You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Future of FinanceDocument30 pagesThe Future of FinanceRenuka SharmaNo ratings yet
- JMC MSDS Puraspec 1173 (GB)Document10 pagesJMC MSDS Puraspec 1173 (GB)Benny Samsul B.No ratings yet
- Zero Tolerance 2010Document16 pagesZero Tolerance 2010Adrian KozelNo ratings yet
- Measuring Road Roughness by Static Level Method: Standard Test Method ForDocument6 pagesMeasuring Road Roughness by Static Level Method: Standard Test Method ForDannyChaconNo ratings yet
- Norman, K. R., Pali Philology & The Study of BuddhismDocument13 pagesNorman, K. R., Pali Philology & The Study of BuddhismkhrinizNo ratings yet
- Optical Transport Network SwitchingDocument16 pagesOptical Transport Network SwitchingNdambuki DicksonNo ratings yet
- Driver Drowsiness Detection System Using Raspberry PiDocument7 pagesDriver Drowsiness Detection System Using Raspberry PiIJRASETPublicationsNo ratings yet
- Kandungan Nutrisi JaheDocument10 pagesKandungan Nutrisi JaheCitra Indah FitriwatiNo ratings yet
- Family Presence During CPR and Invasive Procedures: Subscription InformationDocument2 pagesFamily Presence During CPR and Invasive Procedures: Subscription InformationCitra Indah FitriwatiNo ratings yet
- Multiple MyelomaDocument11 pagesMultiple MyelomaCitra Indah FitriwatiNo ratings yet
- Am J Crit Care-2006-Gélinas-420-7Document9 pagesAm J Crit Care-2006-Gélinas-420-7Citra Indah FitriwatiNo ratings yet
- Foot Pain CareDocument9 pagesFoot Pain CareCitra Indah FitriwatiNo ratings yet
- A Project On "Automatic Water Sprinkler Based On Wet and Dry Conditions"Document28 pagesA Project On "Automatic Water Sprinkler Based On Wet and Dry Conditions"Srínívas SrínuNo ratings yet
- Aharonov-Bohm Effect WebDocument5 pagesAharonov-Bohm Effect Webatactoulis1308No ratings yet
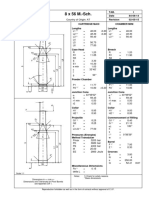
- 8 X 56 M.-SCH.: Country of Origin: ATDocument1 page8 X 56 M.-SCH.: Country of Origin: ATMohammed SirelkhatimNo ratings yet
- Ubicomp PracticalDocument27 pagesUbicomp Practicalvikrant sharmaNo ratings yet
- CHN Nutri LabDocument4 pagesCHN Nutri LabMushy_ayaNo ratings yet
- 16 - Ocean Currents & Salinity Interactive NotebookDocument23 pages16 - Ocean Currents & Salinity Interactive NotebookRaven BraymanNo ratings yet
- Acceptable Use Policy 08 19 13 Tia HadleyDocument2 pagesAcceptable Use Policy 08 19 13 Tia Hadleyapi-238178689No ratings yet
- Chapter 4: Thermal ComfortDocument16 pagesChapter 4: Thermal ComfortWengelNo ratings yet
- Assessing Apical PulseDocument5 pagesAssessing Apical PulseMatthew Ryan100% (1)
- Glossary of Blasting TermsDocument13 pagesGlossary of Blasting TermsNitesh JainNo ratings yet
- Assignment November11 KylaAccountingDocument2 pagesAssignment November11 KylaAccountingADRIANO, Glecy C.No ratings yet
- MSCM Dormitory Housing WEB UpdateDocument12 pagesMSCM Dormitory Housing WEB Updatemax05XIIINo ratings yet
- Fuentes v. Office of The Ombudsman - MindanaoDocument6 pagesFuentes v. Office of The Ombudsman - MindanaoJ. JimenezNo ratings yet
- BarricadeDocument6 pagesBarricadeJithu PappachanNo ratings yet
- FINAL VERSION On Assessment Tool For CDCs LCs Sept. 23 2015Document45 pagesFINAL VERSION On Assessment Tool For CDCs LCs Sept. 23 2015Edmar Cielo SarmientoNo ratings yet
- Legrand Price List-01 ST April-2014Document144 pagesLegrand Price List-01 ST April-2014Umesh SutharNo ratings yet
- NCP - Impaired Urinary EliminationDocument3 pagesNCP - Impaired Urinary EliminationFretzgine Lou ManuelNo ratings yet
- BSRM Ultima BrochureDocument2 pagesBSRM Ultima BrochuresaifuzzamanNo ratings yet
- 6int 2008 Dec ADocument6 pages6int 2008 Dec ACharles_Leong_3417No ratings yet
- Art Integrated ProjectDocument14 pagesArt Integrated ProjectSreeti GangulyNo ratings yet
- Catalogo PukangDocument41 pagesCatalogo PukangClarita Muller LeigueNo ratings yet
- Agrinome For Breeding - Glossary List For Mutual Understandings v0.3 - 040319Document7 pagesAgrinome For Breeding - Glossary List For Mutual Understandings v0.3 - 040319mustakim mohamadNo ratings yet
- Experiment 2 HORSEPOWER EFFICIENCY GEAR RATIO AND SPEED RATIODocument10 pagesExperiment 2 HORSEPOWER EFFICIENCY GEAR RATIO AND SPEED RATIOJake Polo SantiagoNo ratings yet