You might also like
- Sciencedirect: Letter To The EditorDocument2 pagesSciencedirect: Letter To The EditorBala BhaskarNo ratings yet
- LeanLab WhitepaperDocument16 pagesLeanLab WhitepaperZoe ShihNo ratings yet
- Automation in The Clinical Microbiology Laboratory PAPERDocument7 pagesAutomation in The Clinical Microbiology Laboratory PAPERobakhit91No ratings yet
- Lean Six Sigma Methodologies Improve Clinical Laboratory Efficiency and Reduce Turnaround TimesDocument5 pagesLean Six Sigma Methodologies Improve Clinical Laboratory Efficiency and Reduce Turnaround TimesVipul SehgalNo ratings yet
- Preanalytical Requirements of Urinalysis: Biochemia Medica February 2014Document17 pagesPreanalytical Requirements of Urinalysis: Biochemia Medica February 2014MARIO ALVARADONo ratings yet
- Int J Lab Hematology - 2021 - Kitchen - International Council For Standardisation in Haematology ICSH Recommendations ForDocument10 pagesInt J Lab Hematology - 2021 - Kitchen - International Council For Standardisation in Haematology ICSH Recommendations ForWidi MarsandaNo ratings yet
- Ajcpath125 0016Document10 pagesAjcpath125 0016Asad AliNo ratings yet
- Laboratory Utilization in The Emergency Department - Are The Requested Tests Patient-Oriented?Document3 pagesLaboratory Utilization in The Emergency Department - Are The Requested Tests Patient-Oriented?djebrutNo ratings yet
- Artículo BiochemDocument16 pagesArtículo BiochemViankis García100% (1)
- Tackling Preanalytical Challenges in Laboratory Automation - Dr. Tjian Sian HwaDocument43 pagesTackling Preanalytical Challenges in Laboratory Automation - Dr. Tjian Sian Hwagonteng sadyogaNo ratings yet
- Chapter 1 Variation Errors and Quality in The Clinical Laboratory 2013 Accurate Results in The Clinical LaboratoryDocument8 pagesChapter 1 Variation Errors and Quality in The Clinical Laboratory 2013 Accurate Results in The Clinical LaboratoryCristina GaidargiNo ratings yet
- Review Article: Pre-Analytical Phase in Clinical Chemistry LaboratoryDocument8 pagesReview Article: Pre-Analytical Phase in Clinical Chemistry Laboratorymuthia aninditaNo ratings yet
- Quality Assurance of Laboratory Results: A Challenge in Health Care ManagementDocument6 pagesQuality Assurance of Laboratory Results: A Challenge in Health Care Managementrizkiyah prabawantiNo ratings yet
- Urine Specimen Collection - How A Multidisciplinary Team Improved Patient Outcomes Using Best Practices - ProQuestDocument9 pagesUrine Specimen Collection - How A Multidisciplinary Team Improved Patient Outcomes Using Best Practices - ProQuestHelmy HanafiNo ratings yet
- Mistakes in A Stat Laboratory: Types and Frequency: Clinical Chemistry September 1997Document5 pagesMistakes in A Stat Laboratory: Types and Frequency: Clinical Chemistry September 1997Othman MaaiNo ratings yet
- Healthcare Is Ripe For Lean: Executive SummaryDocument7 pagesHealthcare Is Ripe For Lean: Executive SummaryANTUANETTE MARIBEL ZEVALLOS BALLADARESNo ratings yet
- Favaloro 2010Document13 pagesFavaloro 2010Yohana SetiawanNo ratings yet
- Plebani 2006Document10 pagesPlebani 2006ami190No ratings yet
- Errors in Clinical Laboratories or Errors in Laboratory Medicine?Document10 pagesErrors in Clinical Laboratories or Errors in Laboratory Medicine?DiegoMaradónNo ratings yet
- Pan American Society For Clinical Virology Position Statement On Fda Oversight of Laboratory-Developed Tests (LDTS)Document5 pagesPan American Society For Clinical Virology Position Statement On Fda Oversight of Laboratory-Developed Tests (LDTS)fdablogNo ratings yet
- Quality Assurance in The Preanalytical PhaseDocument21 pagesQuality Assurance in The Preanalytical PhaseDaniel Huachani CoripunaNo ratings yet
- Sample of TranslationDocument5 pagesSample of Translationmartabak_polkadotNo ratings yet
- Policy Phlebotomy Blood CollectionDocument6 pagesPolicy Phlebotomy Blood CollectionmuhammadhanifmohdfahmiNo ratings yet
- Rato - Quality of Specimen NotesDocument5 pagesRato - Quality of Specimen NotesAileen SacayNo ratings yet
- Linical Aboratory O: S H, MT (Ascp) SH B A. K, E D, Mls (Ascp), Cls (Nca)Document5 pagesLinical Aboratory O: S H, MT (Ascp) SH B A. K, E D, Mls (Ascp), Cls (Nca)Tito LeopardoNo ratings yet
- Guide To Infection Control in The HospitalDocument14 pagesGuide To Infection Control in The Hospitalsyaiful rinantoNo ratings yet
- Three Years' Experience of Quality Monitoring Program On Pre-Analytical Errors in ChinaDocument7 pagesThree Years' Experience of Quality Monitoring Program On Pre-Analytical Errors in ChinaCenyiqanita NurqanitaNo ratings yet
- Laboratory Quality Control Based On Risk ManagementDocument6 pagesLaboratory Quality Control Based On Risk ManagementRafi UdeenNo ratings yet
- Original Papers: Specimen Rejection in Laboratory Medicine: Necessary For Patient Safety?Document9 pagesOriginal Papers: Specimen Rejection in Laboratory Medicine: Necessary For Patient Safety?KKay LaminNo ratings yet
- Articulo 2810Document5 pagesArticulo 2810cyfra.laboratorioNo ratings yet
- Ajcpath140 0193Document10 pagesAjcpath140 0193Marinelle TumanguilNo ratings yet
- Internal Quality Control Practices in Coagulation LaboratoriesDocument10 pagesInternal Quality Control Practices in Coagulation LaboratoriesMy LeNo ratings yet
- Ce (Ad) F (Is) Pf1 (Aka SS) Pfa (SS) PN (SS)Document4 pagesCe (Ad) F (Is) Pf1 (Aka SS) Pfa (SS) PN (SS)marvel ecstasyNo ratings yet
- The Impact of Laboratory Automation On Performance ImprovementDocument6 pagesThe Impact of Laboratory Automation On Performance ImprovementChris V-PandaNo ratings yet
- Errors in Clinical Laboratories or Errors in Laboratory MedicineDocument11 pagesErrors in Clinical Laboratories or Errors in Laboratory MedicineShahid HussainNo ratings yet
- Lot-To-Lot Variation and Verification - cclm-2022-1126Document8 pagesLot-To-Lot Variation and Verification - cclm-2022-1126Georgiana Daniela DragomirNo ratings yet
- JLP 10 237Document4 pagesJLP 10 237Nur Muhammad IsmatullohNo ratings yet
- Selecting Automation For The Clinical Chemistry LaboratoryDocument7 pagesSelecting Automation For The Clinical Chemistry LaboratoryFathul WiandaruNo ratings yet
- Gestión de Las Fases de Pre y Post-Analítica de La PDFDocument12 pagesGestión de Las Fases de Pre y Post-Analítica de La PDFUlises Saldías RoaNo ratings yet
- Errores en La Fase PreanalíticaDocument4 pagesErrores en La Fase PreanalíticaYaquelin VelasquezNo ratings yet
- VITROS Chemistry Systems PDFDocument4 pagesVITROS Chemistry Systems PDFdatitoxNo ratings yet
- Bertholf2017 Chapter LaboratoryStructureAndFunctionDocument23 pagesBertholf2017 Chapter LaboratoryStructureAndFunctionci8084102No ratings yet
- 2014-1107 Call For DiagnosticsDocument3 pages2014-1107 Call For Diagnosticsdipys41No ratings yet
- UK Lab Survey ReportDocument8 pagesUK Lab Survey ReportGunesh DeosthaliNo ratings yet
- POCTDocument24 pagesPOCTHiminNo ratings yet
- Case Study ST HelensDocument2 pagesCase Study ST HelensQuoc Ty TranNo ratings yet
- Automation of Dissolution TestsDocument9 pagesAutomation of Dissolution TestsAli RizviNo ratings yet
- 8163-Article Text-29935-1-10-20110805Document3 pages8163-Article Text-29935-1-10-20110805Wa Nur Arlin RahmadhantyNo ratings yet
- Script - Seminar ReportingDocument4 pagesScript - Seminar ReportingLYNNE ORDONEZNo ratings yet
- JACEP Open - 2020 - Mulcrone - Reducing Infant Catheterization in The Emergency Department Through Clean Catch UrineDocument9 pagesJACEP Open - 2020 - Mulcrone - Reducing Infant Catheterization in The Emergency Department Through Clean Catch UrineoctawyanaNo ratings yet
- Evaluation & Control of Pre Analytical Errors in Required Quality Variables of Clinical Lab ServicesDocument18 pagesEvaluation & Control of Pre Analytical Errors in Required Quality Variables of Clinical Lab ServicesIOSRjournalNo ratings yet
- Forum - Test SafetyDocument2 pagesForum - Test SafetyhhhNo ratings yet
- JOURNAL Errors in Clinical Laboratories or Errors in LaboratoryDocument11 pagesJOURNAL Errors in Clinical Laboratories or Errors in LaboratoryVincent ReyesNo ratings yet
- CCLM 2015 - Local Validation of Blood Collection Tubes 2Document6 pagesCCLM 2015 - Local Validation of Blood Collection Tubes 2richardNo ratings yet
- Essais Cliniques Decentralises VF enDocument15 pagesEssais Cliniques Decentralises VF enSchmoutNo ratings yet
- Quality Assurance in The Microbiology Laboratory: Dermot HayesDocument6 pagesQuality Assurance in The Microbiology Laboratory: Dermot HayesgiuseppegnrNo ratings yet
- Pharmaceutical Sciences: Frequency of Pre-Analytical Phase Errors in A Clinical Chemistry LaboratoryDocument4 pagesPharmaceutical Sciences: Frequency of Pre-Analytical Phase Errors in A Clinical Chemistry LaboratoryAyesha MehmoodNo ratings yet
- The Preanalytical Phase - Past Present and Future.: Annals of Clinical BiochemistryDocument9 pagesThe Preanalytical Phase - Past Present and Future.: Annals of Clinical BiochemistryArturo Eduardo Huarcaya OntiverosNo ratings yet
- JOURNAL The Preanalytical Phase - Past, Present, and FutureDocument3 pagesJOURNAL The Preanalytical Phase - Past, Present, and FutureVincent ReyesNo ratings yet
- A Tale of Two LibrariansDocument4 pagesA Tale of Two LibrariansNancy FriesNo ratings yet
- Pegasus Band ArticleDocument1 pagePegasus Band ArticleNancy FriesNo ratings yet
- The Boarding School ExperienceDocument2 pagesThe Boarding School ExperienceNancy FriesNo ratings yet
- Sage Hill School 2012 Multicultural Fair Press KitDocument6 pagesSage Hill School 2012 Multicultural Fair Press KitNancy FriesNo ratings yet
- Troop ArticleDocument4 pagesTroop ArticleNancy FriesNo ratings yet
- Multicultural Fair Press Release 3.14.11Document5 pagesMulticultural Fair Press Release 3.14.11Nancy FriesNo ratings yet
- Coast Kids Article: "So Stressed"Document1 pageCoast Kids Article: "So Stressed"Nancy FriesNo ratings yet
- Hello Mudda, Hello FaddaDocument4 pagesHello Mudda, Hello FaddaNancy FriesNo ratings yet
- Parenting DilemmasDocument3 pagesParenting DilemmasNancy FriesNo ratings yet
- Pegasus Stays True To Its Roots: Vision Continues To Drive ProgressDocument8 pagesPegasus Stays True To Its Roots: Vision Continues To Drive ProgressNancy FriesNo ratings yet
- ABB REL5xx RIOConverterDocument10 pagesABB REL5xx RIOConverterzinab90100% (1)
- Chapter 1: INTRODUCTION: 1.1 BackgroundDocument5 pagesChapter 1: INTRODUCTION: 1.1 BackgroundAhsan azizNo ratings yet
- Lab No 8Document5 pagesLab No 8LO Ver JG100% (1)
- Microsoft SQL DatabaseDocument401 pagesMicrosoft SQL Databasemtamilmani50% (2)
- SPIN-Energy Efficiency & Urban Development PlanningDocument45 pagesSPIN-Energy Efficiency & Urban Development PlanningEvropski Projekti Savski VenacNo ratings yet
- Thesis FYPDocument50 pagesThesis FYPEyka ZulaikaNo ratings yet
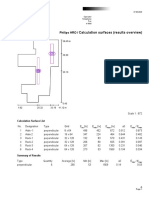
- Calculation Surfaces (Results Overview) : Philips HRODocument4 pagesCalculation Surfaces (Results Overview) : Philips HROsanaNo ratings yet
- 4wd SystemDocument31 pages4wd SystemManuales Transmisiones AutomaticasNo ratings yet
- Installation InstructionsDocument3 pagesInstallation InstructionsRosaLovaNo ratings yet
- 01-RH124 Red Hat System Administration IIDocument4 pages01-RH124 Red Hat System Administration IIpimentel-diogo2056No ratings yet
- Linear ProgrammingDocument6 pagesLinear ProgrammingabeerNo ratings yet
- MagnetostictiveDocument17 pagesMagnetostictivekanikasharma22No ratings yet
- Notes On Foam From SFPE HandbookDocument10 pagesNotes On Foam From SFPE HandbookkdsessionsNo ratings yet
- 08 - Relief System Adequacy - A Step Towards SAFER Operations - Deepak - IngeneroDocument40 pages08 - Relief System Adequacy - A Step Towards SAFER Operations - Deepak - IngeneroCalNo ratings yet
- Sample Problem #8Document8 pagesSample Problem #8DozdiNo ratings yet
- Resume Executive Summary ExampleDocument5 pagesResume Executive Summary ExampleSathish GunasekarNo ratings yet
- Binary Code PowerPoint TemplateDocument36 pagesBinary Code PowerPoint TemplateAbhinand AdhiNo ratings yet
- Sao Paulo Brand BookDocument104 pagesSao Paulo Brand Booknicoagudelo82No ratings yet
- OpenCV 3.0 Computer Vision With Java - Sample ChapterDocument27 pagesOpenCV 3.0 Computer Vision With Java - Sample ChapterPackt PublishingNo ratings yet
- Pumps: Vane Type Single PumpsDocument2 pagesPumps: Vane Type Single PumpsFernando SabinoNo ratings yet
- Maintenance and Repair Instructions TM 124/11: Spring-Applied Sliding Caliper Brake FSG110 With Hub CenteringDocument11 pagesMaintenance and Repair Instructions TM 124/11: Spring-Applied Sliding Caliper Brake FSG110 With Hub CenteringNik100% (1)
- 90 61 085 Transportation ValvesDocument18 pages90 61 085 Transportation ValvesarrikanNo ratings yet
- Ingrid Olderock La Mujer de Los Perros by Nancy GuzmnDocument14 pagesIngrid Olderock La Mujer de Los Perros by Nancy GuzmnYuki Hotaru0% (3)
- Blender 04Document38 pagesBlender 04Ana Maria100% (1)
- Software Project Engineer in Richland Kennewick Pasco WA Resume Robert VeklotzDocument2 pagesSoftware Project Engineer in Richland Kennewick Pasco WA Resume Robert VeklotzRobertVeklotzNo ratings yet
- Hydraulic Vehicle Lift ST List of Parts and Appendices Stertil B.V BDocument24 pagesHydraulic Vehicle Lift ST List of Parts and Appendices Stertil B.V BOvidiu PopaNo ratings yet
- CBSE Class 12 Political Science WorksheetDocument2 pagesCBSE Class 12 Political Science WorksheetKamal BhardwajNo ratings yet
- Et154 PDFDocument6 pagesEt154 PDFbytecNo ratings yet
- Work OverDocument3 pagesWork OverDaniil GhilescuNo ratings yet