Professional Documents
Culture Documents
Pathophysiology of Endocrine System
Uploaded by
Ahmad Abu KushOriginal Description:
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Pathophysiology of Endocrine System
Uploaded by
Ahmad Abu KushCopyright:
Available Formats
Disorders of Endocrine Control of Growth and Metabolism
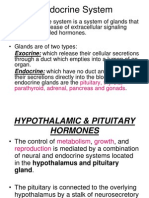
The endocrine system affects all aspects of body function, including growth and development, energy metabolism, muscle and adipose tissue distribution, sexual development, fluid and electrolyte balance, and inflammation and immune responses. Hypo function and Hyper function Disturbances of endocrine function usually can be divided into two categories: hypo function and hyper function. Hypo function of an endocrine gland can occur for a variety of reasons : 1. Congenital defects can result in the absence or impaired development of the gland or the absence of an enzyme needed for hormone synthesis. . !c"uired defects may occur in the result of gland destroying by a disruption in blood flow, infection, inflammation, autoimmune responses, or neoplastic growth. There may be a decline in function with aging, or the gland may atrophy as the result of drug therapy of un#nown reasons. $. %ndocrine&deficient states associated with receptor defects: hormone receptors may be absent, the receptor binding of hormones may be defective , or the cellular responsiveness to the hormone may be impaired. '. %ndocrine disorders binding with biologically inactive hormone or that an active hormone may be destroyed by circulating antibodies before it can exert its action. Hyper function usually is associated with excessive hormone production. This can result from excessive stimulation and hyperplasia of the endocrine gland or from a hormone&producing tumor. ! tumor can produce hormones that are not normally secreted by the tissue from which the tumor is derived (so&called ectopic hormone production)* for example, certain bronchogenic tumors produce hormones such as antidiuretic hormone (!D+) and adrenocorticotropic hormone (!CT+). Primary, Secondary, and Tertiary Disorders %ndocrine disorders in general can be divided into primary, secondary, and tertiary groups. Primary defects in endocrine function originate in the target gland responsible for producing the hormone. ,or example, total thyroidectomy produces a primary deficiency of thyroid hormones. -n secondary disorders of endocrine function, the target gland is essentially normal, but its function is altered by defective levels of stimulating hormones or releasing factors from pituitary system. e..g. .emoval or destruction of the pituitary gland eliminates !CT+ stimulation of the adrenal cortex and brings about a secondary deficiency. ! tertiary disorders results from hypothalamic dysfunction ( as may occur with craniopharyngiomas or cerebral irradiation)* thus, both the pituitary and target organ are understimulated. Physiopathology of pituitary and growth disorders
The pituitary gland has two components: a posterior lobe (neurohypophysis) or neural component and an anterior lobe (adenohypophysis ) or glandular component. The anterior lobe of the pituitary gland produces !CT+, thyroid stimulating hormone (T/+), growth hormone (0+) , the gonadotrophic hormones ( follicle stimulating hormone 1,/+ 2and liteinizing hormone 13+2, and prolactin. ,our of these, !CT+, T/+, 3+, and ,/+ control the secretion of hormones from other endocrine glands. !CT+ controls the release of cortisol from the adrenal gland, T/+ the secretion of thyroid hormone from the thyroid gland, 3+ regulates sex hormones and ,/+ regulates fertility.
Pituitary Tumors
4ituitary tumors can be divided into primary or secondary tumors (i.e., metastatic lesions). Tumors of the pituitary can be divided into functional tumors that secrete pituitary hormones and nonfunctional tumors that do not secrete hormones. 5enign adenomas account for most of the functioning anterior pituitary tumors. Carcinomas of the pituitary are less common tumors. ,unctional adenomas can be subdivided according to cell type and the type of hormone secreted. Table . !re"uency of #denomas of the #nterior Pituitary Cell Type 3actotrope /omatotrope 3actotrope6somatotrope Corticotrope 0onadotrope Hormone 4rolactin (4.3) 0rowth hormone (0+) 7ixed 4.360+ !drenocorticotropic hormone (!CT+) ,ollicle&stimulating hormone (,/+) 3uteinizing hormone (3+) Thyroid :stimulating hormone ( T/+) !re"uency $%& $ 1 8 1$ 9'
Thyrotrope ;onfunctional tumors
9' <
Hypopituitarism
+ypopituitarism, which is characterized by a decreased secretion of pituitary hormones, is a condition that affects many of other endocrine systems. Typically, =>? to @>? of the anterior pituitary must be destroyed before hypo pituitarism becomes clinically evident. The cause may be congenital or result from a variety of ac"uired abnormalities. The manifestations of hypopituitarism usually occur gradually, but it can present as an acute and life&threatening
condition. 4atient usually complain of being chronically unfit, with wea#ness, fatigue, loss of appetite, impairment of sexual function, and cold intolerance. !CT+ deficiency ( secondary adrenal insufficiency) is the most serious endocrine deficiency, leading to wea#ness, nausea, anorexia, fever, and postural hypotension. +ypopituitarism is associated with increased morbidity and mortality. Hypo' and hypersecretion of growth hormone $GH& 0+ is produced by somatotropes in the anterior pituitary, is necessary for linear bone growth in children. -t also increases the rate at which cells transport amino acids across their cell membranes, and it increases the rate at which they utilize fatty acids and decrease the rate at which they use carbohydrates. The effects of 0+ on linear growth re"uires insulin&li#e growth factors (-0,s), which are produced mainly by the liver. 0+ deficiency in children interferes with linear bone growth, resulting in short stature or dwarfism. -n children, 0+ excess results in increased linear growth or gigantism* in adults it results in overfrowth of the cartilaginous parts of the s#eleton, enlargement of the heart and other organs, and metabolic disturbances in fat and carbohydrate metabolism. 0rowth hormone (0+, somatotropin) : is a hormone that has proteic nature, secreted by acidophile cells of 5ecause of its proteic structure, 0+ has a spece specificity, this is why 0+ extracted from animalAs pineal gland is not efficient for substitutive therapy of hormonal insufficiency at humans. Bnly human somatotropin or the one obtained through genic engineering has a therapeutical effect at humans. Cntil 1@D<, the therapy of 0+ insufficiency was made with extract from human pineal gland. !fter that, somatotropine derived from recombinated D;! became accesible, a source limited only by the high price of the preparation. The substitutive therapy with 0+ began at children is continued until the growth is finished or until the moment when antropometric normal index are achieved. The settlement of 0+ secretion is made through many ways by neurotransmitters which modulate the hypothalamic secretion of somatoliberine (0+& releasing hormone, 0+.+ ) and somatostatine (//). !fter separation and clonning of receptors for 0+.+ and somatostatine the neurosettlement of 0+ secretion was detailed studied. -t was established that 0+.+ attaches to specific receptors from the membrane of pineal somatotropes and stimulates the 0+ secretion through intracellular mechanisms c!74 and Ca E&depending. /omatostatine attaches to a family of specific receptors (//&receptors, //&.) Bn the membrane of pineal somatotropes, inhibits the adenilatciclase, with the reduction of calcium influx and secretion (but not the synthesis) of 0+. //&. are expressed not only in somatotrope cells of pineal gland, but also in hypothalamic cells, where these one modulate the secretion of // and 0+.+. /o, the infusion of somatostatine at young men diminishes the amplitude and
fre"uency of 0+ secretion, this demonstrates that somatostatine inhibits not only the 0+ secretion, but also the 0+.+ secretion. The transport of somatoliberine and somatostatine from neurosecretting hypothalamic nucleus to the pineal gland is made through the portal pineal system, its capilaries surround the acidophile cells of , and the 0+ transport to the target peropherical structures is made through blood systemical circulation. /ecretion of 0+ is pulse& li#e, mostly at night hours, this is why the hormoneAs concentration during the day is low. Contemporary methods of measuring (immunofluorimetric and chemiluminiscent) with the performance of >.>1$ Fg6 liter had descovered an inferior basic level of 0+ secretion (for about >.> >& >.>< Fg6 liter) and the pulse&li#e secretion depending on the sex. The pitch of secretion at adults and children varies in limits of 1 <& <> times. These are the reasons why for the tracing of insufficiency of 0+ is used the artificial stimulation of hormonal secretion. The first proposed provocative test was the insulinic hypoglicaemia (insulinic tolerance). Gith the help of this test itAs possible to estimate at the same time and the secretory function of adrenal& !CT+ axle. Bther pharmacological stimuli are 3&DB4!, arginine, glucagone, propranolol, clonitidine. ! supplementary procedure for differentiation of 0+ insufficiency and constitutional delay consist in sensibilisation of organism with steroids, by administration, a few days before of steroids. !t healthy children in puberty period there is a considerable growth of amplitude of 0+ secretion caused directly by the increasing of sexual steroidAs concentration. ;owadays, neuroendocrinological investigations operate with methods of indetification, measuring and cuantification of amplitude, duration and area of 0+ secretion. The concentrationAs profile of 0+ in blood during ' hours is characterized by short, regulated, pulsi&li#e waves. Ghen the endogen secretion of 0+.+ increases, there is an explosive secretion of 0+ . The blood test investigation, every $> seconds during the sleep, at young people, established a tight correlation between episodical secretion of 0+ and the beginning of slow& wave sleep. -t should be mentioned that at patients with renal and hepatic disfunctions it was found the increasing of 0+ half&period in blood, in obesity& its decreasing. /exual steroids (estradiol and testosterone) amplificate the pulse&li#e secretion of 0+ and reduce the regularity of secretion in prepubertal period. The loss of 0+ secretionAs regularity is evident in acromegalia, in tumours secreting !CT+. 0+ secretion varies during the personAs life. -n first hours after birth the 0+ secretion is explosive and outruns the secretion calculated at area unity in aduls. The situation of 0+ hypersecretion in neonatal period is typical for states with 0+&resistance (inanition, chronic renal and hepatic diseases, diabetes type 1, congestive cardiac insufficiency). 5efore puberty, the pulse&li#e secretion of 0+ during ' hours is stable ( >>& 8>> Fg6day) and approximately is e"ual with the secretion in post&puberty. Bnce the biochemical and clinical manifestations of sexual steroidsAincreasing is
started at boys and girls, there is a 1.<& $ times increasing of 0+ secretion. The maximum level is recorded in late period puberty 1& 1.D Fg6 ' hours. !t grown persons, the 0+ secretion decreases until <& <> ? from post& pubertal secretion and constitutes about 1<& 1>> Fg6day. The lowest level is recorded at old and obese persons, in hypothyroidism and diabetes type --. The decreasing of 0+ secretion parallel with age constitutes about 1'? per ten years, recent studies shows that at some old subHects 0+ secretion is completely suspended. The normal ageing is associated with changings in composition of human body, similar to those that accompany the 0+ defficiency: reduction of bones mass, osteoporosis, reduction of cardiac and renal functions. The decline of 0+ secretion and morpho& physiological changings at old persons are #nown as somatopause. The mechanism of progresive decline of hypothalamo& somatotrope axis functions at healthy old persons is not #nown, but the similarity of changings in organism in case of somatotropic insufficiency, with those in ageing leads to the conclusion that ageing is related with 0+ defficiency. (iological effects of GH . Cnli#e other pineal hormones from tropine& group (tireotropine, corticotropine, gonadotropines) that action through peripherical endocrine glands, the 0+ action on peripherical target& cells is made directly, without the help of peripherical endocrine glands. -t is considered that 0+ effects of stimulation on the growth is due to the stimulation of synthesis in liver and other peripherical tissues of some specific substances insuline& li#e and called somatomedines or -0, (insuline li#e growth factor). -0, is a peptide 0+& depended, that mediates the maHority of metabolical actions and mitogene actions of 0+. The peripherical target&cells, receptive to 0+ actions, have specifical receptors for this hormone&especially chondroblasts and osteoblasts. 4eripherical action of 0+ is manifested by metabolic and organogenetic effects. 7etabolic actions of 0+ are diverse and bivalent. 7etabolic action on proteic metabolism is manifested by stimulation of aminoacid transport from blood in cells, by stimulation of proteic synthesis from aminoacid. The catabolic effect of 0+ assures the material and energetical basis for the proteinAs synthesis and consists in stimulation of glicogenolisis with hyperglicaemia (antiinsulinic, diabetogenic effects), stimulation of lipolisis with hyperlipidaemia of transport, stimulation of cetogenesis with hypercetonaemia. Brganogenetic effects are chondrogenesis, osteogenesis, miogenesis and viscerogenesis. 4rimary diseases of hypothalamus and pineal gland(for ex. tumours) generate an excesive secretion or defficiency of 0+, and peripherical effects of 0+ or of insuline&li#e growth factor on target& structures. Hyposecretion of somatotrope hormone Ethiology)!s ethiological factors of hyposecretion of somatotrope hormone serve different pathological processes at hypothalamic and pituitary levels: disturbances of licvorodynamics with hydrocephalus, neuroinfections, intoxications, trauma, tumourous processes, surgical interventions and
radiotherapy of the region. -t should be mentioned that 0+ is the first adenopineal hormone, its secretion is disturbed in vasculo&cerebral accidents. Clinical studies by using ultrasensitive methods had shown that visceral obesity, age and other states can lead to an increased secretion of 0+. Clinical and biochemical manifestations (metabolic and organogenetic) of 0+ secretionAs insufficiency are specifical for the age when they appeared. 0+ defficiency at adults and the abolishment of metabolic and organogenetic actions of 0+ are translated by the growth of adipose tissue mass, especially distributed in trun# region (abolishment of lipolitical function), by hypoglicaemia (because of loss of glicogenolitic function), intolerance of glucose and resistance at insuline (0+ stimulates the glucose use by cells), modification of lipidogramm(insufficiency of fat non& estheric acids because of the abolishment of lipid mobilization function), resorbtion and atrophy of bones& osteopenia(abolishment of osteogenetic functions), hypotrophy of intern organs(abolishment of viscerogenetic function), hypotrophy of conHuctive tissue, alteration of cardiac structure and function, reduction of muscular mass and of physical performance (abolishment of miogenetic and viscerogenetic function), and as a result of it :reduction of lifeAs "uality. !t the same time with different metabolic manifestations, patognomic symptoms for 0+ defficiency are lac#ing, the only specific test is the estimation of hormoneAs secretion. ,or many years, the tolerance at insuline (insuline tolerance test, -TT) was the golden standard in the diagnosis of 0+ defficiency. ;owadays, from the hall number of provocative& tests existing (glucagone, arginine, -TT and hypoglicaemia induced by tolbutamide), the glucagone&test is considered the best. 0+ insufficiency at children, at the same time with specific metabolic disturbances for 0+ insufficiency, is manifested by disturbance of chondroosteogenesis with retardation of growth: +ypersecretion of 0+ at adults is more fre"uently related to hypophisaryI adenom from eosinophile somatotrope secretting cells and is manifested by metabolic and morphogenetic disturbances. 7etabolic disturbances mediated by the somatotropineAs excess are: intensification of proteic synthesis by stimulation of sulphatesAadding in proteoglicanes of bones and cartilages and of timidine in D;!, intensification of .;! synthesis and simple proteins. !t the same time there is the inhibitions of proteolisis and a positive nitric balance. 0lucidic metabolism is characterized by the intensification of glucagone and insuline secretion, at the same time with stimulation of hepatic insulinase, glicogenolisis, with stopping of peripherical use of glucose, with hyperglicaemia, glucosuria. /omatotropina has a permisive action for insuline and glucocorticoids.This is why, small doses of 0+ contribute to anabolism, high doses to catabolism. !s a result, disturbances of glucidic metabolism constitute the picture of insulinoresistant diabetes. 3ipidic metabolism is characterized by the intensification of lipolisis and transport hyperlipidaemia with fat non& estheric acids.
%xcesive morphogenetic action of 0+ is manifested at adults through acromegalia: somatic deformed growth of s#eleton of the extremities, that still have at this age a growing potential (firger phalangs, facial s#eleton) and splanchnomegalia: dimensional growth of intern organs. +ypersecretion of somatotropine at children is traduced through gigantism& somatic excesive growth, but proportional, in association with specific metabolic manifestations for 0+. Hypo' and hypersecretion of adrenocorticotrope hormone !drenocorticotrope hormone (!CT+) is a polypeptide ($@ radicals of aminoacids) secreted by basophile cells of adenopineal gland. The main action of !CT+ consists in stimulation of synthesis and secretion of glucocorticoids of adrenal glands and proliferative activity of fasciculated and reticulated stratum of adrenal cortex. The synthesis and secretion of !CT+ is controled directly by corticoliberine (C.,& corticotropin releasing factor), secreted by neurosecreting hypothalamic nucleus (especially basal hypothalamus, median eminence) and under the retrocontrole (feed& bas#) negativ of pineal !CT+ and adrenal hydrocortisone. !t the same time with corticotrope action, !CT+ has a directly somatotrope action: contributes to lipidic mobilization from depots and their oxidation, intensifies #etogenesis, contributes to glicogenolisis in liver and the storing of glicogen in muscles, the intracellular adding of aminoacids. !CT+, also, intensifies the steroidsA degradation in liver and stimulates melanophores, contributing to the s#inAs pigmentation. -nsufficiency of !CT+ conducts6 leads to the hypoplasia of adrenal glands and a secondary secretory insufficiency of glucocorticoids. +ypersecretion of !CT+ leads to the hyperplasia of cortical adrenal glands and secondary hypersecretion of glucocorticoids. Bther manifestations of hypersecretion of !CT+ are related to metabolic effects mediated directly by !CT+ (extraadrenal action)& activation of thyrosinase from melanocytes and intensification of melanineAs synthesis and s#inAs hyperpigmentation, lipolisis, hyperlipidaemia with fat non& estheric acids. !CT+ effects mediated by glucocorticoidsA hypersecretion (transadrenal action) consists in inhibition of lipolisis, activation of gluconeogenesis and lipogenesis. Hypo' and hypersecretion of thyreotropine hormone T/+ or thyreotropine is a glicoprotein secreted by basophile cells of adenopineal gland. /ecretion of T/+ is controled directly by tireoliberine secreted from hypothalamic neurosecreting cells and by negative feed& bas# based on plasmatic concentration of thyroid hormones. -n direct ways the secretion of T/+ is stimulated, or inhibited by cold or heat, by different #inds of stress. T/+ leads to the proliferation of follicular cells of thyroid glands, intensifies the blood perfusion of the gland, increases the use of oxygen and glucose, stimulates the capture of circulating iodine by thyroid gland, the transforming of molecular iodine in atomic iodine and association of
iodine at tirosine, increases the biosynthesis of thyroid hormones, proteolisis of thyreoglobulin and consecutive the secretion of thyroxine and triiiodthyronine. +ypersecretion of T/+ is a conse"uence of basophil pineal adenom. T/+ leads to hyperplasia and stimulating of thyroid function secondary (hyperthyroidism). -t should be mentioned that the primary hypersecretion of thyroid gland, caused by pathological processes localized in thyroid& for ex. a tumour& is associated with hyposecretion of T/+. +yposecretion of T/+ leads to secundary insufficiency of thyroid. Hypo' and hypersecretion of gonadotrope hormones ,olliculostimulating hormone (,/+), secreted by basophile adenopineal cells is a glicoprotein with the molecular mass about $>>>>. !t women it stimulates the maturring of 0raaf follicles, at men& spermatogenesis. +yposecretion of ,/+ at women is associated with las# of growth and maturring of primordial follicles in ovaries and consecutively leads to infertility. %xogen administration of ,/+ leads to maturity of a big number of ovarian follicles(ovarian hypersecretion). +yposecretion of ,/+ at men leads to the inhibition of spermatogenesis and consecutively to oligozoospermia with sterility. 3uteinisant hormone (3+) is a glicoprotein secreted by basophile adenopineal cells. !t women 3+ stimulates the secretion of estrogens, produces the brea#ing of a mature 0raaf follicle (ovulation) and luteinic transformation of the follicle after the ovulation. !t men 3+ stimulates the secretion of adrogens by interstitial 3eydig cells and it is also called the interstitial cells stimulating hormone (-C/+). +yposecretion of 3+ at women has specific effects, directly related to menstrual cycleAs phases. The basal hyposecretion of 3+ leads to hypoestrogenia, the las# of eruptive secretion of 3+ in the middle of menstrual cycle ma#es impossible the ovulation of the mature follicle and also, the sterility. +yposecretion of 3+ at men has as conse"uence the hyposecretion of testosterone& hypoandrogenia with all the specific conse"uences. The lactotrop hormone (3T+, lactogen hormone, prolactine) is secreted by eosinophile cells of adenopineal gland and represents a polypeptide made of 1@D aminoacids. 3T+ mentains the progesteronAs secretion by the yellow gestant body. 3T+ influences the lactogene activity of mamar gland, prepared preliminary for lactation by estrogenes. 3T+ function at men is un#nown for sure. -t is supposed its role in prostateAs growth. +ypersecretion of 3T+ (hyperprolactinaemia) is a conse"uence of pineal adenom and it is manifested at women by lactorrhea, amenorhea and sterility, at men : hypoandrogenia, inhibition of spermatogenesis, gynaecomastia. Physiopathology of adrenal glands !drenal glands are made of two parts: cortical and medullar. Cortical part has three distinct zones: glomerular, fascicular, reticular, which secrete three groups
of hormones: mineralocorticoids (principally aldosteron), which function in sodium, potassium, and water balance* the glucocorticoids (principally cortisol), which aid in regulating the metabolic functions of the body and in controlling the inflammatory response, and are essential for survival in stress situations* the adrenal sex hormones (principally androgens), which serve mainly as a source of androgens for women . 7ineralocorticoids are represented predominantly by aldosterone. !ldosterone, secreted in blood is bonded to a alpha& &globuline and transported to #idneys, where it influences the resorbtion of sodium in distal contort tubes. !t the same time, sodium ions are resorbed with chloral ions, bicarbonate ions and it is increased the secretion of potasium and hydrogen ions. This effect is manifested also in salivary, gastric glands. The indirect effect of mineralocorticosteroids is translated by the increasing of arterioli tonus, with hypertensive effect. The degradation of aldosterone is made in liver by conHugation and forming glucuronic compounds. 0lucocorticoids (0C) are synthetyzed in fascicular6reticular zones of adrenal cortex and are liberated in blood& circulation as an answer to a big number of stressing stimuli(inanition, pain, surgical interventions, emotions, extremal temperatures, cellular lesions). The liberation is controled by hypothalamic&pineal&adrenal axis (+4!), where C.+ actions on pineal gland, causing the liberation of !CT+, and !CT+ stimulates the adrenal gland in liberation of glucocorticoids. 0lucocorticoids have vital functions, without them the organism can not survive. 0C (at man, the main is cortisole, the day secretion of it is about 1 mg * cortisone has about 1<? from total secretion), controle the glucidic metabolisms, the proteic and lipidic ones * contributes to the absorbtion of glucides from intestines, stimulates neoglucogenesis in liver, #idneys, s#eletic muscles, inhibits the peripherical use of glucose, causing hyperglicaemia, intensifies lipolisis, #etogenesis, but also, at the same time, contributes at deposing the fats in selective regions of subcutaneous adipose stratum, stimulates the synthesis of proteins in liver and at the same time intensify the proteolisis, causing cytolisis and atrophy (involution) of timus, lymphoid tissue, conHuctive tissue with lymphocytopenia, eosinopenia, immunosuppression and antiinflammatory effect, modulates bonesA turnover with osteopenia (osteoporosis) . ! prominent effect of glucocorticoids is neoglucogenesis &the synthesis of glucose from aminoacids. Due to the stimulation of catecolamines synthesis and the permisive effects for them, 0C have a cardiotrope positive effect and participate in maintaining the blood pressure. 0C have many effects, which are manifested in stressing conditions or at prolonged action: 1. !ntiinflammatory effect, seen as stabilizing on cell membranes:cytoplasmatic and of organits (especially lisosomal), inhibition of histamineAs liberation, serotonineAs liberation, inhibition
of prostoglandinesA and #ininesA synthesis, inhibition of cellular adhesion and of complementAs system, inhibition of leucocytesAmigration into inflammatory focus. . !ntialergic and immunosupresive effect depends on antiinflammatory effect and on involution of lymphoid tissue of timic gland, on lymphocytolysis and lymphocytopaenia. $. !ntiproliferative effect on fibroblasts, antifibrogenetic ( inhibits the synthesis of colagenI) and antiregenerative effects, which can hinder the reparation of tissular deffects. '. 4eptic effects& stimulation of pepsine secretion and of chlorous acid, which at the same time with other antigastroprotective effects ( inhibition of regeneration of the mucous stratum) may contribute to ulcerogenesis. The importance of 0C in metabolismAs regulation is evident in Jmetabolic syndromeK, caused, at least, by the hypersensitivity for cortisole. The syndrome includes a collection of metabolic disorders& obesity, hyperlipidaemia, hyperinsulinaemia, insulinic resistance, arterial hypertension. !poptosis of immun cells, also, is a process controled by 0C. There is an effect of 0C on central nervous system, it is not clear yet. 0C have a deep effect on fetal development, especially of fetal lungs and parturition. .eticular zone synthetizes, secrets androgen hormones (dehydroepiandrosterone), vestigial cantities of estrogens and progestines. !ndrogen hormones influence the development of primary and secondary sexual characters at men, have an anabolic effect& stimulate the synthesis of proteins in muscles. 5iological activities of 0C are evident in different periods of ontogenetic development and in different physiological states. -n this conditions have a certain manifestation the insufficiency or the excess of 0C. The role of adrenal glands in antenatal ontogenesis !t primates and at man, during de last 6$ds of pregnancy, the adrenal gland is disproportional big and demonstrates a rising and a extraordinary steroidgenetic activity in a special zone called foetal zone. !fter birth, foetal zone involuates rapidly even in the presence of corticotropine, which is the physiological regulator of steroid secretion of foetal cortex. 4robably, foetal zone is regulated not by the pineal corticotropine, but of the placentary corticotropine and autoregulated by some growth factors, secreted locally, by fetal adrenal glands. -n antenatal period the vital importance of steroid hormones producted by the adrenal foetal cortex, consist in regulation of hormonal intrauterine homeostasis, maturation of foetal organs and their preparation fot the postnatal life, initiation of parturition, production of gluco& and mineralocorticoids, which assure the autonomy of the foetus after his separation from the placenta. The monitoring of gestation) -t is #nown the physiological antagonism of estrogens and progesterone in their action on the uterus. -n this way, gestation is assured by the high concentration of progestines and minimum of estrogens, but parturition& the diminishing of progesteroneAs
concentration at the end of pregnancy and the stimulation of estrogensAsecretion in uterus. 5ecause the synthesis of placentary estrogens necesarry fot parturition is assured in co&operation with adrenal foetal glands, the role of fetal adrenal glands in parturition becomes clear. -n the middle of gestation, foetal zone is about D>& @>? from the total cortical volume and produces 1>>& >> mg of androgenic steroid C1@ (dehydroepiandrosteron), which "uantitatively is the main steroid of the adrenal foetal cortex.(,oetal cortex produces and cortisole, that promovates the maturation of foetal organs, including lungs, thyroid gland, intestines). /teroid C1@ is a source for the placentar synthesis of estrogens. -t was proved that steroid C1@ is synthetized only in the foetal zone of the adrenal foetal gland (placenta can not synthetize it from pregnelone or progesterone because of the las# of the enzyme, but it can synthetize estrogens from steroid C1@). -n the third part of gestation, adrenal foetal cortex expresses a high level of an enzyme (4'/BC1=) and produces high "uantities of steroids. The combination of this two biosynthetics ways in this two organs& adrenal cortex (that synthetizes the steroid C1@ ) and placenta (it synthetizes estrogens from steroid C1@ ) completes it self and forms an integral system of estrogensA synthezis. The role of foetal cortex is to assure the placenta with steroid C1@ necesarry fot the synthesis of estrogens, forming the uni"ue foeto& placentary system. The synchroni*ation of foetal maturation with the beginning of parturition -s crucial for the postnatal survival of the new& born. -t was demonstrated that the growth of activity of hypothalamic&pineal&adrenal foetal axis not only gives a start to parturition (trigger), but at the same time stimulates the maturation of foetal organs for extrauterine life. !t men, the growth of cortisoleAs secretion from foetal adrenal glands in the final wee# of gestation initiates the cascade of culminating processes of birth. Cortisole stimulates the processes associated with the preparation for extrauterine life of foetus& production of surfactant from foetal lungs, activation of foetal intestinal enzymes, enzymes from retina, pancreas, thyroid gland and brain, the storing of glicogene in liver. -n this way the postnatal survival depends on the sufficient maturation of the organs, permitting the new& born the extrauterine life and independed life from the placenta. The initiation of the parturition) !t the end of gestation during the time when adrenal foetal cortex synthetizes intensively steroids C1@, placenta synthetizes a lot of estrogens. !t the same time, the involution of yellow body leads to the diminishing of progesteroneAs synthesis. The growth of estrogensA concentration and the diminishing of progesteroneAs concentration at the end of pregnancy, is indispensable for the determination of the moment of parturition at the maHority of biological speces. -t is considered that C.+ (corticotropine realising hormone) serves as a Jcloc#K, that participates in the determination of gestationAs lenght and the moment of parturition, by its direct effects and those mediated by cortisole it participates to the delivrating process itself. 5esides the hypothalamus,
corticoliberine is synthetized by the placenta. /tarting with the D th wee# of gestation and until delivery, the concentration of C.+ rises suddenly in the peripherical circulation (foetal and maternae). -t was established, also, that unli#e the negative hypothalamic feed& bas# on C.+ secretion, in human placenta glucocorticoids rise the secretion of C.+ positive (feed& bas#). /o, on the eve of parturition the concentration of C.+ rises in the placentary circulation, this leads to a high production of foetal glucocorticoids, and these ones lead to delivery. Datum about the presence in miometrum and foetal membranes of receptors for C.+, stimulation of 40, liberation from decidua and human amnios in vitro by C.+, the potention of 40, and oxitocyne by C.+ in vitro and in vivo, sustain the concept that, at the same time with cortisole, C.+ regulates directly human parturition, increasing the contractibility of miometrum in birth. The concentration of C.+ in maternal plasma is predicative for women that will have a delivery on time, prematurely or postterm. /o, the curve of secretion of C.+ at women that gave birth prematurely has a maximum in early periods of pregnancy. !t women that gave birth post term, the secretion of C.+ has a maximum in late periods of pregnancy, it corresponded to the observed postmaturity. !fter the birth of foetus, the maHor physiological role of cortisole from adrenal cortex is the assurance with glucocorticoids, that mentain the metabolic homeostasis and the answer to a stress* and with mineralocorticoids, that mentain the hydric and electrolitic e"uilibrium. -t should be mentioned that, although these functions in the foetal period are affected by placentary steroids, at primates foetal axis hypothalamus& pineal gland& adrenal gland is able to answer to a stress by increasing the production of cortisole, li#e the answer in the postnatal period, and in late period of gestation it is capable to secrete aldosterone. The role of glucocorticoids in controling immune and inflammatory answer 0lucocorticoids(0C) and glucocorticoid& receptors (0.) are recognized li#e essential modulaters for a long sery of intracellular processes and intracellular communication. !t mammals, the immune and inflammatory answer is a complex physiological process, that has a crucial importance for the homeostasis and survival of the organism. The regulation of immune and inflammatory answer implicates the assurance of an ade"uate reaction at the right time, but without a hyperreaction, which can be a high danger for the organism. -t is considered that 0C are the hormones that mentain the inflammatory and immune answer at the right level for the organism. Two ways of cellular signals were identified as important regalaters of immunity and inflammation& nuclear fact ;,&b and cascades of signals mediated by 0C through intracellular glucocorticoid receptors (glucocorticoid& mediated signal transduction cascades). ;,&5 and 0C& receptors are inducing factors of transcription with opposite functions in regulation of immune and inflammatory answer: ;,&5 mediates the
transcriptional activation of different pro&inflammatory cyto#ines and of genes engaged in immunity, 0. function as supresors of immunity and inflammation& inhibit the expression of the maHority of cyto#ines activated by ;,&5. ;uclear factor ;,&5 is recognized as a ubi"uitous intracellular factor, which can be activated in different tipes of cells. -n non& lymphocitary cells ;,&5 exists as an inactive from of protein, se"uestered in cytoplasma. The activation of ;,&5 factor is made by numerous extracellular pro&inflammatory signals&virus, viral proteins, bacterial lipopolysacharids, pro&inflammatory cyto#ines of L&T;,&tipe, -3&1, -3& , agents that destroy D;!, oxydative stressors and others. -n the moment when these extracellular stimuli action on cells, is activated the way of intracellular signal with the moving of activated ;,&5 towards cellAs nucleo. !t the same time, the transcriptional activity of activated ;,&5 rises dramatically. Bnce it is activated, ;,&5 is bonded to cromatineAs sytes and modulates the expression of genes. 7any tipes of reactive genes to ;,&5 are included in immune and inflammatory answer, brought about extracellular pro&inflammatory signals. -t is well studied the role of ;,&5 in immune system (lymphocytesA growth, inflammatory answer, protective mecanisms), recent investigations involve ;,&5 as an important regulating factor of apoptosis and embryonic development. -n immune cells ;,&5 regulates positively the expression of a big number of genes engaged in mammalsAimmunity and inflammatory answer. The list of transcriptional genes regulated by ;,&5 is commanding growth factors, molecules of cellular adaesion, selectines, cyto#ines -3&1, ,8,D, T;,, beta& interferone, lymphotoxine, proteins of acute phase (angiotensinogen), complementAs factors, immunoreceptors, receptors of T&lymphocytes, anti& apoptosis factors. Corticosteroids action through specific receptors. The family of steroid receptors includes specific receptors for glucocorticoids (0.), mineralocorticoids(7.), progesterone(4.), estrogenes(%.). !ll members of this super&family of nuclear receptors function, through a similar, common mechanism, evoluating as transcriptional factors ligant&depending, which is bonded to D;! and functions by interacting with basal transcriptional apparatus. -n the absence of 0C, classic steroid receptors are holded in cytoplasma into the inactive form, being associated with regulating proteins of the termic shoc#. The inactive conformation of 0C demonstrate a high affinity for steroid ligands. Bnce incorporated in the cell, 0C bond themselves to the cytoplasmatic inactive receptors and produce their activation, which consist in changing of receptorsA conformation, their dissociation from regulating proteins of the termic shoc# and hyperphosphorilation. !ctivated receptors are rapidly transfered to the cellular nucleo, where they bond to a specific se"uence of D;!, called reactive& glucocorticoid. This induces or increases the transcription of target&gene, by interractioning with basal transcriptional apparatus. 0C and glucocorticoid receptors regulate the immune and metabolic genes, canals and transporters.
The general action of 0C consist in induction of inhibiters of pro&inflammatory genes (gene -5 that inhibits ;,&5) and the supression of immune and pro& inflammatory genes& pro&inflammatory cyto#ines, which are the regulating #ey of immune answer and of inflammatory reaction& -3&1, , $, ', 8, D, 1>, 1 , from pulmonary epithelium, peripheric lymphocytes, T;, and -,; from peripheric lymphocytes, %&selectine from pulmonary epithelium, adesive molecules (-C!7&1, %3!7&1) from pulmonary epithelium and endothelial cells, cyclooxygenase& (supplier of 40), the inhibiter of ;B&synthetise from hepatocytes. 0C induce many metabolic genes&genes of thyrosineaminotransferase, glutaminsynthetize, glicogensynthetize, glucose&8&phosphatase, glutaminase, fibrinogen, cholesterol&=&hydrolase, argininsuccinatsynthetize, arginase from liver, obleptine from adipocytes, ileal transporter of biliar acids, sodium canals from foetal lungs, a"uaporine&1, endotheline from vascular miocytes, M& & microglobuline from liver. ;,&5 and 0C are physiological antagonists. ;,&5 is the transcriptional #ey&factor pro&immune and pro&inflammatory, 0. activated by the ligant are powerful supressers of immunity and inflammation. The role of GC in stress'reaction The secretion of 0Cs is the classic answer to stress. 5ut still, the role of 0C in stress is disputed. Concordant to +ans /elyeAs vision, 0Cs are mediaters of stress, which allow the manifestation or stimulate the stress&answer. Contrary to this, there is a revisionist point of vue that postulates that 0Cs supress the stress&answer, preventing the over&pathological reaction (hyperergic reactions). The actions of 0Cs are proHected on the cardiovascular system, the volume of li"uids, immunity and inflammation, metabolism, neurobiological processes and reproduction. -n contemporary vision, the physiologicessence of 0C&hypersecretion induced by stress, is not the protection against the stressing factor, but the protection of organism from the protecting reactions activated by the stress. 0C fulfil this function by bringing bac# to normal the exagerated protecting reactions, that can threaten the homeostasis. !llegorically spea#ing, stress is li#e a fire, protecting reactions are the water that "uash the fire, and 0C have the role to prevent the damage produced by the water. /tress&reaction has some phases KwavesK. The first JwaveK of the stress appears in a few seconds after the action of the stressing factor and includes: 1. The rising of catecholamineAs (C!) secretion in . 1> seconds later, there is the liberation of hypothalamic C.+ in the portal circulation $. The decreasing of secretion of hypothalamic gonadoliberines (0n.+) '. The secretion of prolactine (4.3) and of somatotropine (/T+) <. The secretion of glucagone. -f there is a haemorrhage, the first wave will include, also, the secretion of arginin&vasopressine(!N4) and of renal renine (to other stressers there is Hust a moderate secretion of !N4)* this answer is specific, because the loss of fluids (li#e in haemorrhage) has to be analysrd as a particular side of the stress.
The rapid secretion of hormones from the first wave exerts its maHority of effects through secondary intracellular mesagers, during a few seconds until few minutes. The second wave, more slow, includes the secretion of steroid hormones. During a few seconds, the secretion of 0C is stimulated, but the secretion of gonadal steroids&inhibited. 5ecause the action of steroids is genomic, this is manifested only afterone hour after the beginning of the stress&reaction, and the diminishing of reproductive steroidsA level appears only after a few hours. The effects from the second wave mediated by steroids are: 1) the mobilization of energy to the muscles that ma#e an important effort (for example by mobilizing the stoc#ed energy, the inhibition of further stoc#ing of energy, gluconeogenesis ) the increasing of energic furnishing to muscles by increasing the perfusion of muscles $) the increasing of cerebral perfusion and the local using of glucose with the improvement of cognitive activity ') the stimulation of immune function <) the inhibition of reproductive function and of behaviour (the rapid decline of sexual proceptive and receptive behaviour at both sexes and loss of erection at males, 8) the inhibition of appetite and of using food. -n particular cases (haemorrhage with loss of li"uids), the answer includes, also, the retention of water through renal and vascular mechanisms. 0C, depending of concentration and phase of the stress, exert different actions: permissive, stimulating, supressive, preparatory action. The permissive action is the first depending mechanism, through it the organism fight against the stress and seems advantageous for mediating the answer to a stresser. -t is characterized that 0C, in physiological concentrations (basal secretion), amplify the action of catecholamines, secreted in the first wave of stress&answer* contrary , the lac# of 0C in the anterior period of stress, diminishes the answer to the stress. The stimulating action of 0C is also advantageous in mediating the answer to the stress, and it consists in fait that the level of 0C induced by stress stimulates the action of hormones secreted in the first wave of stress&answer and early physiological reactions, caused by stresser: the abolishement of high level of 0C induced by stress, decreases the physiological answer to a stresser. The supressive action of 0C consists in avoiding the exagerated stress&answer (over&stri#ing), which can be harmful for the organism* the high level of 0C induced by stress inhibits the action of hormones in the first wave of stress& answer and physiological changings induced by the action of stresser* the abolisment of the high level of 0C induced by the stress amplify the physiological answer to the stresser that can have pathological conse"uences. The preparative action of 0C modifies the "uality of the repeated stress&answer and consists the interaction between the high level of 0C induced by stress with the hormones of the first wave of a further stress and modifies the early answer of a further stress, the abolishment of the high level of 0C induced by stress, modifies the physiological answer to the repeated action of the stressers. The
modulation can be mediating and supressive. Thus appears the JcrossedK resistence to the stress. !ll the enumerated actions are manifested together and cases when the 0CAs action consists in only one effect, are rare (for ex. permissive, supressive, stimulating or preparative). -n principle, all the actions can happen depending on the concentration of 0C, on dose :effect curve, on the receptors that ma#e the modifications. 5ecause the 0CAs effects are manifested since the moment when hormones are bonded to their receptors, the latent period is from a few minutes until a few days, and the action of the hormone lasts from a few hours until a few days or wee#s, depending on .;!As period of life and on proteins that transmit the effect. The duration of 0CAs action can have a maHor influence on the answer. The excess of 0CAs is good or without nocive conse"uences for a few days, but becomes letal if it is prolonged. 0Cs effect the primary protection of the organism, avoiding the over&stri#ing, and reduce the potential negative effects of the first protecting line. The maHority of organism and of physiological systems are susceptible to the 0cs action. The best studied effects of 0Cs are: cardiovascular tonus, the li"uidAvolume and the answer to a haemorrhage, immunity and inflammation, metabolism, neural functions, behaviour, reproduction. Cardiovascular effect of 0Cs consist of rising the blood pressure, of the cardiac fre"uence and of cardiac flow (debit), with the redistribution of blood to the muscles by constricting the renal and mesenterial vessels and by dilating the vessel of s#eletic muscles. These effects are due to the inotrope positive effect of 0Cs and due to their permissive effect for catecholamines. The permissive effect for catecholamines is translated through the rising of catecholaminesAsynthesis in adrenergic structures (0l induce phenylalanine&;&metyltransferase), through the prolonged action of C! in neuromuscular Honctions by inhibiting C!As capture from sinapticO and by the decreasing of peripheric level of catecol&B& metyltransferase (CB7T) and 7!B (monoaminoxydase)&enzymes that degrade C!, through the increasing of sensibility of cardiovascular system (0C increase the capacity of bonding and the afinity of adrenergic receptors in vascular smooth muscles, of 0&receptors bonded to proteins and increase the synthesis of 7!4c induced by C!). -ndirectly, by inhibiting the synthesis of 40, 0C blac# the vasodilating effect of 40. -n maHority of cases, 0C facilitate the sympathic interaction, and the prevalent physiological effect is the permissive rising of cardiovascular activation in stress, so, through their permissive action, 0Cs mediate the cardiovascular component part of the stress. The mobilization of cardiovascular tonus done by 0Cs is the vital adaptation to a stress. Different stressers start the cardiovascular activation, this effect is primordiablly mediated by the sympathic ;/, and 0Cs amplify this effect. The removement of 0Cs abolishes the cardiovascular answer to a stress. +aemorrhage is a special stresser, diferent from other types of stresses, by increasing the secretion of arginivasopressine (!N4) and of renine, with vasoconstriction and retention of water. Crucial for haemorrhage is the
hypersecretion of !N4, resulting with vasoconstriction in hepatic and coronarian circulation. This produces ischaemia and further coronarian insufficiency with deep hypoglycaemia (the lac# of hepatic perfusion minimizes the gluconeogenesis. 0Cs inhibit, indirectly, the secretion of !N4 and limit the vasoactive answer to a haemorrhage. ,rom a homeostatic point of vue, the importance of suppression done by 0Cs, as an answer to a haemorrhage, consists in protecting the organism from possible lesions or from death caused by personal defensive mechanisms (for ex. vasoconstriction). The immunosuppressive and antiinflammatory action of 0Cs consist in inhibition of synthesis, liberation and efficiency of cyto#ines and other mediators, that promote the inflammatory and immune reactions. This includes -3&1, , $, ', <, 8, 1 , -,;&gamma, mediators and inflammatory enzymes, such as histamine, eucosanoids, nytric oxyde, colagenases, elastases, activators of plasminogen. 0Cs reduce the synthesis of eucosanoids by inhibiting the expression of inductible forms of cyclooxygenase& . 0Cs inhibit the synthesis of molecule of intercellular adhesion (-C!7&1), the presentation of antigen and the expression of 7+C proteins of -- class, reduce the activation and proliferation of T& and 5&cells, supress the chemotaxis of lymphocytes, monocytes and granulocytes by reducing the accumulation of phagocitary cells in inflammatory focus. 0Cs also, lead to the atrophy of thymus and other lymphoid tissue by initiating the apoptosis in forerunners of 5&cells and T&cells in adult cells. The metabolic actions) -n stress, the glycaemia level rises rapidly, partly from the mobilization of reserves, by inhibition of storing, by the development of insulinic resistance. These changes are induced by C!, glucagone and somatotropine. The prominent effect of 0CsAaction is the hyperglycaemia by stimulating the low appetite, stimulation of glycogenolysis and neoglucogenesis with the help of glucagone and C!, consistuding the immediate answer to a stressor* stimulation of glucogenesis and storing of glycogen in liver, inhibition of transport and peripherical using of glucose, mobilization of lipids by lipolysis in adipocytes and of adipocytes and of aminoacids by inhibiting the synthesis of proteins and stimulating the proteolysis in muscles. 0Cs and insuline have an apposite action on the glycaemia and, also, on the appetite, gluconeogenesis, glucose transport, atrophy of the muscles, synthesis of proteins, lipolysis, lipogenesis* at the same time 0Cs and insuline are synergic in storing of glycogen in liver and lipogenesis. The high level of 0Cs increases the concentration of insuline. Cronic hypercortisolaemia (for ex. Cushing disease) causes muscular pregnant atrophy, accumulation and redistribution of fats, has a diabetogen action. +eurobiologic effects) -n a few seconds, stress rises the glucose use in the brain. /tressing factors facilitate the formation of memory. /tressor inhibits the reproductive behaviour. This includes the decline of portal concentration of 0n.+ and of secretion of pineal gonadotropine in the first minutes. !s a conse"uence, there is a rapid attenuation of erectile capacity and the decline of sexual proceptivity and receptivity at both sexes. -n the first wave this effect is
mediated centrally& C.+ inhibits the physiology and the reproductive behaviour, the administration of C.+ antagonists partially reverses the suppression of 3+& secretion induced by stress. Bpiates released in stress, also, suppress the reproduction, and the same as C.+, inhibit the secretion of 0n.+. /ympathic ;/ has antireproductive properties&bloc# the erection stimulated by the parasympathic ;/. 0Cs hinder the reproductive physiology by decreasing the secretion of 0n.+ and of 3+, by reducing of gonadal reactivity to 3+ and by decreasing the concentration of 3+ receptors. 4robably, these effects areAnot caused by basal concentrations of 0C. /o, adrenalectomy at non&stressed animals does not rises the level of testosterone, showing that basal doses of 0Cs are not sufficient for alterating the reproduction. The administration of >& 1>>m#g6#g6day of dexametasone, for < days, does not diminish the basal level of 3+ at males, while <>>m#g do that dramatically. Congenital adrenal hyperplasia Congenital adrenal hyperplasia (C!+)or the adrenogenital syndrome, describes a congenital disorders caused by an autosomal recessive trait in which a deficiency exists in any of the enzymes necessary for the synthesis of cortisol. ! common characteristic of all types of C!+ is a defect in the synthesis of cortisol that results in increased levels of !CT+ and adrenal hyperplasia. The increased levels of !CT+ over stimulate the pathways for production of adrenal androgens. 7ineralcorticoids may be produced in excessive or insufficient amounts, depending on the precise enzyme deficiency. -nfants of both sexes are affected. 7ales seldom are diagnosed at birth unless they have enlarged genitalia or lose salt and manifest adrenal crisis. -n female infants, an increase in androgens is responsible for creating the virilization syndrome of ambiguous genitalia with an enlarged clitoris, fused labia, and urogenital sinus. -n male and female children, other secondary sex characteristics are normal, and fertility is unaffected if appropriate therapy is instituted. #drenal cortical insufficiency There are two forms of adrenal insufficiency : primary and secondary. 4rimary adrenal insufficiency, or !ddisonAs disease, is caused by destruction of the adrenal gland. /econdary adrenal insufficiency results from a disorders of the +4! system. Primary #drenal Cortical ,nsufficiency -t represents primary adrenal insufficiency in which adrenal cortical cortical hormones are deficient and !CT+ levels are elevated because of lac# of feedbac# inhibition. #etiology !utoimmune destruction is the most common cause of !ddisonAs disease. .are causes include metastatic carcinoma, fungal infection, cytomegalovirus
infection, amyloid disease, and hemochromatosis, bilateral adrenal hemorrhage may, ac"uired immunodeficiency syndrome. Manifestations The manifestations of adrenal insufficiency usually do not become apparent until approximately @>? of the gland has been destroyed. These manifestations are related primarily to mineralocorticoid deficiency, glucocorticoid deficiency, and hyperpigmentation resulting from elevated !CT+ levels. !lthough lac# of the adrenal androgens exerts few effects in men because the testes produce these hormones, women have sparse axillary and public hair. 7ineralcorticoid deficiency causes increased urinary losses of sodium, chloride, and water, along with decreased excretion of potassium. The result is hyponatriemia, loss of extracellular fluid, decreased cardiac output, and hyper#aliemia. There may be an abnormal appetite for salt. Brthostatic hypoptension is common. Dehydration, wea#ness, and fatigue are common early symptoms. -f loss of sodium and water is extreme, cardiovascular collapse and shoc# ensue. Hypo' and hypersecretion of se-ual corticosteroids Congenital form of hypersecretion of sexual corticoids is caused by congenital hyperplasia of adrenal glands and it is manifested by modification of sexual organs at birth :isosexual at boys and heterosexual at girls. !t boys it is manifested by small testicles, developed penis, pronounced pilosityI, stopping of growth. !t girls there is apseudohermaphroditism, intersexuality, hypertrophy of the clitoris that has the aspect of a penis, hypertrophy of big labia, pubian androgen pilosityI, thic#ened voice, hirsutism. Bther forms of hypersecretion are caused by tumours of the corticoadrenal glands, ectopic hypersecretion of sexual corticosteroids, insufficiency of 1& hydroxilase with a decreased secretion of cortisole, hypersecretion of !CT+ and stimulation of androgenAs synthesis. -t is manifested at boys by azoospermia (feminine form, testicular atrophy, at girls&utero&genital atrophy, lac# of mammary glandsA development, amenorrhaea, the reversing of sexual instinct, virilism, hirsutism. !drenogenital syndromes are related to the adrenal secretion of estrogens and androgens. Clinical manifestations depend on the sex, age, and on hormones secreted excessively (androgens or estrogens) and are manifested through two forms: isosexual and heterosexual. !t men, the excessive secretion of androgens (androstendion and andrenosteron) cause the inhibition of gonadotrope hormonesA secretion with the further atrophy of sexual glands. !t women there is an atrophy of primary sexual characters, involution of secondary sexual characters, JmasculinizationK, vigorous muscles (anabolic action of androgens). !t boys there is an early puberty, at men&anabolic effect is evidenced. +ypersecretion of estrogens causes at girls the early puberty, at men : involution of sexual secundary characters, JfeminizationK.
Physiopathology of thyroid gland Thyroid hormones)The synthesis of thyroid hormones consists in a few processes. -nitially, thyreocytes capture from blood and concentrate iodine ions. !limentary iodine proceeds from drin#ing water, iodine&salt and bread (for ex. in C/!), from drugs, disinfectants that contain iodine, preparations with radiological contrast. 0enerally, the daily supply of iodine is >>&<>> mcg.-n geographic areas with a severe lac# of iodine, the daily supply may constitute only 1> mcg per day. !limentary iodine is rapidly absorbed from intestines in blood and with the iodine extracted from tyroxine (T') at deiodination constitute the extraglandular pool of anorganic iodine, dynamically balanced with the thyroid gland and #idneys. The daily "uantity of iodine, captured from blood by the thyroid gland, is about 1>>mcg. The half&period of iodines in plasma at healthy persons without renal diseases is &< hours. !t normal subHects, that use daily 1<> Fg of iodine, the iodineAs clearance is 1>& < ml per minutes* renal clearance is $> ml per minute* this results, prevalently, from glomerular filtration, because there are no dates about tubular secretion or active transport of the iodine. -odine ions are incorporated in thyroid against the concentration gradient. +ere they are transfered in organic compounds by thyroidian peroxydase and eliminated from the cell in the lumen of the follicle. !t the same time, in the granular endoplasmatic reticle the thyreoglobuline peptide is synthetized. Thyreoglobuline is the matrix&protein, on it are synthetized the thyroid hormones in the thyroid gland. Thyreoglobuline is a glycoprotein, that incorporates and contains for about 11> radicals of tyrosine and has the iodinating function. Thyreoglobuline synthetized in the endoplasmatic reticle, is further, also, eliminated by exocytosis through the apical part of cytoplasmatic membrane of the thyreocyte, in the follicle. Thyreoglobuline is the place where iodine&thyronines and iodine&thyrosines are assembled& from tuo molecules of diiodthyronine results tetraiodthyronine (T', thyroxine), triiodthyronine is made from diiodthyrosine and monoiodthyrosine. -n thyreocytes, proteases eut thyreoglobuline in molecules of tetra6triiodthyronine, secreted in lymphatic and blood circulation. The synthesis of thyroidian hormones is regulated by the thyreotrope hormone (T/+)(extrathyroidian mechanism) and by iodineAs concentration in blood (intrathyroidian mechanism). Thyreostimulating hormones is a glycoprotein secreted by basophile adenopineal cells. The secretion of thyreostimulating hormone is regulated at the hypothalamic level by thyreoliberine, at adenopineal level by thyroidian hormones(free from) through the negative feed&bac#. The intrathyroidian mechanism consist in: to an excessive supply of iodine, this inhibits the incorporation of iodine ions in organic compounds and reduces the hormonal synthesis (Golf& Chai#off effect), when iodine lac#s thyreoglobuline is not iodinated, this increases the 7-T6D-T report, the synthesis of T$ is encouraged. This is an adaptational mechanism, destined to produce a hormone with a higher biological activity&T$.
T/+ interactionates with specific receptors from thyreocytesAmembrane, stimulating through secondary intracellular messengers, the capture and the oxydation of the iodine, its incorporation in thyreoglobuline, proteolysis of thyreoglobuline and the formation of thyroid hormones T' and T$. /timulating action on the secretion of thyroid hormones have proteic aliments, low temperature, dar#ness, gestation, parturition, lactation* contrary& a high temperature, strong light inhibits the thyroidAs activity. Thyroid hormones tetraiodthyronine (T') and triiodthyronine (T$) circulate in blood bonded with transporting proteins& T50 (thyroxine binding globulin or albumin* the variation of transporting forms modifies the hormonal balance). /o, in cases when T50 is high, the concentration of total T' is also high, paralelly with a normal concentration of the free T' (for ex. in gestation when estrogens or progesterones are administered)* if the level of T50 is diminished* diminishes also, the concentration of total T', while the concentration of free T' is normal (nephrotic syndrome, hepatic cirrhosis). The peripherical metabolism of thyroid hormones is done by three enzymes, which catabolize the deiodination of thyroid hormones in tissues. Deiodinase type - is responsible of deiodnation of T' in T$* this enzyme produces, almost exclusively, T$ circulating in blood. Deiodinase type -- has the same action expressed in brain, pineal gland, adipous tissue and placenta. 5ecause the activity of deiodinase type -- increases at the same time with the decreasing of availability of T', it is considered that this enzymeA s activity represents the homeostatic mechanism of maintaining the production of T$ in peripherical tissues, including placenta at pregnant women with hypothyroidism, assuring the foetus with the necessary "uantity of thyroxine (necessary for organogenesis). 4lacenta contains and deiodinase type ---, that converts T' in T$, and T$ in T . The biological action of thyroid hormones) Triiodthyronine is the primary thyroid hormone, and tetraiodthyronine(thyroxine) serves as a forerunner for the synthesis of T$ (through deiodination done by iodthyronine& deiodinase). The peripherical conversion of T' in T$ serves to the stabilization of circulating T$ level. The seric level of T' has a supplementary role in the homeostasis of thyroid hormones. -n states characterized by a low concentration of T' in serum, because of a iodine defficiency, the activity of iodthyronine& deiodinase increases in the brain, resulting with the amplification of conversion of T' in T$ and a partial compensation of its defficiency (by intensifying its activity). -nterrelations between T'&T$ have a special importance in the antenal development period of the brain. 5rain is especially rich in deiodinase type --.The intensification of this enzymeAs activity at hypothyroidian animals (in order to maintain the intracellular level of T$) suggests that the interaction of T$ with specific nuclear receptors is a critical stage in mediating the action of this hormone on the brain. T$ is fixed on nuclear receptors T$. with a higher affinity for T$ that for T', the interaction of the hormone with the receptors initiate the cascade of nuclear events, and as a result there is an amplification or inhibition of the expression of those genes, on which de complex T$&T$. is fixed.
The role of maternal thyroid hormones in the development of brain is crucial. /tudies have demonstrated that human embryo with hypothyroidism the transplacentary maternal&foetal transfer assures for about <&<>? of needs in T' for a normal development of the foetus. !s an answer to the decreasing of T' concentration, the deiodinase type -- intensifies its activity in the foetal brain, assuring the maintenance of a normal level or almost normal of T' in brain (but not in other tissues). 5ecause after birth the maternal source disappears, these children can have a normal level of intelectual development only with a right therapy, began right after the birth. Thyroid hormones have metabolic, functional and morphogenetic effects. 7etabolic effect consist in the intensification of oxydative processes, the increasing of oxygen use in muscles, myocandum, liver, s#in, the increase of thermogenesis (calorigen effect) through decoupling of oxidization from phosphorilation. Thyroid hormones intensify lipolisis and inhibits lipogenesis, activates the synthesis of cholesterol concomitantly with the intensification of use and its elimination from organism. The same as adrenalin, thyroid hormones intensify the glucogenolisis, inhibits the glycogenesis, contribute to proteolisis and neoglucogenesis. Thyroid hormones activate the simpatoadrenal and cardiovascular systems, stimulate erythropoiesis, the secretion of digestive glands and appetite. 7orphogenetic effects consist in body growth, formation of C;/ in embryogenetic and early postnatal periods. The estimation of thyroid glandAs function is made by exploring its basal function or its dynamic function* capture and intrathyroid distribution of radioactive iodine* peripherical effects of thyroid hormones. /tatical dosing includes the measuring of iodaemia or ioduria during ' hours* the analysis of free forms of free T' (normally 11& $ pmols6liter) and free T$ (normally $&D pmols6liter).(-t should be mentioned that if there are antibodies anti&T$, the amount of free T$ grows artificially). ,or daily practice it is sufficient the dosing of T' and T/+. Bther tests are: thyreoglobulin, which is dosed for monitorization of thyroid cancer and it rises also in some forms of thyreoiditis, at smo#ers, pregnant women, persons with goitre, the presence of antibodies anti&T0 and it is low in thyreotoxicosis. Calcitonine secreted by C cells of thyroid gland can be dosed by determinating of its basal secretion, and also by stimulating its secretion with pentagastrine. ! hypersecretion of calcitonine allows to diagnose a hyperplazia of C cells, medullar thyroid carcinomes* it can rise in chronic thyroiditis* renal insufficiency, hypercalcaemia, hypergastrinaemia. The measuring of total loss of energy in basal conditions (bazal metabolism) through indirect calorimetria, is also, an index for thyroid secretion. Dynamic tests) The intravenous administration of >> Fg of T.+ (thyrotropin& releasing hormone) generates the secretion of T/+ in maximum $> minutes. The test with T.+ appreciates the reactivity of adenopineal thyreotrope, that depends on the integrity of thyreotrope cells, on level of hormonaemia& the excess of thyroid hormones endo&or exogens inhibits the thyreotrope answer.
The thyreotrope answer allows to differenciate the central pineal (secondary) hypothyroidism from the peripherical (primary). 3ac# of answer to T.+ in period of treatment of goitre or thyroid cancer with thyroid hormones certifies a physiological thyreotrope inhibition. Scintigraphy and fi-ation cur.es The capture of radioactive iodine by thyroid gland needs an inHection with radioactive iodine (-1$1 or -1 $), it is expressed in percents of captured iodine reported to the total administrated dose (normally >? after 8 hours, '>? after ' hours) and reflects the basal hormonal secretion, which is rised when is a hyperthyroidism. This test is contraindicated to pregnant women and children, in overdosing of organism with iodine (iodinated drugs). -sotopic scintigraphy offers the image of the gland and it is done with Tc @@, but only the scintigraphy with radioactive iodine corresponds to the functional image of the gland. Gith this procedure it can be studied the functional aspect of a nodule, that can be JhotK in case of a hyperfixation or JcoldK in case of a hypofixation. The dosing of anti&peroxydase antibodies (anti&T.B) is informative in D>? of cases of +ashimoto thyroiditis, antibodies antireceptors T/+ (-gT/) and antithyreoglobulinic (anti&T0) are found in D> ? cases of 5asedow disease. !t the same time, 1> ? from normal subHects have anti&T0 and anti T4B without having a thyroid pathology. The hyperthyroidism The hyperthyroidism is a syndrome with a thyroid hyperfunction with an excess of thyroid hormones or with exagerated thyroidian effects (the advanced degree is called thyreotoxicosis). There are distinguished three forms of hyperthyroidism: primary&primary affections of the thyroid gland (secretory hormonal adenome), secondary& affections of pineal thyreotropes (active pineal adenom), tertiary&affections of neurosecreting cells of T.+ from hypothalamus. +yperthyroidism represents a conse"uence of a total hyperfunction or a partial one of the thyroid gland. The most fre"uent nosological entity is 5asedow disease, which represents an autonomous thyroid hyperfunction of autoimmune nature. The pathogenesis consists in an autoimmune excesive stimulation of the thyroid gland, independently of pineal gland, by membranary antibodies&antireceptors (receptors fot T/+). Conse"uences of thyroid hyperstimulation are the paren#ymatous hyperplazia with a lymphocitary infiltration and peripherical effects of the hyperthyroidism. J!rtificialK thyreotoxicosis and the iatrogenic one can be induced by the excessive use of thyroid hormones (especially surreptitiously, in order to lose weight). The hyperthyroidism, of different origins, is manifested by neurological, psychic, metabolical, cardiovascular disorders. Disorders of energetic metabolism in hyperthyroidism are manifested by dicoupling the oxidization and phosphorilation in mythochondria, by diminishing the synthesis of T4!, increasing of D4! concentration an
anorganic phosphorus, intensification of energogenesis and calorigenesis, increasing of basal metabolism. 0lucidic metabolism is characterized by the activation of hepatic phosphorilase with intensification of glycogenolisis, depletion of glycogen in liver, intensification of peripherical use of glucose, activation of hexo#inase and intensification of glucoseAs absorbtion from intestines, hyperglycaemia. The activation of pentozophosphoric cycle by thyroid hormones, leads to the synthesis of ;!D4+. !t the same time, the hepatic insulinase is activated, the degradation of insuline is accelerated and there is a defficiency of this hormone, which stimulates its secretion, a prolonged secretion can exhaust functionally the endocrine pancreas. Discorders of proteic metabolism consist in intensification of proteinsA catabolism, a negative nitric balance, an intense nitric excretion, phosphorus and potassium with urine, hypernitrogenaemia resulting from residual nitrogen, hyperaminacidaemia, atrophy of striated muscles, osteoporosis. Disorders of lipidic metabolism are manifested by sensibilization of sympathic fibres in adipous tissue with intense lipolisis, acceleration of lipolisis in liver, inhibition of lipogenesis from glucids, intensification of #etogenesis, hyper#etonaemia, #etonuria. ;eurological manifestations are translated by the increase of C;/ excitability, of vegetative sympathic ;/ with specific effect. Cardiovascular manifestations consist in the increase of concentration of M&adrenoreceptors in heart and the hypersensibilization of organism to adrenergic actions, degradation of thyroid hormones resulting in poducts called pseudocatecholamines. Cardiotrope action of thyroid hormones consist in cardiotrope positive action and metabolic effects in myocardum&intensification of oxidizing processes, decoupling of oxidization from phosphorilation, depletion of glycogen and creatinphosphate reserves, the increase of lactic acidAs concentration. !s a result, the cardiac hyperfunction occurs :tachycardia, an increasid excitability, atrial fibrilation, myocardial hypertrophy* tachycardia associated with metabolic disorders leads to degeneracy of myocardiocytes (myocardiodystrophy) circulatory cardiogen insufficiency. -n hyperthyroidism the tonus of arteriola increases, with arterial hypertension. Clinical important signes of a hyperthyroidism are: a paradoxical loss of weight, at the same time with a present appetite or even bulimia, a predominent wea#ening of proximal muscles (for ex. m. "uadriceps with Jchair symtomK& the subHect sitting on the chair can not rise on his feet), miastenia, tachycardia in repose with sinusal rhythm (1>>&$>> per minute), it is aggravated after physical effort, dyspnaea after effort, diffuse homogeneous goite in bath thyroid lobes, a brilliant loo#, palfebro&retractile symptoms& retraction of superior eyelid with the appearance of upper cornean limbus, oculopalpebral asynergism at a down loo#, at the same time with the increase of upper cornean limbus, rare blin#ing, simple exophtalmia (present in D< ? cases without being specific for 5asedowAs disease* in +ashimotoAs thyroiditis the incidence of the symptom is about 1>?). %xophtalmia is due to the oedema of retrobulbar muscles, that push outside the eyeball and ma#e the appearance of upper and lower cornean limbus.
Bther symptoms are iritability, unstable behaviour, trembling and uns#ilful gestures, oligohypomenorrhaea, osteoporosis especially in menopause, sexual asthenia, impotency and gynecomastia at men, thermophobia, thirst. -t is characteriotic pretibial myxoedema, due to oedematous and inflammatory infiltration ofO Hypothyroidism +ypothyroidism is a state characterized by the insufficiency of thyroid hormones and by the diminishing of thyroid effects. +ypothyroidism can be primary (congenital deffects in hormonesAsynthesis, primary affections of the thyroid gland, inflammatory processes, autoimmune processes, thyroidectomy, radiotherapy, defficiency of iodine)* secundary (pineal affections with thyreotropinAs insufficiency) or tertiary (hypothalamic affections with T.+As insufficiency). !t children, hypothyroidism is translated into thyroid cretinism, at adults&into myxoedema. +ypothyroidism is manifested through disorders of energetic metabolism (diminishing of oxidizing processes, decreasing of basal metabolism), glucidic metabolism (diminishing of phosphorilaseAs activity with glycogenAs accumulation of it in liver, diminishing of hexo#ynaseAs activity with disorders of glucoseAs absorbtion from intestines, diminishing of glucidsA oxidization with oxaloacetateAs defficiency, of pentosophosphoric cycle with ;!4+ defficiency and, finally, the intensification of #etogenesis with hyper#etonaemia, #etonuria, metabolic acidosis), lipidic (hypercholesterolaemia and atheromatosis), proteic (diminishing of proteic anabolism concomitantly with intensification of their catabolism. Congenital sporadic myxoedema has as a cause hypo6aplasia of thyroid gland and it is manifested by a somatic and psychic underdevelopment& thyreoprive cretinism, idiotism. %ndemic cretinism is related to the defficiency of iodine in the soil and waters of some geographical areas. !t the same time with iodineAs defficiency, in pathogenesis of the endemic cretinism are important some exogen substances with thyreostatic action& domestic animalsAexcreta which contain thyreostatic substances, synthetic substances& tiourea, tiouracil, tiocyanids, sulphonamids. ! low concentration of thyroid hormones in blood leads to a hypersecretion of T/+ with speciphic effects& hyperplasia of thyroid (goitre, goitrogen and strumogen action). Hypothyroidism at adults) Thyroid insufficiency at adults can be a conse"uence of thyroidAs distruction, thyroidectomy, drugs, which inhibit the function or the proliferation of thyroid, consume of radioactive iodine, autoimmune thyroiditis, senescence or thyroidAs sclerosis, congenital disorders of hormonogenesis, use of antithyroidians, pineal affections with a T/+ defficiency, overpineal affections with a T.+ defficiency. ! reduced thyroidian hormonaemia can be met in denutrition, congenital defficiency of T50, in the presence of antihormonal antibodies. 4rimary hypothyroidism is more fre"uent of organic origin: congenital and ac"uired& iatrogenic (radioactive iodine, thyroidectomy, radiotherapy),
autoimmune (+asimotoAs thyroiditis), congenital :functional, which is manifested in adult period, in organismAs overloading with iodine, antithyroidians of synthesis, litium. The pathogenesis of hypothyroidismAs manifestations is related to the defficiency of thyroid hormones. Cutaneous manifestations consist in a coutenous&mucous infiltration, myxoedema, anasarcaI, dry s#in, cold especially on extremities, a hard oedema with cold fingers, a swallen figure, rounded, white and oedematous eyelids, violet lips and yellow s#in, macroglossia, brittle nails, rare hair, allopecia, axilary and pubian depilation, senzation of cold and hypothermia. .espiratory manifestations are dyspnaea, alveolary hypoventilation, pleuresia. ;europsychic disorders are manifested through intelectual asthenia, retarded reactions, loss of memory, drowsiness, slow movements, sedentarism, indifference, passivity, depression, hallucinatory psychosis, diminishing of sexuality, paresthesia, myxoedematous coma with hypothermia. Bther manifestations are muscular cramps, hypertrophic myopathia (myoedema), constipations, a swollen abdomen, paralytic ileus, ascitaI, menorrhage, hyperprolactinaemia and galactorrhaea, extension of tur#ish saddle because of thyreotrop cellsAhyperplasia. -n blood a hypercholesterolaemia is detected, microcytary anaemia, normocytary and sometimes macrocytary* in case of a peripherical hypothyroidism (primary) there is an increased plasmatic concentration of T/+ (P8mQ63), diminishing of T' or normal value of T' but with a diminished report T'6T$ (a reserved thyroid insufficiency), in central hypothyroidism (secondary)& the concomitant decreasing of T' and T/+. The test with T.+ allows to differenciate the pineal and overpineal hypothyroidism: the secretion of /T+ after thyroliberineAs administration shows a hypothalamic hypothyroidism (tertiary), the lac# of reaction shows a pineal hypothyroidism (secondary). /imple goitre& represents the volume enlargement of thyroidAs body without inflammatory or degenerative lesions and without secretory disorders. !etiologically, goitre can be congenital, endemic, sporadic and experimental. 0oitre caused by congenital disorders of hormonogenesis is related to iodineAs absence, deficiency of iodineAs incorporation in organic compounds, absence of dehalogenase, anomalas of thyreoglobulin. %ndemic goitre affects ad least 1>? from the population of the region with a deficiency of iodine. (!n endemic goitre is considered so only if 1>? of population is affected). These geographical areas arenAt obligatory in mountainous regions. !etiological factors are many: the daily contribution of iodine is less than <>mcg* natural goitrogens that liberate, tiocyanids (brassica, manioca), malnutrition and pollution, heredity, radiation. /poradic goitre attac#s, especially, adolescent women, its development is encouraged by different stages of genital life. J%xperimentalK goitre is settled in partial thyroidectomy, treatment with synthesis antithyroidians, iodine, litium, urinary loss of proteins which bond thyroid hormones (nephrotic syndrome).
/pontan goitre or the experimental goitre, causes the lac# of iodine or by administrating antithyroids of synthesis* represents the pineal answer to the deficiency of thyroid hormones, with retroreglating stimulation of thyroid hormoneAs secretion. This is a compensatory mechanism, and consist in thyroidAs hyperplasia, after thyreotropAs action and allows the maintaining of euthyroidism. Disturbances of thyreocalcitonineAs secretion. Thyreocalcitonine is secreted by parafollicular C&cells, which are a component part of !4BD system. Calcitonine has an apposite effect compairing to parathormone& inhibits osteoclasts, contributes to their transformation in osteoblasts, stopes boneAs resorbtion, has a calciuretic effect, intensifies the formation of 1, < dihydroxivitamine&D and absorbtion of calcium from intestine. Physiopathology of gonads Physiopathology of testicles) !t maHority of animal species all aspects of reproduction are controled by hormones secreted by ovaries and testicles. These functions include: formation of sexual genotype during embryogenesis, formation of sexual fenotype in postnatal period, which includes sexual maturation during puberty, different forms of sexual behaviour typical for each sex, sexual attraction and potency. !t man, gonadal steroids are responsible for sexual fenotypical differentation, sexual maturation, libido and potency. /exual behaviour at men includes and sex& identity, perception of the masculine& me or feminine one, the behavioural role according to the sex (social sex or social identity), different processes demonstrating the sexual identity to other individs. -t is considered that sexual behaviour at men is more complex compairing to other species and that sexual identity is determined, in a large measure, also, by social and psychological factors. /exual development in ontogenesis. %mbryos of both sexes develop identically until the seventh wee# of gestation, after that anatomical and psychological development diverges. The normal sexual development of the embryo depends on three successive processes. The first process includes the determination of genetic sex in the moment of conception (RR or RS). The second process includes the formation of gonadal sex on the influence of coded information in sexual chromosomes& initial indifferent gonad is differentiated in ovaries or testicles. The final process includes the translation of gonadal sex in fenotypic sex. ,eminization of genital tract is produced if ovaries are present or in absence of functional masculine gonad :in these conditions mullerian ductus developes (bud of feminine genital tract) and inhibition of volfian ductus& bud of masculine genital tract* and as a results the feminine sexual fenotype developes. 7asculinization of urogenital tract or external masculine genitals needs functional testicles and three hormones with three successive actions: antimullerian hormone, testosterone and dihydrotestosterone (<&reduced metabolit of testosterone). !ntimullerian hormone synthetized in foetal testicles
produces the supression of mullerian ductus, preventing this way the development of uterus, uterine tubes at men. The testosterone synthetized by testicles circulates in plasma and transforms the volfian ductus in epididimis, deferent canal and seminal vesicles. Dihydrotestosterone, formed predominantly in target&cells from testosterone, induces the formation of masculine urethra, prostate and external masculine genitals. Disturbances of any of these three processes can cause the anormal sexual development, which generates the disturbances of chromosomial, gonadal and fenotypical sexes. The role of se-ual hormones in controlling libido and potency at men ,rom a biological point of vue, steroids have to type of behavioural effects: organizing and activating. Brganizing effect is exerted by hormones during organogenetic stage and consist in modification of anatomical development of brain, acording to the spece, imparting ireversibly certain stereotypical behaviour models, which, once imparted, manifested tthemselves even if sexual hormones are lac#ing. !ctivating effects consist in arousing of some discreet sexual activities( for ex. copulating behaviour) and needs a continous presence of steroids in order to their full manifestation. This delimitation is conventional. /o, organizing effects can be latent in the absence of sexual hormones, but activating associated effects can persist even after castration. 3ibido or sexual desire is defined as a biological necessity for sexual activity and represents an instinctive sexual attraction, expressed typically through Jsexual searchK (Jsexual huntingK). 3ibidoAs intensity is variable at different individis and even at one individ during different periods of time. 4sychological bases of libido are #nown insufficiently. Determinant factors are: sexual activity in past and present, psychosocial environment, dopaminergic receptors of the brain and of spinal medulla, gonadal hormones. 4otency is the ability to ma#e a complete sexual intercourse. -t includes, at men, the specific reaction to erogenous stimulants by sufficient penial erection for vaginal penetration, a frictional activity of most propitious duration,eHaculation. These functions are influenced by gonadal hormones. /o, at men, prepubertal castration, before the secretion of androgens, prevents the development of sexual attraction, while castration at adult men produces a sexual behavioural decline* only occasionally a castrated men is capable of copulation during years after castration. The substitutive therapy with androgens of hypogonadal men restores rapidly the sexual attraction. The fact that administration of aromataseAs inhibitors at castrated mon#ey male affects the sexual attraction, demonstrates the crucial role in sexual attraction of estrogenic metabolits of testosterone, but not of testosterone itself. %vidence of androgensArole in regulating the sexual behaviour at man is supported and by libidoAs dependence of seric concentration of testosterone, but this is more true at old men, not at young one. The high level of testosterone can shorten the latency period of erection stimulated by erogen factors, as well as refractory period, the restoring of testosteroneAs level at hypogonadal men,
restaures the sexual interest, shortens the posteHaculatory latency and refraction, increases the fre"uency and magnitude of nocturnal erections. !nd versus, the ceasing of therapy with testosterone at hypogonadal men leads to libidoAs decline during $&' wee#s, at the same time with diminution of spontaneous erections. !t women, annihilation of ovarian secretion (ovarectomy) or in natural menopause has no essential effect on sexual activity. %xplication consists in fact that sexual feminine patern, once fixed in ontogenesis, becomes hormonally independet. -t is possible that sexual attraction at women is depended on the same hormones, as men, so androgens. 5ecause ovarectomy doesnAt influence the formation of adrenal androgens, this doesnAt affect and sexual attraction. Contrary, hypophisectomy or adrenalectomy, at the same time with ceasing of androgensAsecretion at women castrated anteriorly, diminishes the sexual desire. -t is considered that adrenal androgens at women have a direct effect on sexual desire or actuate as prohormones for the synthesis in extraglandular tissues of other steroid hormones, which can maintain the sexual attraction when ovarian hormones are las#ing. !t castrated men, in extraglandular tissues from adrenal androgens, considerable "uantities of estrogens are formed, but only small "uantities of testosterone, which can be sufficient at only few men in order to maintain the libido and the potency. 0onadal steroids have an important role in sexual attraction at males of all species and control the sexual attraction at females, and, possibly, at women. /exual identity and sexual behavioural role at human species is fundamentally different at men amd women. The sexual behavioural role is influenced by cultural and social factors, fact that results from different activities of both sexes in different societies. /ole of se-ual hormones in pineal erection 4enial erection is the final answer to various (many) erogen stimuli: psychogen and sensorial from imaginative sources, visual, auditive, olphactive, tasting, tactile and genital reflexogen sources, which cause cascades of neurologic and vascular phenomenons, which lead to penial tumescence and to a sufficient rigidity for vaginal penetration. %rection is associated with essencial psychological and physical modifications, including sexual Jawa#eningK, testicular tumescence, dilatation of urethral bulb, enlargement of gland and of circular penial dimensions, s#inAs hyperaemia upper the epigastris, chest buttoc#s, erection of nipples, tachycardia, hypertension, hyperventilation, general myotonia. 4enial local modifications represent a conse"uence of parasympathic vasodilatation, under the action of impulses came from C;/ or as a result of reflex action as an answer to afferent local stimulation of sacral parasympathic nuclei. -t is cosidered that androgens modulate the reactivity of nervous centers at erogen stimuliAs action. ;ew data certify the involvement of gonadal androgens in modulation of penial erection, by regulating the local secretion of ;B (nitric oxyde is a powerful relaxing
factor of blood vesselsAmuscles, which can produce arterial hyperaemia). %xperiments had shown the reduction of ;B& synthetase in pineal tissues after castration and the restoring of ;B/ reserves during androgen substituting therapy. This repels the old theory that androgens actuate only by central modulation of libido. Data about androgensAinfluence on reflex erectionAs fre"uence Jnon&eroticK, also sustain the role of peripherical action of androgens at men. .ecent studies on rats have demonstrated the role of dihydrotestosterone, and not testosterone, in local modulation of ;B&c 074 way. The fact that androgens amplify the nocturnal penial tumescence, but not the erection as an answer to erotic stimuli, suggests the existence of central androgen&sensitive and androgen insensitive ways for control of erection. 4enian erection is related to subtraction of resistance in vascular bed of penis an further increasing of arterial flow, leading to to overfuslfiling with blood of cavernous bodies. Dramatical increasing of arterial penian flow for <&8> times leads to tumescence. /o, intracorporal pression in flaccid penis is 1>&1< mm +g, during initial phase of sexual cycle modifies modestly and stays at this level until the maximal circumference and volume of penis are achieved. Bnce the penis becomes erect, the pression in penisAbody arises rapidly until @> mm+g. The contraction of perineal muscles generates the further arising of intrapenial pressure upper than 1 > mm+g (oversistolic pressure), resulting in complete rigidity and elevation of penis more than @>T, compairing to inferior membres. !fter eHaculation and orgasm, the pressure in penial body declines rapidly, and volume is bac# to flaccid stage. /erical androgens can have a role in regulating the nocturnal penile tumescence, ;4T, which represents the spontaneous erection (about =>? from total rigidity) appeared in paradoxal phase of sleep. The phenomenon appears '&< times during a night, with an interval of about @> min, each episode lasts about $>&'< min* total duration is @>&1D> min for a night ( >& <? from total duration of sleep). The number and duration of episodes substracts with age: 8,D&' times at 1$ years, until $,<&1,= episodes at => years, total time of tumescence substracts until <? from time at 1$ years. The maHority of dreams associated to episodes of penile tumescence have an erotic colour. %rection at awa#ening is the last episode of tumescence, but it is not related to fulfilment of gall bladder. The substitutive administration of androgens restores ;4T at hypogonadal men and old men. !ntidepressive and antihypertensive drugs influence ;4T. Trasodon, an antidepressive drug with complex action, with inhibiting the recapturing of serotonine, prolonges the ;4T duration, amitriptiline and mianserine reduces the amplitude and duration of ;4T. The promotion of copulation through testosterone seems to be mediated by the increasing of dopamineAs liberation in preoptical medial area, possible through synthesis of ;B. The role of dopaminergic activation in stimulation of sexual behaviour at men is sustained by the following fact: the administration of apomorphine,
bromocriptine (dopamineAs agonosts) causes spontaneous penile erection* us of dopamineAs forerunner&levodopa, is associated to libidoAs increasing, restoring of spontaneous erection and nocturnal emissions at >&$> ? of patiens with 4ar#insonAs disease, treated with this agent* use of antidopaminergic agents causes the decreasing of libido and erectile disfunctions in <>? of cases. %Haculation is controlled by sympathic enervation of genital organs and appears as a result of activity of spinal reflex bow. %Haculation consists from two consecutive processes: emission and eHaculation itself. %mission consist in storing the seminal li"uid in posterior urethra, through simultaneous contraction of vas deferens ampulla, seminal vesicles and smooth muscles of prostate gland. True eHaculation is the expulsion of fluid seminal li"uid from posterior urethra through meatus. The influence of androgens on eHaculating act consist in amplification of spermatogenesis, seminal and prostatic secretions, modifying this way the volume and composition of eHaculating li"uid. The 0rgasm) To orgasmAs genesis contribute physiological and psychological elements. !scendent stimuli generated by the sexual act and transmitted from genital organs through pudental nerve induce the physiological elements: the contraction of accesory muscles of sexual organs* senzation of inevitability of eHaculation, liberation of pressure in posterior urethra, contraction of urethraAs bulb and perineum, rhytmical contraction of pelvicO, emission of sperm and eHaculation, reversion of sexual tension and generalized physiological modifications. /ensorial cortical neurones perceive these events as pleasure. ,actors that influence subHectively the sensation of orgastic pleasure, include the degree of sexual excitement, the novelty of sexual activity, psychosexual of individ. Detumescence) -n this phase, penis returns to its flaccid state. Nasoconstriction of arterioles and reversion of events in contractual elements, remove the blood from cavernous bodies and allow the increasing of venous flow. -nitially, the speed of venous reflowing increases 1> times, further it achieves the pretumescent level. !ctivation of adrenergic local penile receptors is the most important neuromechanism of detumescence.The interference with this function by bloc#ing L&1 receptors can lead to priapism& prolonged persistant erection during 1 & ' hours (even more). /efractory period is the period after eHaculation, during it erogen stimuli can not cause sexual excitement and penile erection. Duration of refractory phase depends on age, physical statement of the individ, psychological environment. -t should be mentioned that not all the time orgasm at men is followed by detumescence and refraction& there are observations that demonstrate the fact that some men are multiorgasticI :have repeated orgasms, without detumescence and refractority. #ndrogen secretion, se-ual function and age at men) Concomitantly with age, sexual reactivity at men decreases, it is manifested by the prolongement of time necessary to achieve total erection to psychic and tactile stimuli. The plateauAs phase (persistant sexual excitement is also
prolonged, the maintaining of erection needs continous genital stimulation. The orgasm and the sensation of inevitability of eHaculation becomes less intense. Detumescence occurs more rapidly, the refractory period becomes longer. The volume of eHaculated li"uid decreases. Concomitantly with age, in penian vessels the number of nervous fibres decreases, which contain ;B/ (;B& synthetase), the erectile answer to stimulation with apomorphine decreases, also as maximal intravernous pressure. Bnce with age, the seric concentration of bio&available testosterone diminishes, the report of testosterone to estradiol reduces (the androgens decrease, the estrogens increase), the concentration of globulins that bond sexual hormones increases, fact that leads to increasing of circulating testosteroneAs fixation, clearance decreases and reduces the accumulation in reproductive tissues of active <&reduced steroids. 5eginning with the age of '> and until => years, the concentration of seric testosterone decreases yearly with 1?. !t hypogonadal persons there is the loss of sexual intenest and activity, decreasing of seminal emissionAs volume, diminishing of nocturnal and matinal erection, decreasing of energy and sensation of wellbeing* the substitutive administration of testosterone leads to amplification of libido, of sexual potency, increases the number of nocturnal erections, certifying the fact that severe deficiency of testosterone is the primary cause of sexual disfunctions in cases of hypogonadism, including erectile disfunctions. +ypogonadism& represents the diminishing of functions exerted by gonads and has a specifical character (depending on sex). 0eneral causes of the hypogonadism (masculine and feminine) are congenital (chromosomial anomalies, agenesia, disgenesia of testicles) and achieved (pathological processes in hypothalamus, pineal gland, testicles). 7asculine hypogonadism includes the hypofunction of germinative epithelium, leading to masculine sterility or to hyposecretion of 3eydig cells, which leads to hypoandrogenia. 4repubertal hypogonadism is manifested by restraint of somatic sexual development (under& development of sexual organs and annexed organs, lac# of sexual secondary characters) and of manifestation of masculine sexual behaviour (diminishing or lac# of libido, erections). The ensemble of signs combines the syndrome of eunuchoidism, characterized by excessive growth in lenght of membreAs bones, retardation of cartilagesAosification, microgenitalism, O under development of muscles, subcutaneous adiposity of feminine type. 4ostpubertal hypogonadism leads to the involution of primary and secondary sexual characters, by progressive decline of masculine sexual behaviour. ,eminine hypogonadism (hypoovarian state) is characterized by dereglation of maturation of ovarian follicles and6or ovulation and dereglation of secretion of estrogens and progestines. +ypoestrogenia is characterized by restaint of puberty, underdevelopment (or involution) of external sexual organs and anexxes, atrophy of endometrium, vaginal epithelium, hyposecretion of genital glands, lac# of cyclic hormonal processes and in sexual organs, excessive growth of membresAbones and retardation of cartilagesAosification, sterility. /econdary sexual characters lac#
also& O underdevelopment of mammary glands. The prepubertal hypergonadism is manifested by early puberty at boys, girls, with specifical manifestations. Physiopathology of endocrine pancreas %ndocrine pancreas secretes two hormones in appreciative "uantities and with distinct physiological activities: insulin and glucagon. -nsulin is synthetized by beta cells of pancreas. The expression of insulin gene in beta cells of pancreas is regulated by glucose. 0lucose regulates the secretion of insulin through glucose&sensible system of beta&cells. 0lucose stimulates transcription and stabilizes insulinAs .;!m, causing its liberation from secreting granules of beta&cells. /ecretion of insulin and of C&peptid is stimulated, besides glucose, by aminoacids (especially by arginine and lysine), #etonic bodies and fat acids and it is made through exocytosis. The half period of insulin in circulation is about $> minutes. 3iver retains about 8>? of insulin, in #idneys are filtered about '>? of insulin, which further are reabsorbed and degraded in epitheliocytes of proximal canals. -nsulin participates in regulation of glucidic, lipidic, proteic metabolism, transmembranary transport of ions and glucose, nuclear transcription, differentiation, proliferation and transformation of cells. -nsulin and glucagon (main contrainsular hormone) maintain energetic homeostasis of organism& e"uilibrium between offert of energy and real necessities of organism, modulate the metabolism between two states of organism: digestion (absorbation of nutrients, that lasts 1>&1< hours from ' hours), and starvation (that lasts @&1' hours). 5ecause organism uses energy continuously, but ingeration is discontinuous, is important to store the surplus of energy arrived after digestion (in liver, adipous tissue and muscles), for its further using during starvation. /o, the storing regime O alternates with mobilizating regime of nutrients. The cellular use of glucose is made through transmembranary hydrophile canals& transporting proteins (receptors) of glucose through two mechanisms: active transport depended on sodium ionsAgradient and facilitated difusion (in remainder organs). .eceptors of facilitated difusion are of five types, but only receptors from s#eletic muscles, myocardum and adipocytes (receptors of type -N) are regulated by insulin (these tissues are called insulindepended), while other types of receptors do not depend on insulin (it should be mentioned that receptors for glucose from beta&cells of pancreas, that participate in regulation of indsulinAs secretion, are insulinoindepended). -nsulinindepended receptors are localized on cytoplasmatic membrane and also in cytoplasm. -nsulindepended receptors (type -N), in lac# of insulin, are localized only in cytoplasm, in cytoplasmatic vacuoles, cellsAstimulation with insulin leads to vesiclesAtranslocation to cytoplasmatic membrane and their incorporation in membrane, forming transmembranary canals. !s a result, transmembranary transport of glucose in adipocytes and myocytes increases $>&'> times. Ghen insulinAs concentration
decreases, receptors detach themselves from cytoplasmatic membrane and return in cytoplasma. Transduction of insulinic signal is made through membranary receptor, which represents a piruvat#inase, present in almost all types of cells, but especially in hepatocytes (about <>>>> per cell), adipocytes (about <>>>> per cell). -nteraction of receptors with insulin induces transcriptional processes of metabolic specific genes: gluco#inase, glyceraldehiddehydrogenase. 7ain generators of energy are glucids and lipids, less important& proteins and aminoacids. 7etabolism devolves in function of organismAs state. /o, during digestion period, anabolic processes prevail :storing of glucose as glycogen (glycogenogenesis), glucoseAs splitting until L&glycerophosphate and acetyl& Co!, from which further lipids are synthetized (lipogenesis). -n starvation prevails glycogenolysis with glucoseAs splitting in Urebs cycle, until final products with generation of energy, lipolysis with fat acidsAliberation, complete oxidization of them, proteolysis with liberation of aminoacids and synthesis of glucose (gluconeogenesis) and further use of neoformed glucose. !lternation of digestion with starvation (at least times in ' hours) modifies diametrically direction of metabolism. -t should be mentioned that #ey&enzymes of metabolic chains are controlled by insulin, glucagon, adrenalin and cortisole. 4rimary signals for reversion of metabolic processes in digestion and starvation are glucoseAs concentration in blood and e"uidirectional modifications of insulin and contradirectional of glucagon. %ffects of these hormones are opposite: insulin activates glycogensynthetase and inhibits glycogenphosphorilase, while glucagon inhibits glycogensynthetase and activates glycogenphosphorilase. -nsulin inhibits synthesis of glucose&8&phosphate, glucagon&dephosphorilation of glucose&8&phosphate, insulin stimulates glucoseAs splitting until piruvatI !nd further synthesis of fat acids from acetyl&Co!, glucagon inhibits this metabolic way. Bnce with these mentioned facts, insulin inhibits directly glucagonAs secretion. -nsulin processes an anticatabolic action on proteins (inhibits gluconeogenesis from proteins and aminoacids) and a direct metabolic action: contributes to transmembranary transport of aminoacids in cells and stimulates .;! synthesis and proteosynthases. -n hepatocytes glucose penetrates through receptors for glucose type --, independent of insulin. 7etabolic processes of glucose in hepatocytes include formation of glucose&8&phosphate with gluco#inase (hexo#inase -N), which further can be subdue to three processes: synthesis of glycogen, glycolysis and pentosophosphoric cycleI. !cetyl&Co! formed from glucose is used for synthesis of fat acids. !ll the stages of glucoseAs metabolism in hepatocytes are regulated by insulin, pretranslational level (synthesis of .;!m) or posttranslational level (synthesis of respective enzymes). 0enes regulated by insulin are: gluco#inase and T4!& citratliase of hepatocytes, glyceroaldehiddehydrogenase of adipocytes.
0lucagonAs effects on these processes are opposite. /ummary metabolic effect depends not so much on absolute concentration of hormones, but more on report of insulin6glucagon concentrations. ,nsulinic insufficiency -nsulinic insufficiency constitutes the main lin# in pathogenesis of insulindepended diabets or diabetes type -. Diabets type - is related to deficiency of insulin, consecutive to reduction of beta&cellsApopulation from pancreas. Bne of maHor cause of -DD is inflammation with autoimmune alteration of 3angherhans islands (insulitis), with an exclusive specific location in islands formed by beta&cells, while in islands formed by cells producing glucagon inflammation is lac#ing. Deficit of insulin causes multiple metabolic disorders with severe lesions in organismsAstructures. Disturbance of synthesis of glycogen and lipids is primordial metabolic manifestation and essential of insulinic deficiency. These are related to decreasing of insulin6glucagon index. The conse"uence is liverAs incapacity and musclesAto synthetize glycogen and of adipocytes to synthetize lipids from glucose. -n deficiency of insulin, these organs, even in absorbtional digestive period, function in a starvating regime: with inhibition of anabolic glycogenogenetic and lipogenetic processes and predomination of catabolic glycogenolytic and lipolytic processes. Concomitantly, the proteolysis with neoglucogenesis is intensified. The reduced tolerance to glucose, hyperglicaemia, intensified proteic catabolism, hyperlipidaemia, angiopathy, renal syndrome are cardinal clinical signs of diabetes type -. 4athogenesis of hyperglicaemia consists in fact that, in lac# of insuline, insulinodepended receptors type -N for glucose from myocytes and adipocytes retire themselves in cytoplasma, are not exposed on cellulary membrane, this is why glucose can not be assimilated by these cells for synthesis of glycogen and lipids. ! reduced tolerance for glucose reflects cellsAincapacity to assimilate glucids. This explains the fact that in insulinAs deficiency liverAs glycogensynthetase remains in inactive, phosphorilated form, a high concentration of glucagone stimulates processes of glycogenolysis. 5ecause of the inactive state of glycolytic enzymes and of piruvatedehydrogenase the transformation of glucose in acetyl&Co! is inhibited, and consecutively, the synthesis of fat acids (lipogenesis). !t small concentrations of insulin, neoglucogenesis from aminoacids and glycerol is activated. 0lucagon intensifies the processes of proteolysis, the result is hyperaminoacidaemia, aminoaciduria, the increasing of urea and ammoniaAs concentration in blood. The pathogenesis of hyperlipidaemia (predominantly on lipoproteins with very little density and on nonesterified fat acidsAaccount) is explained by the fact that, in lac# of insulin, adipocytesAlipase stays phosphorilated, inactive, alimentary lipids are not incorporated in adipocytes, and non&re"uired fat acids are
transformed in liver in lipoproteins with very little density. The increasing of blood concentration of nonesterified fat acids (transporting hyperlipidaemia) is a conse"uence of intense mobilization of lipids from adipous tissue. +yper#etonaemia and #etonuria is due to high concentrations in blood of fat acids, with intensification of beta&oxidization and abundant production of acetyl& Co!, that, in lac# of insulin, is not used for lipidsAresynthesis, but for synthesis of #etonic bodies&acetone, hydroxibutiric acid and acetylacetic acid. .enal syndrome in hypoinsulinism consists in glucosuria, due to a high hyperglicaemia and high concentration of glucose in renal filter, that outruns the functional capacity of gluco#inase from canalicular epithelium (the limit is about 1D> mg6D3). 0lucosuria rallies polyuria (osmotic diuresis), and polyuria consecutive polydipsia. Development of microangiopathy with diabetic nephropathy leads to a progressive diminishing of glomerular filtration, to the increase of renal filterAs permeability with albuminuria. Uetonuria is consecutive to hyper#etonaemia. Diabetic angiopathies have in their pathogenesis proteinsAglycozilation& a processes proper to -DD, that consist in non&enzymatic association of glucose to aminogroups of aminoacids, with formation in vascular wall of complexes made by glucose and proteins (#etoaminproteins). 0licozilation modifies the conformation of proteic molecule, electric charge, modifies proteinsAfunction, bloc#s the active centre. Diabetic angiopathies affect small vessels and big vessels. 0eneral pathogenesis of diabetic angiopathies consists in proteinsAglycozilation and alteration of basal membrane of vessels, degradation of intercellular matrixAcompounds (colagen, fibronectins, proteoglycans, integrins). -n sum, results the remodelation with thic#ness of basal membran. 7acroangiopathy devolves as an atherosclerosis, with a predominant affectation of vascular intima, and it is observed in heart, brain, legs. /uccession of these processes include the glicozilation of proteins, alteration of basal membrane, liberation of cyto#ins, activation of endotheliocytes, vascular myocytes, fibroblasts, macrophages, their infiltration with lipoproteins, formation of atheromatosis plate. This process is favorized by the high blood concentration of atherogen lipoproteins with very little density, characteristic for diabetes. !nother pathogenetic mechanism of diabetic macroangiopathy consists in glicozilation and alteration of colagen and elastin from vascular wall, fact that modifies mechanical properties of vessels. 7icroangiopathies are met at about 16$ of diabetic patients, attac# predominantly glomerular capilaries, with resolution in glomerulosclerosis. The basic compound of capilary wall in renal glomeruli is basal membrane, on one side of it are endotheliocytes, on the other side&podocytes. 0lomerular capilaries are sustained by a tree&li#e mesangium, consisted from mesangial cells and matrix. -n diabetes there is proteinsAglycozilation, that thic#ens basal membrane, the whole vascular wall, with diminishing of glomerular perfusion and speed of filtration, increases the permeability of glomerular capilaries with albuminuria, hypertrophy of mesangial matrix, leading to complete obturation of vessels, their sclerosis&glomerulosclerosis. -n region of renal tubuli there is a tubulo&
instertitial fibrosis. -t should be mentioned that diabetic angiopathies are appreciated as a disturbance of reparative processes, orientated to reparation of bazal membraneAs and mesangiumAs lesions, caused by pathogenic factors of diabetes. Bther forms of microangiopathy are retinopathies. Diabetes can lead to comas: #etoacidotic in absolute insufficiency of insulin, hypersmolary in moderated insulinic deficiency, lactoacidotic in hypoxia, septicaemia, cardiogen shoc# (over dosing of insulin can lead to hypoglycemic coma). !cidosis is also a conse"uence of hyperlactacidaemia produced as a result of liverAs incapacity to resynthetize glycogen from lactic acid formed in different organs. 4rimary cause of #etoacidotic coma is absolute insufficiency of insulin (in blood insulin and C&peptid are not found). -t is manifested through hyperglycaemia ( >&$> m7ol63), glucosuria, decompensated metabolic acidosis by accumulation in blood of #etonic bodies (concentration can increase >> times until m7ol6D3), lactate, piruvate* p+ is lower than =,> ,the dehydration with total deficit of water occurs in 1>? and decreasing of intravascular li"uid with <&$>?, polycytaemia hypovolemic, hemoconcentration, arterial hypotension, circulatory insufficiency. Disturbances of perfusion lead to hyponutrition and hypoxia of myocardum with cardiac insufficiency. .heological disturbances of blood can lead to hypocoagulation. 4athogenetic correction of homeostasis in #etoacidotic coma follows the abolition of insulinic deficiency, rehydration and resalting of organism, restoration of acido&basic e"uilibrium and of glycogen reserves. ,nsulinoresistance Diabetes type -- is characterized by disfunction of beta&cells of pancreas and resistance to insulin of maHority of periferic target&tissue: s#eletic muscles, liver, #idneys, adipous tissue. 0enetic researches have determined that at a child from parents with diabetes type --, there is a primary resistance to insulin, and also disfunction of beta&cells. Bften insulinic resistance is synomymized with incapacity of storing glucose after a stimulation with insulin, masured byKhyperinsulinaemia&euglycaemiaK test (the tolerance to insulin increases, this is why the necessary dose for maintaing euglycaemia is increased too). ,urther, investigatorsAattention was concentrated on insulinoresistance of organs responsible for capture of glucose ( muscles, adipous tissue). 5esides this, the lipolysis is studied, and production of glucose through glycogenolysis& processes which are inhibited by insulin. -n insulinoresistance capturing of glucose is inhibited, lipolysis and endogen production of glucose get out of insulinAs control. 5esides muscles and liver, adipous tissue is the third metabolic area of insulinAs action. ! maHor implication in glucidic metabolism is regulation by insulin of lipolysis and delivery in circulation of glycerol and free fat acids. 0lycerol represents a source for endogen synthesis of glucose, a high concentration of ,,! contributes to development of insulinoresistance of muscles. ,rom adipous
tissueAs resistance to antilipolytic action of insulin results an excessive liberation of ,,! and of glycerol, which has a bad influence on glucoseAs homeostasis. -n insulinoresistance (at persons with diabetes type --) dose of exogen insulin increases considerably, which stimulates glucoseAs capturing by tissues and inhibits de production of endogen glucose. 3ipolysis is the most sensible process to insulin: at persons with D type --, dose of insulin that inhibits lipolysis is &$ times higher than at healthy persons. This indicates the fact that adipous tissue is as sensible to insulin as muscles or liver are. The series of processes aranged in diminishing way of their sensibility to insulin is: lipolysis&endogen production of glucose&capture of glucose. Pathogenesis of insulinoresistance -nsulinoresistance reflects the deficiency of insulinAs action, predominantly in s#eletic muscles and liver. 7aHor causes of musclesAinsulinoresistance in prediabetic stage are: genetic propensity, obesity and physic hypoactivity. -n insulinoresistance and D type -- deficiencies in insulinic signalizationAs chains had been revealed. !t cellular level insulinic signalization begins with fixation of insulinic on cellular specific receptors, which stimulates the autophosphorilation of intracellular subunity of receptor. !t patients with diabetes type -- reduction of autoactivation of insulinic receptors on myocytes and adipocytes was observed. -t was demonstrated that obesity is the maHor factor that contributes to a reduced activity of insulinic receptors, fact that suggests the conclusion that reduction of #inasic activity of receptors is secondary and consecutive to obesity, hyperinsulinaemia and hyperglycaemia. There are convincing data about hereditary character of diabetes type --. 0enes&candidates are gene that clone insulinic receptors intracellular subunity, protein#inases, hepatic gluco#inase, glycogensynthetase, proteinphosphatase. Bbesity and lac# of physical exercises are maHor factors that contribute to development of insulinoresistance. -t was established that physical exerceses increase the sensibility to insulin, independently on reduction of bodyAs weight and modifications of bodyAs composition. /o, at children from parents with diabetes type --, physical training during 8 wee#s activates glucoseAs capture and synthesis of glycogen, as a result of increasing of sensibility to insulin. ,at free acids from adipocytes are involved in pathogenesis of insulinoresistance. -n insulinoresistance the antilipolytic effect of insulin decreases, that at the same time with activation of sympathic system, causes liberation of ,,! in blood. ,,! counteract insulinAs effects, by inhibiting glucoseAs capture and oxidization in s#eletic muscles and rising of acetyl& Co!Aproduction. -n pathogenesis of insulinoresistance has an importance and leptin&hormone derived from adipocytes. 3eptin reduces body wlight through hypothalamic specific receptors, that regulate energic expenses of organism and sensation of satiety. 3eptinAs secretion is related to adipous tissueAs mass. Deficiency of leptin or deffect of receptors causes obesity at rats, hyperinsulineamia,
hyperglycaemia. !t man, mutations in leptin&receptors system are extremaly rare.
You might also like
- Chapter 125Document18 pagesChapter 125Saloni SaloniNo ratings yet
- Endocrinologia EquinaDocument7 pagesEndocrinologia EquinaNiñoTorresNo ratings yet
- CH 45 Guided ReadingDocument7 pagesCH 45 Guided ReadingmharirajNo ratings yet
- Human and Animal Physiology Chapter 18 The Central Endocrine GlandsDocument21 pagesHuman and Animal Physiology Chapter 18 The Central Endocrine Glandshitmanno5No ratings yet
- EndoDocument252 pagesEndoyuuki konnoNo ratings yet
- Hypothalamus - Anterior Pituitary and Their HormonesDocument138 pagesHypothalamus - Anterior Pituitary and Their HormonesML Rodriguez100% (1)
- Determination of Hormones: Mohamed A.Ali BSC - HLS, Admls, DmlsDocument43 pagesDetermination of Hormones: Mohamed A.Ali BSC - HLS, Admls, Dmlsmoha3liNo ratings yet
- Lec 2Document9 pagesLec 2Imran HussainNo ratings yet
- Endocrine System ppt1Document47 pagesEndocrine System ppt1Aldrich Paul CelisNo ratings yet
- Group 2 Endocrine System Questions 5 - 7Document35 pagesGroup 2 Endocrine System Questions 5 - 7Marcus KaglNo ratings yet
- AP-2 Lab Report - Lab 01 The Endrocine SystemDocument15 pagesAP-2 Lab Report - Lab 01 The Endrocine Systemrcdunfee86% (7)
- Endocrine Glands Are Glands of TheDocument9 pagesEndocrine Glands Are Glands of ThextinebadzNo ratings yet
- Pharmacology of The Endocrine System PDFDocument74 pagesPharmacology of The Endocrine System PDFGlenn Perez71% (7)
- Endocrine GlandDocument4 pagesEndocrine Glandakash_zizouNo ratings yet
- Endocrine System Part 1.Document57 pagesEndocrine System Part 1.Jonathan Young XDNo ratings yet
- Answers2e ch27Document8 pagesAnswers2e ch27Pat ChuaNo ratings yet
- Male HypogonadismDocument11 pagesMale HypogonadismRendhy Wisnugroho SantosoNo ratings yet
- Fazio Log YeDocument31 pagesFazio Log YeBianca NegrutNo ratings yet
- Endocrinology HandbookDocument75 pagesEndocrinology Handbookhirsi200518No ratings yet
- Unit - Iv Human Anatomy and Physiology: Very Short Answer QuestionsDocument12 pagesUnit - Iv Human Anatomy and Physiology: Very Short Answer QuestionsRK YeleswarapuNo ratings yet
- MODULE 2 Disorders of The Pituitary GlandDocument24 pagesMODULE 2 Disorders of The Pituitary GlandLorraine GambitoNo ratings yet
- Endocrine Gland: Aldrin Mercado Bsae Ii-ADocument3 pagesEndocrine Gland: Aldrin Mercado Bsae Ii-AaldrinNo ratings yet
- Endocrine Gland - Wikipedia, The Free EncyclopediaDocument5 pagesEndocrine Gland - Wikipedia, The Free EncyclopediakbhattacNo ratings yet
- Pharmacology of The Endocrine SystemDocument74 pagesPharmacology of The Endocrine SystemarpanabiswassshetyeNo ratings yet
- Endrocrine SystemDocument6 pagesEndrocrine SystemAsif Hasan NiloyNo ratings yet
- NTU BS3104 Endocrine NotesDocument116 pagesNTU BS3104 Endocrine NotesChen HouyuNo ratings yet
- Hypopituitarism Group F BSN 3Document21 pagesHypopituitarism Group F BSN 3Mari IllustriousNo ratings yet
- CA2018PPt NewDocument32 pagesCA2018PPt NewAshlene Kate BagsiyaoNo ratings yet
- Suprasellar Region PDFDocument114 pagesSuprasellar Region PDFmalex33yNo ratings yet
- Biochemistry of Hormones (Part 1)Document31 pagesBiochemistry of Hormones (Part 1)arun231187100% (1)
- UNIT II Endocrine & Metabolic DisordersDocument19 pagesUNIT II Endocrine & Metabolic DisordersAmmar BhattiNo ratings yet
- Disorders of Endocrine SystemDocument48 pagesDisorders of Endocrine SystemSHARIM ASGHARNo ratings yet
- Endocrine SystemDocument41 pagesEndocrine SystemMerrin EncarnacionNo ratings yet
- Anterior Pituitary Gland: Fawwaz Ammari Laith & HaniDocument22 pagesAnterior Pituitary Gland: Fawwaz Ammari Laith & HaniRashed ShatnawiNo ratings yet
- SAQ 2nd Week (Thyroid Gland)Document15 pagesSAQ 2nd Week (Thyroid Gland)Josephine BediakoNo ratings yet
- Endocrine SystemDocument30 pagesEndocrine SystemAkshat RastogiNo ratings yet
- Hormones and It's TypesDocument10 pagesHormones and It's TypesSidraNo ratings yet
- HypothyroidismDocument146 pagesHypothyroidismAisha Wadiwala100% (1)
- Endocrine SystemDocument31 pagesEndocrine SystemPreeti ChouhanNo ratings yet
- BB Aminoglycosides VI Sem. 4.04.2021Document44 pagesBB Aminoglycosides VI Sem. 4.04.2021Gunjan KalyaniNo ratings yet
- Endocrine System: Endocrine: Which Have No Duct and ReleaseDocument36 pagesEndocrine System: Endocrine: Which Have No Duct and Releasedr_saleh77No ratings yet
- Endocrine System ProvidedDocument73 pagesEndocrine System Providedummezainhumayra11No ratings yet
- Activity70 HypopituitarismDocument8 pagesActivity70 HypopituitarismJohanna Recca MarinoNo ratings yet
- 11 - Chem Coordination and Integration PDFDocument37 pages11 - Chem Coordination and Integration PDFANo ratings yet
- Unit IXDocument10 pagesUnit IXPreeti ChouhanNo ratings yet
- Anatomy and Physiology Chapter 21 The Sensory SystemDocument34 pagesAnatomy and Physiology Chapter 21 The Sensory SystemThanh Nguyen VanNo ratings yet
- Endocrinal PathologyDocument81 pagesEndocrinal PathologyshehlaNo ratings yet
- System Glands Hormone: NeurotransmittersDocument6 pagesSystem Glands Hormone: NeurotransmittersShaheryar HasanNo ratings yet
- Function and Regulation of Hormones Hormones: Small Lobules of Compound Gland)Document11 pagesFunction and Regulation of Hormones Hormones: Small Lobules of Compound Gland)Ariane-Gay Cristobal DuranNo ratings yet
- CH 45Document9 pagesCH 45homamunfatNo ratings yet
- Hormonal Management of Male InfertilityDocument22 pagesHormonal Management of Male Infertilitydranibalurologoencancun.mxNo ratings yet
- The Endocrine System LabDocument11 pagesThe Endocrine System Lablaike082921100% (1)
- The Pituitary Gland Phamela Joy S. Alvarez Anatomic and Physiologic OverviewDocument27 pagesThe Pituitary Gland Phamela Joy S. Alvarez Anatomic and Physiologic OverviewEdelrose LapitanNo ratings yet
- Endocrine Gland - WikipediaDocument29 pagesEndocrine Gland - WikipediaSumaya FarheenNo ratings yet
- Endocrine ReviewDocument9 pagesEndocrine ReviewSpencer ThomasNo ratings yet
- Lewis: Medical-Surgical Nursing, 10 Edition: Assessment of Endocrine System Key PointsDocument3 pagesLewis: Medical-Surgical Nursing, 10 Edition: Assessment of Endocrine System Key PointsDeo FactuarNo ratings yet
- Endocrine & Reproductive Physiology: Chapter 1: Introduction To Endocrine SystemDocument7 pagesEndocrine & Reproductive Physiology: Chapter 1: Introduction To Endocrine Systemapi-290338101No ratings yet
- Hypothalamus and Pituitary GlandDocument48 pagesHypothalamus and Pituitary GlandMohsin AbbasNo ratings yet
- ENDOCRINE SYSTEM DISORDERS Unit 1Document8 pagesENDOCRINE SYSTEM DISORDERS Unit 1Rizza Mae MaglacionNo ratings yet
- Test Eng. Cu Raspuns 2010Document27 pagesTest Eng. Cu Raspuns 2010Ahmad Abu KushNo ratings yet
- Moldova Courses PDFDocument7 pagesMoldova Courses PDFAhmad Abu KushNo ratings yet
- Cancer and Cell SenescenceDocument2 pagesCancer and Cell SenescenceAhmad Abu KushNo ratings yet
- Eng Red Act Ate 2012Document17 pagesEng Red Act Ate 2012Ahmad Abu KushNo ratings yet
- Peculiarities of Pediatric Surgical PatientDocument19 pagesPeculiarities of Pediatric Surgical PatientAhmad Abu KushNo ratings yet
- Test Eng. Cu Raspuns 2010Document27 pagesTest Eng. Cu Raspuns 2010Ahmad Abu KushNo ratings yet
- Neonatal Surgical InfectionDocument43 pagesNeonatal Surgical InfectionAhmad Abu KushNo ratings yet
- Congental Abdominal Wall DefectsDocument38 pagesCongental Abdominal Wall DefectsAhmad Abu KushNo ratings yet
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesDocument83 pagesAtherosclerosis, Dyslipidaemia and Diabetes SlidesTatiana GobjilăNo ratings yet
- Mal RotationDocument29 pagesMal RotationAhmad Abu KushNo ratings yet
- Imperforate Anus and Cloacal MalformationsDocument110 pagesImperforate Anus and Cloacal MalformationsAhmad Abu KushNo ratings yet
- Hypertrophic Pyloric StenosisDocument28 pagesHypertrophic Pyloric StenosisAhmad Abu Kush100% (2)
- Intestinal Atresias, Obstructions, WebsDocument59 pagesIntestinal Atresias, Obstructions, WebsAhmad Abu KushNo ratings yet
- IntussusceptionDocument60 pagesIntussusceptionAhmad Abu KushNo ratings yet
- Hirschsprung DiseaseDocument44 pagesHirschsprung DiseaseAhmad Abu KushNo ratings yet
- Bacterial Destruction of The LungsDocument46 pagesBacterial Destruction of The LungsAhmad Abu KushNo ratings yet
- Congenital Lung MalformationsDocument115 pagesCongenital Lung MalformationsAhmad Abu KushNo ratings yet
- Ginecologie An.v EngDocument67 pagesGinecologie An.v EngAhmad Abu KushNo ratings yet
- Tematica Eng 2013Document6 pagesTematica Eng 2013Ahmad Abu KushNo ratings yet
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesDocument83 pagesAtherosclerosis, Dyslipidaemia and Diabetes SlidesTatiana GobjilăNo ratings yet
- PG Eng CoursDocument96 pagesPG Eng CoursAhmad Abu KushNo ratings yet
- Questions For Exam in GYNECOLOGYDocument3 pagesQuestions For Exam in GYNECOLOGYAhmad Abu KushNo ratings yet
- DRENGDocument19 pagesDRENGAhmad Abu KushNo ratings yet
- DozeDocument3 pagesDozeAhmad Abu KushNo ratings yet
- 5Document14 pages5Ahmad Abu KushNo ratings yet
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesDocument83 pagesAtherosclerosis, Dyslipidaemia and Diabetes SlidesTatiana GobjilăNo ratings yet
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesDocument83 pagesAtherosclerosis, Dyslipidaemia and Diabetes SlidesTatiana GobjilăNo ratings yet
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesDocument83 pagesAtherosclerosis, Dyslipidaemia and Diabetes SlidesTatiana GobjilăNo ratings yet
- IndicatiiDocument1 pageIndicatiiAhmad Abu KushNo ratings yet
- Assessment and Management of Patients With Endocrine DisordersDocument91 pagesAssessment and Management of Patients With Endocrine DisordersAirme Raz AlejandroNo ratings yet
- Endocrine Answer KeyDocument10 pagesEndocrine Answer KeyJoyce LimNo ratings yet
- Serum ElectrolyteDocument6 pagesSerum ElectrolyteShubham PandeyNo ratings yet
- Extrarenal Effects of Aldosterone On Potassium HomeostasisDocument8 pagesExtrarenal Effects of Aldosterone On Potassium HomeostasisKhánh Nguyễn NgọcNo ratings yet
- Gangguan Dan Keseimbangan Cairan Dan ElektrolitDocument37 pagesGangguan Dan Keseimbangan Cairan Dan ElektrolitFyana PutriNo ratings yet
- Jama Hta ResistenteDocument9 pagesJama Hta ResistenteMayra Alejandra Prada SerranoNo ratings yet
- A-Level Coordination (Kugonza)Document41 pagesA-Level Coordination (Kugonza)kasumbaashraf3No ratings yet
- Fluids and ElectrolytesDocument102 pagesFluids and Electrolytesfelxhu50% (2)
- SGLT2Document14 pagesSGLT2Rezultate DMD ElytisNo ratings yet
- Adrenal Gland by DR Rajnee Ist PartDocument29 pagesAdrenal Gland by DR Rajnee Ist Part9460106212No ratings yet
- Electrolytes and Acid Base Common Fluid and Enlectrolyte DisordersDocument9 pagesElectrolytes and Acid Base Common Fluid and Enlectrolyte Disordersninta karinaNo ratings yet
- Question of TH Week 2020 NBCRNADocument23 pagesQuestion of TH Week 2020 NBCRNACristianFranceschi100% (1)
- Fluid Volume BalanceDocument73 pagesFluid Volume BalanceSalman HabeebNo ratings yet
- Functions of The Mineralocorticoids Aldosterone Reg of Ald SecretDocument5 pagesFunctions of The Mineralocorticoids Aldosterone Reg of Ald SecretEstellaNo ratings yet
- ExamDocument8 pagesExamfatiNo ratings yet
- Aldosterone ELISA: Instructions For UseDocument39 pagesAldosterone ELISA: Instructions For UseYousra ZeidanNo ratings yet
- MedSurg Group2Document4 pagesMedSurg Group2Lacangan, Thea YvonneNo ratings yet
- Case StudyDocument10 pagesCase StudyJib SinsuatNo ratings yet
- Adrenal Gland: Structure, Hormones and Clinical Disorders-: Professor Dr. Najat A. HasanDocument18 pagesAdrenal Gland: Structure, Hormones and Clinical Disorders-: Professor Dr. Najat A. HasanDrFarah Emad Ali100% (1)
- Kuliah Patofisiologi Trauma - DR Raden Ajeng Sri WulandariDocument22 pagesKuliah Patofisiologi Trauma - DR Raden Ajeng Sri WulandariAgung Budi SuristioNo ratings yet
- Fluid, Electrolyte and Acid-Base Homeostasis (Renal)Document36 pagesFluid, Electrolyte and Acid-Base Homeostasis (Renal)xarae23No ratings yet
- Diagnostic MedlabDocument585 pagesDiagnostic MedlabKiko KiwiblokeNo ratings yet
- Endocrine System Anatomy and PhysiologyDocument17 pagesEndocrine System Anatomy and PhysiologyKBD0% (1)
- Biochem Final Exam MCQs PDFDocument173 pagesBiochem Final Exam MCQs PDFzeeshan jaskaniNo ratings yet
- ENDOCRINE 1.3 Incidentallomas, Conn's SyndromeDocument5 pagesENDOCRINE 1.3 Incidentallomas, Conn's SyndromeJem QuintoNo ratings yet
- TáchDocument18 pagesTáchQuỳnh TrâmNo ratings yet
- Summary of Product Characteristics, Labelling and Package LeafletDocument29 pagesSummary of Product Characteristics, Labelling and Package LeafletImmanuel PurbaNo ratings yet
- 1-Adrenocorticosteroids Chapter39Document94 pages1-Adrenocorticosteroids Chapter39hamidNo ratings yet
- TUGAS 5 B.INGGRIS TigaDocument3 pagesTUGAS 5 B.INGGRIS TigaMesya FauziahNo ratings yet