You might also like
- Translational Research in Coronary Artery Disease: Pathophysiology to TreatmentFrom EverandTranslational Research in Coronary Artery Disease: Pathophysiology to TreatmentNo ratings yet
- ClonidineDocument4 pagesClonidineDR RAVI ANANDNo ratings yet
- ESCAPE Study - JAMA 2005Document9 pagesESCAPE Study - JAMA 2005MICHAEL AMARILLO CORREANo ratings yet
- Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization EffectivenessDocument9 pagesEvaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization EffectivenessMelisa AnaNo ratings yet
- Continuous Hemodynamic MonitoringDocument54 pagesContinuous Hemodynamic MonitoringOrion JohnNo ratings yet
- Fifteen-Year Experience: Open Heart Surgery in Patients With End-Stage Renal FailureDocument6 pagesFifteen-Year Experience: Open Heart Surgery in Patients With End-Stage Renal FailureDavid RamirezNo ratings yet
- Pathophysiology of COPDDocument4 pagesPathophysiology of COPDrinieeeNo ratings yet
- Critical Care of Patients With Acute Ischemic and Hemorrhagic StrokeDocument7 pagesCritical Care of Patients With Acute Ischemic and Hemorrhagic StrokeMary Jhane VillanuevaNo ratings yet
- Decompressive Hemicraniectomy and DuroplastyDocument5 pagesDecompressive Hemicraniectomy and DuroplastyAmy NilifdaNo ratings yet
- Early Prediction of Severity StrokeDocument11 pagesEarly Prediction of Severity StrokeainihanifiahNo ratings yet
- Emboli ParuDocument10 pagesEmboli Paruindry_purnamasariNo ratings yet
- 2011 ATHM FootreflexologyDocument8 pages2011 ATHM FootreflexologyGorengan 27No ratings yet
- (19330693 - Journal of Neurosurgery) Decompressive Hemicraniectomy - Predictors of Functional Outcome in Patients With Ischemic StrokeDocument7 pages(19330693 - Journal of Neurosurgery) Decompressive Hemicraniectomy - Predictors of Functional Outcome in Patients With Ischemic StrokeRandy Reina RiveroNo ratings yet
- Randomised Controlled Trial of Continuous Positive Airway Pressure and Standard Oxygen Therapy in Acute Pulmonary OedemaDocument8 pagesRandomised Controlled Trial of Continuous Positive Airway Pressure and Standard Oxygen Therapy in Acute Pulmonary OedemaAlex PiecesNo ratings yet
- Stroke PreventionDocument8 pagesStroke PreventionjaanhoneyNo ratings yet
- Full Text 01Document8 pagesFull Text 01febyNo ratings yet
- Epidemiology of Hypertension and Metabolic Disorders: 10.1016/j.ijcard.2011.08.581Document2 pagesEpidemiology of Hypertension and Metabolic Disorders: 10.1016/j.ijcard.2011.08.581Mirza RisqaNo ratings yet
- Nimodipine in Aneurysmal Subarachnoid Hemorrhage: A Randomized Study of Intravenous or Peroral AdministrationDocument5 pagesNimodipine in Aneurysmal Subarachnoid Hemorrhage: A Randomized Study of Intravenous or Peroral AdministrationMiftakhul BaitiNo ratings yet
- 14 - Mazandarani2012Document7 pages14 - Mazandarani2012TandeanTommyNovenantoNo ratings yet
- Glyceryl Trinitrate For Acute Intracerebral HemorrhageDocument21 pagesGlyceryl Trinitrate For Acute Intracerebral HemorrhageAhmad Al-atthosNo ratings yet
- Cerebral Hemodynamic Effects of Morphine and Fentanyl in Patients With Severe Head InjuryDocument9 pagesCerebral Hemodynamic Effects of Morphine and Fentanyl in Patients With Severe Head InjuryVincent ScorsinniNo ratings yet
- Pulmonary Hypertension in Hemodialysis PatientsDocument5 pagesPulmonary Hypertension in Hemodialysis PatientsDr. Jatin GargNo ratings yet
- SaosDocument9 pagesSaosAlexander MayNo ratings yet
- E2f7 PDFDocument7 pagesE2f7 PDFSujith KumarNo ratings yet
- 10 1 1 524 3424Document10 pages10 1 1 524 3424Kim MariusNo ratings yet
- Nejmoa 010746Document9 pagesNejmoa 010746Mmle BlaséNo ratings yet
- Goyal Et Al-2015-Annals of NeurologyDocument7 pagesGoyal Et Al-2015-Annals of NeurologyWinda Wahyu IkaputriNo ratings yet
- Research Article: ECG Markers of Hemodynamic Improvement in Patients With Pulmonary HypertensionDocument11 pagesResearch Article: ECG Markers of Hemodynamic Improvement in Patients With Pulmonary HypertensionFaradilla NovaNo ratings yet
- Articles: BackgroundDocument9 pagesArticles: Backgroundapi-308365861No ratings yet
- Deccompresive Brain InjuryDocument4 pagesDeccompresive Brain InjuryDharmendra WidetyaNo ratings yet
- Research Article Baseline Serum Uric Acid Levels Are Associated With All-Cause Mortality in Acute Coronary Syndrome Patients After Percutaneous Coronary InterventionDocument9 pagesResearch Article Baseline Serum Uric Acid Levels Are Associated With All-Cause Mortality in Acute Coronary Syndrome Patients After Percutaneous Coronary InterventionmikeNo ratings yet
- Predictors of The Intracerebral Hemorrhage Volume in Hypertensive PatientsDocument5 pagesPredictors of The Intracerebral Hemorrhage Volume in Hypertensive PatientsNouchan NoupNo ratings yet
- Yeshwant 2018Document16 pagesYeshwant 2018StevenSteveIIINo ratings yet
- Brain Injury Resuscitation 2009Document8 pagesBrain Injury Resuscitation 2009Dandy Azmi AzwirNo ratings yet
- 67 Ej20-0159Document9 pages67 Ej20-0159desconocido 123 ambticonNo ratings yet
- Misra 2012Document7 pagesMisra 2012Carlos RiquelmeNo ratings yet
- Retired Firefighter of 40 Years Grateful For The Help of Doctors at HCA Florida MemorialDocument9 pagesRetired Firefighter of 40 Years Grateful For The Help of Doctors at HCA Florida MemorialSarah GlennNo ratings yet
- GLAUKOMA2Document12 pagesGLAUKOMA2NorytaWahyuniawatiAsfianaNo ratings yet
- CHARM Alt TrialDocument5 pagesCHARM Alt TrialCristian Villarroel SNo ratings yet
- Jakkula Et Al-2018-Intensive Care MedicineDocument11 pagesJakkula Et Al-2018-Intensive Care Medicinecaza_nova032282No ratings yet
- FluidDocument190 pagesFluidAndrias OzNo ratings yet
- Admission Inferior Vena Cava Measurements Are Associated With Mortality After Hospitalization For Acute Decompensated Heart FailureDocument18 pagesAdmission Inferior Vena Cava Measurements Are Associated With Mortality After Hospitalization For Acute Decompensated Heart FailurePuja Nastia LubisNo ratings yet
- 4 I PDFDocument6 pages4 I PDFDaniel Fernando Mendez CarbajalNo ratings yet
- Hyperglycemia and Neurological Outcome in Patients With Head InjuryDocument7 pagesHyperglycemia and Neurological Outcome in Patients With Head InjuryOsQ_drNo ratings yet
- Hemodynamic Support in Fluid-Refractory Pediatric Septic ShockDocument6 pagesHemodynamic Support in Fluid-Refractory Pediatric Septic ShockJosé Pepo Apey ReinosoNo ratings yet
- Bauch-Atrial Natriuretic Peptide As A MarDocument6 pagesBauch-Atrial Natriuretic Peptide As A MarSzendeNo ratings yet
- PrintDocument8 pagesPrintannarchyNo ratings yet
- IcuDocument56 pagesIcurulli_pranandaNo ratings yet
- Materials and MethodsDocument5 pagesMaterials and Methodsike ikeNo ratings yet
- A High Mean Arterial PressureDocument8 pagesA High Mean Arterial Pressureadek07No ratings yet
- Farmacology Del Paro CardiacoDocument14 pagesFarmacology Del Paro CardiacoNicoSwtifNo ratings yet
- Vasopressin and Methylprednisolone and HemodynamicDocument8 pagesVasopressin and Methylprednisolone and Hemodynamicaida154No ratings yet
- Brainhypoxiaisassociatedwithshort Termoutcomeafterseveretraumaticbraininjuryindependentlyofi 2Document9 pagesBrainhypoxiaisassociatedwithshort Termoutcomeafterseveretraumaticbraininjuryindependentlyofi 2indahNo ratings yet
- Pan 2017Document1 pagePan 2017Arhip CojocNo ratings yet
- Echocardiography in Hemodynamic MonitoringDocument5 pagesEchocardiography in Hemodynamic MonitoringDr.Biswajit jenaNo ratings yet
- Review Article: Elevated Blood Pressure in The Acute Phase of Stroke and The Role of Angiotensin Receptor BlockersDocument8 pagesReview Article: Elevated Blood Pressure in The Acute Phase of Stroke and The Role of Angiotensin Receptor BlockersPatrick RamosNo ratings yet
- Goal-Directed Fluid Restriction During Brain Surgery: A Prospective Randomized Controlled TrialDocument7 pagesGoal-Directed Fluid Restriction During Brain Surgery: A Prospective Randomized Controlled TrialkenjiNo ratings yet
- The Effects of Heart Failure On Renal FunctionDocument16 pagesThe Effects of Heart Failure On Renal FunctionNurul KamajayaNo ratings yet
- The Use of Sildenafil in Persistent Pulmonary Hypertension of The Newborn PDFDocument6 pagesThe Use of Sildenafil in Persistent Pulmonary Hypertension of The Newborn PDFmaciasdrNo ratings yet
- Deep Brain Stimulation: An Overview of History, Methods, and Future DevelopmentsDocument6 pagesDeep Brain Stimulation: An Overview of History, Methods, and Future DevelopmentsAik NoeraNo ratings yet
- Weight Loss Outcomes in Patients With Pain: ObesityDocument7 pagesWeight Loss Outcomes in Patients With Pain: ObesityAik NoeraNo ratings yet
- Neurotransmitter Dalam Fisiologi Saraf Otonom: Iwan Dwi Cahyono, Himawan Sasongko, Aria Dian PrimatikaDocument14 pagesNeurotransmitter Dalam Fisiologi Saraf Otonom: Iwan Dwi Cahyono, Himawan Sasongko, Aria Dian PrimatikaardianNo ratings yet
- Anatomical Variations of A CommDocument4 pagesAnatomical Variations of A CommAik NoeraNo ratings yet
- Neurophysiology of Deep Brain StimulationDocument33 pagesNeurophysiology of Deep Brain StimulationAik NoeraNo ratings yet
- Cerebrovascular Complications of COVID-19: Brief ReportDocument5 pagesCerebrovascular Complications of COVID-19: Brief ReportAmandaNo ratings yet
- The Holistic Approach In: 2 AnnouncementDocument1 pageThe Holistic Approach In: 2 AnnouncementAik NoeraNo ratings yet
- The Impact of Age On CognitionDocument11 pagesThe Impact of Age On CognitionDara Agusti MaulidyaNo ratings yet
- Pathophysiology of Dystonia: G. Madeo and A. PisaniDocument22 pagesPathophysiology of Dystonia: G. Madeo and A. PisaniAik NoeraNo ratings yet
- Middle Meningeal Artery Embolization To Treat Progressive Epidural Hematoma: A Case ReportDocument6 pagesMiddle Meningeal Artery Embolization To Treat Progressive Epidural Hematoma: A Case ReportAik NoeraNo ratings yet
- Jcen 22 2 78Document7 pagesJcen 22 2 78Aik NoeraNo ratings yet
- LO Radiologic Pattern of BronchopneumoniaDocument1 pageLO Radiologic Pattern of BronchopneumoniaAik NoeraNo ratings yet
- LARIO Score For LVO - 2019Document5 pagesLARIO Score For LVO - 2019Aik NoeraNo ratings yet
- The Role of Acetaminophen and Geohelminth Infection On The Incidence of Wheeze and EczemaDocument6 pagesThe Role of Acetaminophen and Geohelminth Infection On The Incidence of Wheeze and EczemaAik NoeraNo ratings yet
- Intracranial HaemorrhageDocument12 pagesIntracranial HaemorrhageAik NoeraNo ratings yet
- Pohl 2016Document9 pagesPohl 2016Aik NoeraNo ratings yet
- Acute Disseminated Encephalomyelitis in 228 Patients: A Retrospective, Multicenter US StudyDocument10 pagesAcute Disseminated Encephalomyelitis in 228 Patients: A Retrospective, Multicenter US StudyAik NoeraNo ratings yet
- Documents StackDocument1 pageDocuments StackDan MNo ratings yet
- 100 Questions in Cardiology-, PDFDocument241 pages100 Questions in Cardiology-, PDFditairinaNo ratings yet
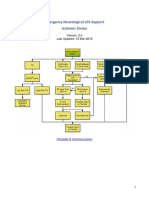
- Emergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Document22 pagesEmergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Aik NoeraNo ratings yet
- Predicting Outcome After Traumatic Brain InjuryDocument11 pagesPredicting Outcome After Traumatic Brain InjuryAik NoeraNo ratings yet
- LINAC Radiosurgery and Radiotherapy Treatment of Acoustic NeuromasDocument21 pagesLINAC Radiosurgery and Radiotherapy Treatment of Acoustic NeuromasAik NoeraNo ratings yet
- Journal Cerebellar AstrocytomaDocument18 pagesJournal Cerebellar AstrocytomaAik NoeraNo ratings yet
- Case Report Rabies BARUDocument14 pagesCase Report Rabies BARUAik NoeraNo ratings yet
- Falciparum: Misdiagnosis of An Imported Case of Malaria Caused by PlasmodiumDocument3 pagesFalciparum: Misdiagnosis of An Imported Case of Malaria Caused by PlasmodiumAik NoeraNo ratings yet
- Toxic FurDocument8 pagesToxic FurOur Compass100% (2)
- Fur - An Environmental Nightmare: Water & Air PollutionDocument3 pagesFur - An Environmental Nightmare: Water & Air PollutionAik NoeraNo ratings yet
- Acute Myelogenous LeukemiaDocument8 pagesAcute Myelogenous LeukemiaAik NoeraNo ratings yet
- Schedule SympoDocument6 pagesSchedule SympoAik NoeraNo ratings yet
- Pharma For StudentsDocument23 pagesPharma For StudentsWreddit RegalNo ratings yet
- Early Considerations of Mental IllnessDocument14 pagesEarly Considerations of Mental Illnesszuh blackNo ratings yet
- Management Unit Standard ListDocument1 pageManagement Unit Standard ListChristian MakandeNo ratings yet
- Bone Marrow AspirationDocument12 pagesBone Marrow Aspirationfeva55No ratings yet
- Delivering and InsertionDocument28 pagesDelivering and Insertionomaryaya18No ratings yet
- FWCQ22 COVID19 Healthcare Protocol V28 EnglishDocument24 pagesFWCQ22 COVID19 Healthcare Protocol V28 EnglishKarthik KothandaramanNo ratings yet
- Assam Hill Goat Production ND PerformanceDocument5 pagesAssam Hill Goat Production ND PerformanceShazzad Ul IslamNo ratings yet
- Support de Cours ANG504-Anglais Médical PDFDocument34 pagesSupport de Cours ANG504-Anglais Médical PDFN'sougan Fidel WOUDJINo ratings yet
- II. Upper Respiratory Tract DisordersDocument98 pagesII. Upper Respiratory Tract DisordersarielleortuosteNo ratings yet
- HemorrhageDocument239 pagesHemorrhageparmeshori100% (1)
- ST Rose of Lima Catholic SchoolDocument30 pagesST Rose of Lima Catholic SchoolKathy SarmientoNo ratings yet
- Laporan Harian Diagnosa 21022022-012015Document20 pagesLaporan Harian Diagnosa 21022022-012015puskesmas sukanegaraNo ratings yet
- Wang Et Al-2012-Journal of Pineal ResearchDocument8 pagesWang Et Al-2012-Journal of Pineal ResearchDionisio MesyeNo ratings yet
- My Method - E. CoueDocument236 pagesMy Method - E. Couealex100% (4)
- Internal Medicine 1, Conrad FischerDocument35 pagesInternal Medicine 1, Conrad Fischerdukelist566100% (3)
- 345-Article Text-1032-1-10-20180629Document4 pages345-Article Text-1032-1-10-20180629Regina AyediaNo ratings yet
- Physiology Biochemistry Gen Surgery AnswersDocument7 pagesPhysiology Biochemistry Gen Surgery AnswersSanNo ratings yet
- Acutepainmanagement: Nabil Moussa,, Orrett E. OgleDocument13 pagesAcutepainmanagement: Nabil Moussa,, Orrett E. OgleMahmoud AbouelsoudNo ratings yet
- Adenomiosis CX ConservadoraDocument12 pagesAdenomiosis CX Conservadorajuan carlos pradaNo ratings yet
- Abnormal Perception PDFDocument5 pagesAbnormal Perception PDFsugarmelodies100% (1)
- Definition:: Pleural EffusionDocument4 pagesDefinition:: Pleural EffusionGetom NgukirNo ratings yet
- The Kissing PaperDocument33 pagesThe Kissing PapersamuelacohenNo ratings yet
- EpidemiologyDocument52 pagesEpidemiologyasdfsNo ratings yet
- Obstetrics V13 Obstetric Emergencies Chapter 1614623048Document12 pagesObstetrics V13 Obstetric Emergencies Chapter 1614623048Jeferson CuaranNo ratings yet
- Swollen Ankles and FeetDocument36 pagesSwollen Ankles and FeetMagikeyNo ratings yet
- Eng PDFDocument98 pagesEng PDFMark Anthony MadridanoNo ratings yet
- History of MicrobiologyDocument23 pagesHistory of MicrobiologyISRAELNo ratings yet
- Biological Assay in Quality ControlDocument34 pagesBiological Assay in Quality ControlDilawar KhanNo ratings yet
- 9814774723Document467 pages9814774723Ortopedia FabioNo ratings yet
- Medical Medium Thyroid Healing The TruthDocument8 pagesMedical Medium Thyroid Healing The TruthVatsala Saith0% (18)