You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Student Clinical Report SheetDocument2 pagesStudent Clinical Report SheetMike100% (4)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Brain 3Document3 pagesBrain 3Nurse Betty100% (1)
- Clinical Experience "Tips"Document5 pagesClinical Experience "Tips"ashdmb217No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Room: - Name: - Code Status: - AllergiesDocument2 pagesRoom: - Name: - Code Status: - Allergiesashdmb217No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Maxwell Quick Medical Reference PDFDocument35 pagesMaxwell Quick Medical Reference PDFAnonymous fj68Ms100% (10)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Room: - Name: - Code Status: - AllergiesDocument2 pagesRoom: - Name: - Code Status: - Allergiesashdmb217No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Information Regarding Family History DocumentDocument9 pagesInformation Regarding Family History Documentashdmb217No ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Nursing Management of The Perioperative PatientDocument16 pagesNursing Management of The Perioperative Patientashdmb217No ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Nurse Brain Sheet Telemetry Unit SBARDocument1 pageNurse Brain Sheet Telemetry Unit SBARashdmb217No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- SymbolsDocument1 pageSymbolsashdmb217No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Useful Spanish Words and PhrasesDocument32 pagesUseful Spanish Words and Phrasesashdmb217No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Exam 3 PathwaysDocument1 pageExam 3 Pathwaysashdmb217No ratings yet
- Adventitious Breath SoundsDocument1 pageAdventitious Breath Soundsashdmb217No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Medical TerminologyDocument13 pagesMedical Terminologyashdmb217No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Histology Exam 3 ReviewDocument7 pagesHistology Exam 3 Reviewashdmb217No ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- AbbreviationsDocument5 pagesAbbreviationsashdmb217No ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- HCP FormDocument8 pagesHCP FormMarkNo ratings yet
- Nutrition Review1.2Document12 pagesNutrition Review1.2ashdmb217No ratings yet
- Vitamin Chart.2Document3 pagesVitamin Chart.2ashdmb217No ratings yet
- Critical Care PhysiologyDocument287 pagesCritical Care Physiologyashdmb217100% (7)
- Histology Exam 2 Review.1Document18 pagesHistology Exam 2 Review.1ashdmb217No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Histology Exam IV Review Part 2Document26 pagesHistology Exam IV Review Part 2ashdmb217No ratings yet
- Histology Exam IV Review Part 1Document36 pagesHistology Exam IV Review Part 1ashdmb217No ratings yet
- Starting Out - New in The ICUDocument30 pagesStarting Out - New in The ICUashdmb217100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Nutrition Review 2.3Document10 pagesNutrition Review 2.3ashdmb217No ratings yet
- Exam 4 PathwaysDocument1 pageExam 4 Pathwaysashdmb217No ratings yet
- Exam IV ReviewDocument39 pagesExam IV Reviewashdmb217No ratings yet
- Biochem Exam 2 Review.2Document31 pagesBiochem Exam 2 Review.2ashdmb217No ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
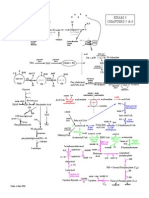
- Exam 1 Study Guide.2Document52 pagesExam 1 Study Guide.2ashdmb217No ratings yet
- Biochem Exam III Review.2Document24 pagesBiochem Exam III Review.2ashdmb217No ratings yet
- 12 Physiology of Autonomic Nervous SystemDocument39 pages12 Physiology of Autonomic Nervous SystemVinod SharmaNo ratings yet
- 2 AnsDocument97 pages2 AnsMahmoud AboudNo ratings yet
- (Netter) Atlas of Human Anatomy. 8° (2023) - 3Document13 pages(Netter) Atlas of Human Anatomy. 8° (2023) - 3ALEXIS SEDERAPNo ratings yet
- Gastrointestinal System: Git Brief Introduction: Dr. S. M. A. WaseemDocument20 pagesGastrointestinal System: Git Brief Introduction: Dr. S. M. A. WaseemHoping HeartsNo ratings yet
- Anatomy of The Facial NerveDocument75 pagesAnatomy of The Facial NerveRao Rizwan Shakoor100% (1)
- Chap-21 Neural Control and CordinationDocument48 pagesChap-21 Neural Control and CordinationMANIK CHHABRANo ratings yet
- Psych Notes - Clinical Pocket GuideDocument242 pagesPsych Notes - Clinical Pocket Guidevroux100% (1)
- Anatomy - Head and Neck Table of NervesDocument11 pagesAnatomy - Head and Neck Table of NervesIke Ononiwu100% (3)
- 3 Minutes To Neurologic Harmony 2020Document22 pages3 Minutes To Neurologic Harmony 2020anon_82154430No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Anatomy & Physiology Ansci Q&ADocument13 pagesAnatomy & Physiology Ansci Q&AJoylyn TroniadoNo ratings yet
- Spinal Manual 20 August 2004Document235 pagesSpinal Manual 20 August 2004Forum PompieriiNo ratings yet
- 3 Physiology Notes PDFDocument119 pages3 Physiology Notes PDFshiningdream100% (1)
- Cholinergic DrugsDocument44 pagesCholinergic Drugskhuzaima9100% (1)
- Chapter 7 - Autonomic Nervous SystemDocument12 pagesChapter 7 - Autonomic Nervous Systemmichael3vo-1No ratings yet
- Bisc 305 Practice Questions PhysiologyDocument1 pageBisc 305 Practice Questions PhysiologyAman BassiNo ratings yet
- Primal Hormones - Made by Aesthetic Primal 1Document59 pagesPrimal Hormones - Made by Aesthetic Primal 1Levi Ackermann100% (3)
- Head Neck MCQ ChaptersDocument17 pagesHead Neck MCQ ChaptersMohamed GhabrunNo ratings yet
- Neuromuscular Physical TherapyDocument13 pagesNeuromuscular Physical Therapypearl042008100% (3)
- AP Psychology Unit 3 Test Study GuideDocument27 pagesAP Psychology Unit 3 Test Study Guide(Albert) Minkyu KimNo ratings yet
- Test Bank For Essentials of Psychology 7th Edition Douglas A BernsteinDocument31 pagesTest Bank For Essentials of Psychology 7th Edition Douglas A Bernsteinpearloanhrl4iNo ratings yet
- DIGESTIVE Lecture Notes PDFDocument20 pagesDIGESTIVE Lecture Notes PDFAaliya Minar100% (4)
- To Autonomic Pharmacology: Anatomy of The Autonomic Nervous System: Sympathetic and Parasympathetic DivisionsDocument154 pagesTo Autonomic Pharmacology: Anatomy of The Autonomic Nervous System: Sympathetic and Parasympathetic DivisionsLycan AsaleNo ratings yet
- Neurological System Assessment Part 1 - NCM 101 H.ADocument5 pagesNeurological System Assessment Part 1 - NCM 101 H.ALexie KepnerNo ratings yet
- Nervous System ReviewerDocument4 pagesNervous System ReviewerSophia CaisipNo ratings yet
- Pex 06 02Document4 pagesPex 06 02Jihan FadillaNo ratings yet
- Aqa Byb4 W QP Jan08 PDFDocument20 pagesAqa Byb4 W QP Jan08 PDFCindyVortexNo ratings yet
- Total Health Through Rhythmic BreathingDocument64 pagesTotal Health Through Rhythmic Breathingkishor827100% (3)
- Autonomic Nervous System AnatomyDocument10 pagesAutonomic Nervous System AnatomyghalyNo ratings yet
- Al-Azhar University Faculty of Medicine: Thanks ToDocument20 pagesAl-Azhar University Faculty of Medicine: Thanks TogopscharanNo ratings yet