You might also like
- Honda Accord 95Document2 pagesHonda Accord 95ejg26No ratings yet
- Case StudyDocument2 pagesCase Studyejg26No ratings yet
- Facebook or Facing Your BookDocument2 pagesFacebook or Facing Your Bookejg26No ratings yet
- Chain of InfectionDocument2 pagesChain of Infectionejg26No ratings yet
- Theresa J. Llanes: ObjectiveDocument2 pagesTheresa J. Llanes: Objectiveejg26No ratings yet
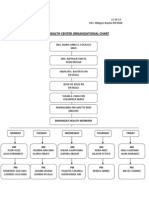
- Health Center: Organizational Chart Ampid 1 San Mateo, RizalDocument1 pageHealth Center: Organizational Chart Ampid 1 San Mateo, Rizalejg26No ratings yet
- Freuds Psychosexual Stages of Development Oral StageDocument8 pagesFreuds Psychosexual Stages of Development Oral Stageejg26No ratings yet
- Empire of The Sun Soc 18Document3 pagesEmpire of The Sun Soc 18ejg26No ratings yet
- Dopa DobuDocument2 pagesDopa Dobuejg26No ratings yet
- Movie Reports DutyVLDocument9 pagesMovie Reports DutyVLejg26No ratings yet
- Purposes of SurgeryDocument2 pagesPurposes of Surgeryejg26No ratings yet
- Aaron Learning InsightsDocument1 pageAaron Learning Insightsejg26No ratings yet
- Intake and Output Monitoring Sheet: Date TimeDocument3 pagesIntake and Output Monitoring Sheet: Date Timeejg26No ratings yet
- Nursing Informatics in CanadaDocument25 pagesNursing Informatics in Canadaejg26No ratings yet
- Anti Tuberculosis AgentsDocument15 pagesAnti Tuberculosis Agentsejg26100% (1)
- Ketorolac Drug StudyDocument1 pageKetorolac Drug Studyejg26No ratings yet
- Rarejob Endorsement Letter For BpiDocument1 pageRarejob Endorsement Letter For Bpiejg26100% (2)
- Report Sa Informatics!Document13 pagesReport Sa Informatics!ejg26No ratings yet
- QuizDocument2 pagesQuizejg26No ratings yet
- Roosevelt College System Institute of Nursing and Health Education Sumulong Highway Cainta, RizalDocument2 pagesRoosevelt College System Institute of Nursing and Health Education Sumulong Highway Cainta, Rizalejg26No ratings yet
- Roosevelt College System Institute of Nursing and Health Education Sumulong Highway Cainta, RizalDocument1 pageRoosevelt College System Institute of Nursing and Health Education Sumulong Highway Cainta, Rizalejg26No ratings yet
- FNCP Health Center ChartDocument1 pageFNCP Health Center Chartejg26No ratings yet
- FNCP Barangay ChartDocument1 pageFNCP Barangay Chartejg26No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Mifepristone & Misoprostol Dosing Chart 2023Document1 pageMifepristone & Misoprostol Dosing Chart 2023Iriawan Indra PutraNo ratings yet
- Rett SyndromeDocument55 pagesRett SyndromeSnezana MihajlovicNo ratings yet
- Bronchiolitis in Infants and Children - Upto-Date 2015Document15 pagesBronchiolitis in Infants and Children - Upto-Date 2015Gerardo MansillaNo ratings yet
- Question NurseDocument240 pagesQuestion NurseKaye PatanindagatNo ratings yet
- Feto Pelvic DisproportionDocument10 pagesFeto Pelvic DisproportionIsrael WoseneNo ratings yet
- Lawsuit Against Small Smiles Dental Center Aka Alabany Access Dental Center Et. Al.Document52 pagesLawsuit Against Small Smiles Dental Center Aka Alabany Access Dental Center Et. Al.DebHgnNo ratings yet
- Lesson 5: Role of Informatics Nurse SpecialistDocument9 pagesLesson 5: Role of Informatics Nurse SpecialistJerica Jaz F. Vergara100% (1)
- Letter and Nurse)Document2 pagesLetter and Nurse)ruggero07No ratings yet
- WS 1Q - PHYSICAL EDUCATION With PagesDocument14 pagesWS 1Q - PHYSICAL EDUCATION With PagesJellie Delos ReyesNo ratings yet
- Shaukat Khanum Memorial Cancer Hospital & Research Centre: Coagulation ProfileDocument1 pageShaukat Khanum Memorial Cancer Hospital & Research Centre: Coagulation ProfileSyed Muhammad Zubair TariqNo ratings yet
- Abortions in Dairy Cows PDFDocument4 pagesAbortions in Dairy Cows PDFransinghNo ratings yet
- CMN 463 Lecture 2 Insurance Medicare and MedicaidDocument18 pagesCMN 463 Lecture 2 Insurance Medicare and MedicaidCarlos GuiterizNo ratings yet
- NI Final ExamDocument7 pagesNI Final ExamJoseph Burra LagodNo ratings yet
- Establishment of Bangamata National Cellular and Molecular Research CenterDocument5 pagesEstablishment of Bangamata National Cellular and Molecular Research CenterMosaddak100% (1)
- Test Bank For Introduction To Critical Care Nursing 5th Edition Mary Lou SoleDocument9 pagesTest Bank For Introduction To Critical Care Nursing 5th Edition Mary Lou Solemammonphysics2e1.w4No ratings yet
- Pre Test Health Assessment and The NurseDocument4 pagesPre Test Health Assessment and The NurseAileen A. MonaresNo ratings yet
- AttbDocument6 pagesAttbmuiz_travxNo ratings yet
- UNAS Ob Surabaya 2017Document31 pagesUNAS Ob Surabaya 2017Zurya UdayanaNo ratings yet
- Kesihatan Pergigian Warga Emas: DR Hirzi B Kamaludin KP TG TualangDocument46 pagesKesihatan Pergigian Warga Emas: DR Hirzi B Kamaludin KP TG TualangAvina Anin NasiaNo ratings yet
- Uterine Leiomyoma: Case ReportDocument16 pagesUterine Leiomyoma: Case Reportangie riveraNo ratings yet
- The Infectious Hazards of Dead BodiesDocument3 pagesThe Infectious Hazards of Dead Bodiespenn hicksNo ratings yet
- Ankle-Brachial Index-3 PDFDocument9 pagesAnkle-Brachial Index-3 PDFSarah HalanNo ratings yet
- Ectopic Pregnancy Student LectureDocument19 pagesEctopic Pregnancy Student Lectureapi-370504650% (4)
- Aceclofenac Efficacy and Safety Vs DiclofenacDocument6 pagesAceclofenac Efficacy and Safety Vs DiclofenacpdelaxNo ratings yet
- Doctors N Chemist ListDocument19 pagesDoctors N Chemist ListJaggu TigerNo ratings yet
- Paramount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceDocument2 pagesParamount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceVasudevan KunjithapathamNo ratings yet
- Pressure Ulcer Prevention in Long Term CareDocument6 pagesPressure Ulcer Prevention in Long Term CareambariyantoNo ratings yet
- RetinopathyDocument64 pagesRetinopathySiti NcitNo ratings yet
- Chronic Kidney Disease (PSN) 03Document28 pagesChronic Kidney Disease (PSN) 03Logia LegisNo ratings yet
- NCP PneuDocument3 pagesNCP PneuRichelle Sandriel C. de CastroNo ratings yet