You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Muara Bulian Jambi Puskesmas Muara Bulian Sumatra PsksDocument1 pageMuara Bulian Jambi Puskesmas Muara Bulian Sumatra Pskshp inventNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Myiasis: Fabio Francesconi and Omar LupiDocument27 pagesMyiasis: Fabio Francesconi and Omar Lupihp inventNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- AsadadadacDocument1 pageAsadadadachp inventNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Muara Bulian Jambi Puskesmas Muara BulianDocument1 pageMuara Bulian Jambi Puskesmas Muara Bulianhp inventNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Muara Bulian Jambi PuskesmasDocument1 pageMuara Bulian Jambi Puskesmashp inventNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Muara Bulian Jambi Puskesmas Muara Bulian SumatraDocument1 pageMuara Bulian Jambi Puskesmas Muara Bulian Sumatrahp inventNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Muara BulianDocument1 pageMuara Bulianhp inventNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Sindrom MetabolikDocument2 pagesSindrom MetabolikMelisha L. Gaya100% (1)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Aplication LettersDocument1 pageAplication Lettershp inventNo ratings yet
- Muara BulianDocument1 pageMuara Bulianhp inventNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Bab 128 Nefritis LupusDocument6 pagesBab 128 Nefritis Lupushp inventNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Bab 125 GlomerulonefritisDocument4 pagesBab 125 Glomerulonefritishp inventNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Bab 428 Koma Hiperosmolar Hiperglikemik Non KetotikDocument3 pagesBab 428 Koma Hiperosmolar Hiperglikemik Non KetotikLhandd'smartAlexander BbfplusmeofChibyNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- CaseDocument2 pagesCasehp inventNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Atrial Natriuretic PeptideDocument1 pageAtrial Natriuretic Peptidehp inventNo ratings yet
- Bab 394 KoleraDocument4 pagesBab 394 KoleraSyafril LubisNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Influence of Hepatitis B Immunization To Prevent Vertical Transmission of Hep-B Virus in Infants Born From Hep-B Positive MotherDocument5 pagesInfluence of Hepatitis B Immunization To Prevent Vertical Transmission of Hep-B Virus in Infants Born From Hep-B Positive MotherHartonoNo ratings yet
- JOI Vol 7 No 5 Juni 2011 (Dewi R)Document6 pagesJOI Vol 7 No 5 Juni 2011 (Dewi R)hp inventNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Bab 67 Gangguan Motilitas Saluran Cerna Bagian BawahDocument4 pagesBab 67 Gangguan Motilitas Saluran Cerna Bagian Bawahhp inventNo ratings yet
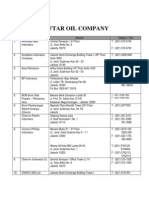
- Daftar Dan Alamat Oil CompanyDocument16 pagesDaftar Dan Alamat Oil Companysetia wirawan100% (7)
- JOI Vol 7 No 5 Juni 2011 (Reni P)Document4 pagesJOI Vol 7 No 5 Juni 2011 (Reni P)Syahrial Laskar PelangiNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Vitamin A Untuk Diare AkutDocument7 pagesVitamin A Untuk Diare AkutPandu AnggoroNo ratings yet
- ProsperDocument3 pagesProsperhp inventNo ratings yet
- He Modi NamikDocument16 pagesHe Modi Namikhp inventNo ratings yet
- PemainDocument13 pagesPemainhp inventNo ratings yet
- Dubowitz ScoreDocument3 pagesDubowitz ScorentadudulNo ratings yet
- Determination Normal Reference Value Conventional Units SI Units Blood, Plasma or SerumDocument12 pagesDetermination Normal Reference Value Conventional Units SI Units Blood, Plasma or Serumhp inventNo ratings yet
- Nutrition & Growth 1Document70 pagesNutrition & Growth 1hp inventNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Faktor Resiko DM Type 2Document3 pagesFaktor Resiko DM Type 2hp inventNo ratings yet
- Sample Research About Teenage Pregnancy - NEUDocument53 pagesSample Research About Teenage Pregnancy - NEUAndy Lalu100% (3)
- Eng8 - Q3 - Module3Determining Various Social, Moral, and Economic Issues in A Text Listened To V3Document30 pagesEng8 - Q3 - Module3Determining Various Social, Moral, and Economic Issues in A Text Listened To V3Julius Salas0% (1)
- Local Media5535365952530108777Document16 pagesLocal Media5535365952530108777GYNKY MONTERDENo ratings yet
- University of Ghana Http://ugspace - Ug.edu - GHDocument83 pagesUniversity of Ghana Http://ugspace - Ug.edu - GHajNo ratings yet
- What Is Multicultural Education?: Contemporary Issues Related To Multicultural FunctioningDocument4 pagesWhat Is Multicultural Education?: Contemporary Issues Related To Multicultural FunctioningClaudine Christiane Caparas - HemedezNo ratings yet
- National Health Situation of Maternal and Child Health NursingDocument11 pagesNational Health Situation of Maternal and Child Health NursingNiña Ricci MtflcoNo ratings yet
- Malawi Youth Policy PDFDocument10 pagesMalawi Youth Policy PDFDayyanealosNo ratings yet
- Kate Valerie Quiban - OrangeDocument5 pagesKate Valerie Quiban - OrangeKate QuibanNo ratings yet
- SpeechDocument1 pageSpeechSheryl BorromeoNo ratings yet
- RRLDocument2 pagesRRLJohn Smith60% (5)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- BBCunderageandpregnant PDFDocument124 pagesBBCunderageandpregnant PDFmarielaNo ratings yet
- Teen Pregnancy - HoniaraDocument33 pagesTeen Pregnancy - HoniaraMillenium Ayurveda80% (5)
- ThesissssDocument30 pagesThesissssPearl Joy Villagomeza IINo ratings yet
- Teenage Pregnancies in The Philippines 2Document5 pagesTeenage Pregnancies in The Philippines 2Tweetie Sabado83% (29)
- Practical Research 1Document7 pagesPractical Research 1Ron Marc MarananNo ratings yet
- 38160Document13 pages38160Jessa Esperanza SorioNo ratings yet
- Chapter 1-1Document8 pagesChapter 1-1Caroline ValenzuelaNo ratings yet
- Music Group Overview CalaboozDocument5 pagesMusic Group Overview CalaboozKaytee SilverNo ratings yet
- Students Are Allowed To Use Mobile Phones Inside The Campus: Good, But in Moderation"Document10 pagesStudents Are Allowed To Use Mobile Phones Inside The Campus: Good, But in Moderation"Robert GarciaNo ratings yet
- 06 Chapter 5Document10 pages06 Chapter 5Gie Marie Francisco UmaliNo ratings yet
- Group 1 FInalDocument53 pagesGroup 1 FInalAljeya EvanchezNo ratings yet
- Swot Analysis On Youth BillsDocument7 pagesSwot Analysis On Youth BillsRosechelan Acorda-AdongayNo ratings yet
- Sample of Research Paper About Teenage PregnancyDocument7 pagesSample of Research Paper About Teenage Pregnancygz9avm26No ratings yet
- Nutrition of Adolescent Girls in Low and Middle Income CountriesDocument12 pagesNutrition of Adolescent Girls in Low and Middle Income CountriesmanalNo ratings yet
- Sex Education Boon or BaneDocument40 pagesSex Education Boon or BaneAlex ManiboNo ratings yet
- Dinda Amalia Shaleha (019.06.0022) Exercise by Mrs. Nurul InayahDocument3 pagesDinda Amalia Shaleha (019.06.0022) Exercise by Mrs. Nurul InayahDinda Amalia SNo ratings yet
- Teen PregnancyDocument4 pagesTeen PregnancyJoshua PicartNo ratings yet
- Review of Related Literature: Research TitleDocument3 pagesReview of Related Literature: Research TitleDharlyn AlmonteNo ratings yet
- Essaytigers Expository Essay SampleDocument3 pagesEssaytigers Expository Essay SampleJamie GernerNo ratings yet
- The Correlation With Pornographic Exposure and Teenage PregnancyDocument3 pagesThe Correlation With Pornographic Exposure and Teenage PregnancySIEG The FREEDNo ratings yet
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- What to Expect When You’re Expecting (5th Edition)From EverandWhat to Expect When You’re Expecting (5th Edition)Rating: 5 out of 5 stars5/5 (1)
- Healing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeFrom EverandHealing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeNo ratings yet
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)