You might also like
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Single Visit Vs Multiple Visit EndodonticsDocument47 pagesSingle Visit Vs Multiple Visit Endodonticspiece_of_mindzz1969No ratings yet
- Fixed-Removable Lingual ArchDocument2 pagesFixed-Removable Lingual ArchOrtho OrganizersNo ratings yet
- Wound ManagementDocument44 pagesWound ManagementOby RomdhoniNo ratings yet
- Local and Regional Flaps in Head and Neck PRT 1 (NXPowerLite) / Orthodontic Courses by Indian Dental AcademyDocument93 pagesLocal and Regional Flaps in Head and Neck PRT 1 (NXPowerLite) / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- Uml Patient Information SystemDocument5 pagesUml Patient Information SystemSathyaPriya Ramasamy0% (1)
- Chapter 4Document3 pagesChapter 4YZEL ALFECHENo ratings yet
- Soap Note Rubric NS5067P April 2018: Teaching and Learning 6, 516-526Document1 pageSoap Note Rubric NS5067P April 2018: Teaching and Learning 6, 516-526coldNo ratings yet
- Diuretics Pharmacology 79 88Document6 pagesDiuretics Pharmacology 79 88Neha RoyNo ratings yet
- Nephrotic Syndrome in Adults: Acute Medicine 2018 17 (1) : 36-43 36Document8 pagesNephrotic Syndrome in Adults: Acute Medicine 2018 17 (1) : 36-43 36Deddy TriwijayaNo ratings yet
- Anti-Asthmatic Potential of Dried Draco SpilopterusDocument6 pagesAnti-Asthmatic Potential of Dried Draco SpilopterusNxxxNo ratings yet
- Part A.2 and AnsDocument3 pagesPart A.2 and AnsluigiNo ratings yet
- Anticholinergic Medication Use Is Associated With Globus Pharyngeus (HAFT 2016)Document5 pagesAnticholinergic Medication Use Is Associated With Globus Pharyngeus (HAFT 2016)DANDYNo ratings yet
- Task-Specific TrainingDocument16 pagesTask-Specific Trainingapi-293223028No ratings yet
- Hemodialysis English Lesson: Assignment From The Teacher Mr. Christovel Kahuweka S.PDDocument51 pagesHemodialysis English Lesson: Assignment From The Teacher Mr. Christovel Kahuweka S.PDJovelia KojongianNo ratings yet
- Person-Centered Theory by Carl Rogers: Prepared By: Rachel Joyce Peleno David Neriel OlanoDocument23 pagesPerson-Centered Theory by Carl Rogers: Prepared By: Rachel Joyce Peleno David Neriel OlanoNomer AerichNo ratings yet
- Disaster Nursing Cfu 084740Document9 pagesDisaster Nursing Cfu 084740Leone HeathensNo ratings yet
- The Vodka Diet Edit 12.20Document114 pagesThe Vodka Diet Edit 12.20Late Knight GamingNo ratings yet
- Iron Deficiency Anemia Fact SheetDocument2 pagesIron Deficiency Anemia Fact SheetCandace MorinNo ratings yet
- Hygiene 2Document41 pagesHygiene 2Nermine ElcokanyNo ratings yet
- Zimmer® Unicompartmental High Flex KneeDocument62 pagesZimmer® Unicompartmental High Flex Knee洪侊增No ratings yet
- Diagnosis of ScoliosisDocument17 pagesDiagnosis of ScoliosisMerci PirjolNo ratings yet
- Wicksall: ExperienceDocument2 pagesWicksall: Experienceapi-451678594No ratings yet
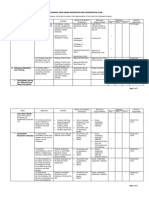
- For Companies - Sample - Three - Year Plan Matrix Revised 11.30.19Document5 pagesFor Companies - Sample - Three - Year Plan Matrix Revised 11.30.19Arnold RadaNo ratings yet
- Treating The Mother of Black Triangles With Bioclear VeneersDocument4 pagesTreating The Mother of Black Triangles With Bioclear VeneersThe Bioclear ClinicNo ratings yet
- Five To 10-Year Followup of Open Partial Nephrectomy in A Solitary KidneyDocument5 pagesFive To 10-Year Followup of Open Partial Nephrectomy in A Solitary KidneyMihaela LitovcencoNo ratings yet
- Management of Deep UlcerationDocument8 pagesManagement of Deep UlcerationQueenie WongNo ratings yet
- Cast Metal RestorationDocument48 pagesCast Metal RestorationRosa Faraon EspeñaNo ratings yet
- Kroll CV 26 March 2018Document92 pagesKroll CV 26 March 2018wolf woodNo ratings yet
- Building Self-Compassion - 03 - Preparing For Self-CompassionDocument9 pagesBuilding Self-Compassion - 03 - Preparing For Self-CompassionThe Happy Mind HouseNo ratings yet
- Brushing Technique: Development of ToothbrushesDocument70 pagesBrushing Technique: Development of Toothbrushesgauravparakh100% (2)