG Master Class-3Shohag ID CenterNo ratings yet
- Systematic Layout PlanningDocument45 pagesSystematic Layout Planningkevin punzalan94% (31)
- Heartbeat Irregularities ExplainedDocument5 pagesHeartbeat Irregularities ExplainedKayelyn-Rose Combate100% (1)
- Patient with fever: Causes and typesDocument46 pagesPatient with fever: Causes and typesNosheen hafeez100% (1)
- Descending ParalysisDocument7 pagesDescending ParalysisgianpinotNo ratings yet
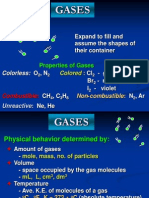
- Properties and Behavior of GasesDocument34 pagesProperties and Behavior of GasesPaul Jeremiah Serrano NarvaezNo ratings yet
- Advanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineDocument88 pagesAdvanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineRoroNo ratings yet
- Industrial Training (Tarun Kumar) - Final ReprtDocument46 pagesIndustrial Training (Tarun Kumar) - Final ReprtSaumya GargNo ratings yet
- Ventricular ArrhytmiaDocument30 pagesVentricular ArrhytmiaIkhsan AmadeaNo ratings yet
- What Is HyperlipidemiaDocument9 pagesWhat Is Hyperlipidemiaichanara100% (2)
- Hypertensive Crisis: Megat Mohd Azman Bin AdzmiDocument34 pagesHypertensive Crisis: Megat Mohd Azman Bin AdzmiMegat Mohd Azman AdzmiNo ratings yet
- Pain: Onset: Provocation: Mental Status Airway Skin Moisture Pulse Color TempDocument4 pagesPain: Onset: Provocation: Mental Status Airway Skin Moisture Pulse Color TempAlvarez StevenNo ratings yet
- Intubation ChecklistDocument2 pagesIntubation ChecklistDaniel CrookNo ratings yet
- A Guide To ECG Reporting For Year 3 Medical StudentsDocument2 pagesA Guide To ECG Reporting For Year 3 Medical StudentscsngiuNo ratings yet
- EKG PJK Co AssDocument115 pagesEKG PJK Co AsssalmaNo ratings yet
- StemiDocument34 pagesStemimonicaNo ratings yet
- Immunosuppressant Drugs Drug Name Class Function Method/Receptor UseDocument3 pagesImmunosuppressant Drugs Drug Name Class Function Method/Receptor UseKristin DouglasNo ratings yet
- ECG Interpretation in One PageDocument2 pagesECG Interpretation in One PageRyan AycockNo ratings yet
- Cardiac SarcoidosisDocument13 pagesCardiac SarcoidosisEmeric Jorge Macedo VendezuNo ratings yet
- EAR First AidDocument4 pagesEAR First Aidr_lakshmi2722No ratings yet
- 10 Steps To Learn ECG InterpretationDocument5 pages10 Steps To Learn ECG InterpretationIbrahem Y. NajjarNo ratings yet
- A Simplified ECG GuideDocument4 pagesA Simplified ECG GuideMarian Ioan-LucianNo ratings yet
- Mesenteric Ischemia in Dilated CardiomyopathyDocument30 pagesMesenteric Ischemia in Dilated CardiomyopathyJo AnneNo ratings yet
- Pediatric Shock: A Guide to Identification, Classification and Initial ManagementDocument20 pagesPediatric Shock: A Guide to Identification, Classification and Initial ManagementvgmanjunathNo ratings yet
- DD ScrotumDocument4 pagesDD ScrotumAy HaanNo ratings yet
- Mitral Valve ProlapseDocument5 pagesMitral Valve ProlapseDerofiez Hana RuhyadinNo ratings yet
- Lutembacher's Syndrome at KolonodaleDocument7 pagesLutembacher's Syndrome at KolonodaleWayan GunawanNo ratings yet
- Heparin and WarfarinDocument2 pagesHeparin and WarfarinBaeyer100% (1)
- Cardiovascular Nursing: Study Online atDocument7 pagesCardiovascular Nursing: Study Online atLilly DayeNo ratings yet
- Pediatric DKA: Section I: Scenario DemographicsDocument7 pagesPediatric DKA: Section I: Scenario DemographicsSugi DenyNo ratings yet
- Classification of MurmursDocument2 pagesClassification of MurmursNazneen SiddiquiNo ratings yet
- Cme Acs 2. Stemi (Izzah)Document36 pagesCme Acs 2. Stemi (Izzah)Hakimah K. SuhaimiNo ratings yet
- Ecg For InternsDocument25 pagesEcg For InternszeshooNo ratings yet
- Basic EP IntervalsDocument13 pagesBasic EP IntervalsdrharoonmohdNo ratings yet
- Ventricular Conduction DisturbancesDocument30 pagesVentricular Conduction DisturbancesNicholas PetrovskiNo ratings yet
- Ekg Full BibleDocument6 pagesEkg Full BibleTJNo ratings yet
- NSTEMI Refarat Cardio 2016Document48 pagesNSTEMI Refarat Cardio 2016Anonymous IOkNvM8VbtNo ratings yet
- Cardiology Case ReportDocument39 pagesCardiology Case ReportFara OmarNo ratings yet
- Atrial Septal DefekDocument29 pagesAtrial Septal DefekChe Ainil ZainodinNo ratings yet
- Nur 111 Session 6 Sas 1Document12 pagesNur 111 Session 6 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- Exam 3 pathophysiology Cancer growth types and characteristicsDocument7 pagesExam 3 pathophysiology Cancer growth types and characteristicsmenickel3No ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Lect 5Document8 pagesLect 5LuaNo ratings yet
- 1 Session1 DRR ConceptsDocument43 pages1 Session1 DRR ConceptsHoneylet Ü FerolNo ratings yet
- Land, Soil, Water, Natural Vegetation& Wildlife ResourcesDocument26 pagesLand, Soil, Water, Natural Vegetation& Wildlife ResourcesKritika VermaNo ratings yet
- Vision CSP22 Abhyaas Test 3SDocument44 pagesVision CSP22 Abhyaas Test 3SManasa DevarakondaNo ratings yet
- Circle, Cube, and CuboidsDocument27 pagesCircle, Cube, and CuboidsYohanes DhikaNo ratings yet
- Tie Technology DK SKDocument32 pagesTie Technology DK SKVladimir PleșcaNo ratings yet
- Tectonics, Vol. 8, NO. 5, PAGES 1015-1036, October 1989Document22 pagesTectonics, Vol. 8, NO. 5, PAGES 1015-1036, October 1989atoinsepeNo ratings yet
- Sample Format PDFDocument5 pagesSample Format PDFRhod R. AvisoNo ratings yet
- Totally New Term Dates 2013.20Document9 pagesTotally New Term Dates 2013.20nabub8No ratings yet
- Introduction To Computing Week 2Document23 pagesIntroduction To Computing Week 2Jerick FernandezNo ratings yet
- Deepali Bhartiya: TCI Express Limited Gurgaon Assistant Manager Prateek Group Noida Senior ExecutiveDocument3 pagesDeepali Bhartiya: TCI Express Limited Gurgaon Assistant Manager Prateek Group Noida Senior ExecutiveThe Cultural CommitteeNo ratings yet
- Checking battery control unitDocument3 pagesChecking battery control unitjuanNo ratings yet
- Visvesvaraya Technological University BelagaviDocument148 pagesVisvesvaraya Technological University BelagavichetanbvNo ratings yet
- HavellsDocument4 pagesHavellsanurag_iiitmNo ratings yet
- AMX-3 Prom AdaptorDocument18 pagesAMX-3 Prom AdaptorEmmanuel RamirezNo ratings yet
- The Remains of The Day-Excerpts-1Document2 pagesThe Remains of The Day-Excerpts-1DajanaNo ratings yet
- Indian Standard: Hexagon Head Bolts, Screws and Nuts of Product Grades A and BDocument11 pagesIndian Standard: Hexagon Head Bolts, Screws and Nuts of Product Grades A and BJignesh TrivediNo ratings yet
- AmpConectorsExtracto PDFDocument5 pagesAmpConectorsExtracto PDFAdrian AvilesNo ratings yet
- Concept Deck de BosBoerderij - Dec2023Document32 pagesConcept Deck de BosBoerderij - Dec2023Bruna San RomanNo ratings yet
- Microsoft PowerPoint Presentation IFRSDocument27 pagesMicrosoft PowerPoint Presentation IFRSSwati SharmaNo ratings yet
- BV14 Butterfly ValveDocument6 pagesBV14 Butterfly ValveFAIYAZ AHMEDNo ratings yet
- ICT Backup Procedure PolicyDocument8 pagesICT Backup Procedure PolicySultan BatoorNo ratings yet
- Investors' Perceptions of StocksDocument95 pagesInvestors' Perceptions of StocksPriya Ramanathan67% (3)
- Link L5 Assessment AKDocument11 pagesLink L5 Assessment AKJoanna MajczykNo ratings yet
- Communication Thesis PDFDocument2 pagesCommunication Thesis PDFBarbara0% (2)
- Modern Pharmacy Layout TrendsDocument9 pagesModern Pharmacy Layout TrendsRaheem KhanNo ratings yet