You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Chronic Pain Management Fact SheetDocument2 pagesChronic Pain Management Fact SheetAdvaMedLCINo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Infographic: IMPACT OF HEART DISEASEDocument1 pageInfographic: IMPACT OF HEART DISEASEAdvaMedLCINo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
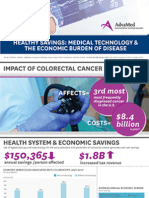
- Infographic: IMPACT OF COLORECTAL CANCERDocument1 pageInfographic: IMPACT OF COLORECTAL CANCERAdvaMedLCINo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- 2015 Innovation AgendaDocument1 page2015 Innovation AgendaAdvaMedLCINo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Innovation Agenda: February 2015Document4 pagesInnovation Agenda: February 2015AdvaMedLCINo ratings yet
- Pulse Redefining Medical Technology InnovationDocument64 pagesPulse Redefining Medical Technology InnovationAdvaMedLCINo ratings yet
- The Anatomy of Medical ResearchDocument16 pagesThe Anatomy of Medical ResearchAdvaMedLCI0% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Innovation Scorecard - Report FINAL - External UNSECUREDDocument50 pagesInnovation Scorecard - Report FINAL - External UNSECUREDAdvaMedLCINo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Oct 2012 King Report FINALDocument16 pagesOct 2012 King Report FINALAdvaMedLCINo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Group 7 Worksheet No. 1 2Document24 pagesGroup 7 Worksheet No. 1 2calliemozartNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- What Is Emergency ManagementDocument8 pagesWhat Is Emergency ManagementHilina hailuNo ratings yet
- Rediscovering Alginate Wound DressingsDocument4 pagesRediscovering Alginate Wound DressingstanveerhusseinNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Wada Defending Cannabis BanDocument18 pagesWada Defending Cannabis Banada UnknownNo ratings yet
- Factory OverheadDocument2 pagesFactory OverheadKeanna Denise GonzalesNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Narrative ReporDocument3 pagesNarrative ReporMARK LUKE ULITNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Athletes Who Made Amazing Comebacks After Career-Threatening InjuriesDocument11 pagesAthletes Who Made Amazing Comebacks After Career-Threatening InjuriesანაNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Cape 2 Biology - Homeostasis &excretionDocument9 pagesCape 2 Biology - Homeostasis &excretionTamicka BonnickNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Edgie A. Tenerife BSHM 1108: Page 1 of 4Document4 pagesEdgie A. Tenerife BSHM 1108: Page 1 of 4Edgie TenerifeNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Cheap TBE Inverter TeardownsDocument33 pagesCheap TBE Inverter TeardownsWar Linux92% (12)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pentacam Four Maps RefractiveDocument4 pagesPentacam Four Maps RefractiveSoma AlshokriNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Gloria Pfoltzer Theresa Morris, an Infant, by Mother and Next Friend Christopher Morris, an Infant, by Mother and Next Friend Randy Morris, an Infant, by Mother and Next Friend v. Fairfax County Department of Human Development Susan Manzo Paulette Byrd Florence Hannigan, and Louis Villafane, 966 F.2d 1443, 4th Cir. (1992)Document10 pagesGloria Pfoltzer Theresa Morris, an Infant, by Mother and Next Friend Christopher Morris, an Infant, by Mother and Next Friend Randy Morris, an Infant, by Mother and Next Friend v. Fairfax County Department of Human Development Susan Manzo Paulette Byrd Florence Hannigan, and Louis Villafane, 966 F.2d 1443, 4th Cir. (1992)Scribd Government DocsNo ratings yet
- Grain Silo Storage SizesDocument8 pagesGrain Silo Storage SizesTyler HallNo ratings yet
- Private Standard: Shahram GhanbarichelaresiDocument2 pagesPrivate Standard: Shahram Ghanbarichelaresiarian tejaratNo ratings yet
- 0010 kOBELCO SK 179-9 PDFDocument52 pages0010 kOBELCO SK 179-9 PDFDaman Huri100% (2)
- Ammonia Synthesis ConverterDocument26 pagesAmmonia Synthesis ConverterKvspavan Kumar100% (1)
- The Benefits of RunningDocument1 pageThe Benefits of Runningefendi odidNo ratings yet
- R633199 PDFDocument1 pageR633199 PDFChirag RohitNo ratings yet
- Astm A712 PDFDocument3 pagesAstm A712 PDFCristian OtivoNo ratings yet
- API 614-Chapter 4 DATA SHEET Dry Gas Seal Module Si Units: System Responsibility: (2.1.2)Document10 pagesAPI 614-Chapter 4 DATA SHEET Dry Gas Seal Module Si Units: System Responsibility: (2.1.2)tutuionutNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Posi LokDocument24 pagesPosi LokMarcel Baque100% (1)
- Hydrogen Production From The Air: Nature CommunicationsDocument9 pagesHydrogen Production From The Air: Nature CommunicationsdfdffNo ratings yet
- Technical Publication: Direction 2296441-100 Revision 06 Ge Medical Systems Lightspeed 3.X - Schematics and BoardsDocument380 pagesTechnical Publication: Direction 2296441-100 Revision 06 Ge Medical Systems Lightspeed 3.X - Schematics and BoardsJairo Manzaneda100% (2)
- 2017 THE BLUE WAY Visual PDFDocument54 pages2017 THE BLUE WAY Visual PDFAlex KappelNo ratings yet
- Phenotype and GenotypeDocument7 pagesPhenotype and GenotypeIrish Claire Molina TragicoNo ratings yet
- C 1 WorkbookDocument101 pagesC 1 WorkbookGeraldineNo ratings yet
- Sudheer Kumar CVDocument3 pagesSudheer Kumar CVGujjar Dhayki valeNo ratings yet
- Distribución Del Mercurio Total en Pescados y Mariscos Del Mar ArgentinoDocument15 pagesDistribución Del Mercurio Total en Pescados y Mariscos Del Mar ArgentinoaldiNo ratings yet
- Rahu Yantra Kal Sarp Yantra: Our RecommendationsDocument2 pagesRahu Yantra Kal Sarp Yantra: Our RecommendationsAbhijeet DeshmukkhNo ratings yet
- Brachiocephalic TrunkDocument3 pagesBrachiocephalic TrunkstephNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)