Importance of ST-Segment Depression during Dipyridamole
201
Tl Myocardial Perfusion Imaging in the Diagnosis of
Multivessel Coronary Artery Disease
Yu-Erh Huang, Chiang-Hsuan Lee, Pei-Wen Wang, Hsu-Hua Huang
Department of Nuclear Medicine, Chang Gung Memorial Hospital, Kaohsiung, Taiwan
Received 9/2/2004; revised 12/14/2004; accepted 12/16/2004.
For correspondence or reprints contact: Chiang-Hsuan Lee, M.D., Department of
Nuclear Medicine, Chang Gung Memorial Hospital, 123 Ta-Pei-Road, Niao-Sung,
Kaohsiung 833, Taiwan, ROC. Tel: (886)7-7317123 ext. 2627, Fax: (886)7-
7317123 ext. 2631, E-mail: lee4cgmh@mail.ht.net.tw
We describe a case of a 72-year-old female who under-
went dipyridamole
201
Tl myocardial perfusion imaging
for the evaluation of coronary artery disease (CAD).
The images showed no transient or fixed defect, but
ST-segment depression on electrocardiography was
noted after dipyridamole administration. Coronary
angiography demonstrated multiple significant stenosis
i n the l eft mai n, l eft ci rcumfl ex, and l eft anteri or
descending coronary arteries. Thus, dipyridamole-
induced ST-segment depression (DISTD) helped to
identify the multivessel CAD. In this article, we empha-
size that normal dipyridamole
201
Tl myocardial perfusion
images with DISTD still suggests the presence of CAD.
Key words: dipyridamole,
201
Tl myocardial perfusion
scintigraphy, ST-segment depression
Ann Nucl Med Sci 2005;18:51-56
Radionuclide myocardial perfusion scintigraphy is clin-
ically useful for the diagnosis of coronary artery disease
(CAD). It depends upon a physiologic stimulus, such as exer-
cise, or pharmacologic agents to provoke coronary hyper-
emia. For patients who are unable to exercise fully for non-
cardiac reasons, a standard exercise stress test leads to
impaired sensitivity [1-3]. Pharmacologic stress testing using
intravenous infusion of dipyridamole or adenosine appears to
be an excellent alternative in these patients and has essential-
ly the same accuracy in detecting CAD when compared with
exercise [4-6].
Ischemic ST-segment depression on electrocardiogra-
phy (ECG) occurs in 6% to 34% of patients receiving intra-
venous dipyridamole [7]. Although it is not very sensitive,
ST-segment depression that occurs during dipyridamole
administration is quite specific for the presence of CAD [8].
It is likely that dipyridamole-induced ST-segment depression
(DISTD) is more likely to occur in patients with angiographic
evidence of CAD compared to those patients without CAD
[9,10].
In the previous reports, there were limited data referring
to the clinical significance of normal dipyridamole
201
Tl
myocardial perfusion images with ST-segment depression
during the test [8,11,12]. We describe a patient whose dipyri-
damole
201
Tl myocardial perfusion images did not show any
transient or fixed defect. However, ST-segment depression
was noted after dipyridamole infusion. Coronary angiography
showed left main and two-vessel CAD.
Case Report
A 72-year-old female with hypertension for 10 years
presented with dyspnea and chest tightness. Physical exami-
nations showed a grade III/VI diastolic heart murmur.
Laboratory data revealed elevated cholesterol at the level of
285 mg % (normal range <200 mg %), elevated LDL at the
level of 139 mg/dL (normal range <130 mg/dL) and low
HDL level (28 mg/dL, normal range >40 mg/dL). Resting
Huang YE et al
ECG showed left ventricular hypertrophy (Figure 1). Chest
X-ray revealed cardiomegaly with pulmonary congestion.
She was referred for
201
Tl myocardial perfusion scintigraphy
under the impression of CAD.
The patient had fasted for 4 h and did not have any
xanthine medications or caffeine containing beverages.
Resting heart rate and blood pressure were 75 bpm and
181/79 mmHg, respectively. Dipyridamole was administra-
ted intravenously at a dose of 0.56 mg/kg over 4 min. Three
millicuries of
201
Tl was given 7 min from start of the dipyri-
damole infusion. ECG at 9 min showed 1 mm horizontal ST-
segment depression in the leads II, III, and aVF (Figure 2).
The patient did not complain of chest discomfort. Her heart
rate and blood pressure at that time were 84 bpm and 161/69
mmHg, respectively. ST-segment depression returned to
baseline after intravenous administration of 180 mg of
aminophylline at 11 min. Single photon emission computed
tomography (SPECT) imaging began at 12 min with a three-
headed scintillation camera (Siemens, MULTISPECT), and
the resting study was performed 4 h later.
201
Tl myocardial perfusion SPECT revealed no perfu-
sion defect (Figure 3). No increased lung
201
Tl uptake or tran-
sient left ventricular dilatation was noted. The transthoracic
echocardiogram was then performed and showed normal left
ventricular systolic function and wall motion.
Although the myocardial perfusion SPECT and
echocardiogram were normal, we could not
exclude the possibility of CAD due to the find-
ing of DISTD, and the patient was referred for
cardiac catheterization. The coronary angiogra-
phy showed 81% stenosis in the distal left main
coronary artery (LM) involving the ostium of
left circumflex coronary artery (LCX) (Figure
4A). The ostium of left anterior descending
coronary artery (LAD) had 61% stenosis (Figure
4B). The proximal right coronary artery had
mild lesion. The patient received angioplasty to
distal LM to the ostium of LCX, and the ostium
of LAD.
Discussion
Thallium-201 myocardial scintigraphy
measures myocardial flow relatively, rather than
absolutely. Hence when patients have triple-ves-
sel CAD, the myocardial segments supplied by
the less severely stenosed arteries may appear to
be normal. Previous reports have estimated that
only 13%-50% of patients with triple-vessel or
left main CAD had perfusion abnormalities in
multiple territories [13-15]. Besides, patients
with multi-vessel CAD may not have stress-
induced perfusion abnormalities because of the
balanced global hypoperfusion of the left ventri-
cle [16]. Our patient did not have any transient
Ann Nucl Med Sci 2005;18:51-56 Vol. 18 No. 1 March 2005
52
Figure 2. Electrocardiogram at 9 min after the dipyridamole infusion shows
a horizontal ST-segment depression for 1mm in the leads II, III, and aVF.
Figure 1. Resting electrocardiogram shows a sinus rhythm and left ventric-
ular hypertrophy.
Dipyridamole
201
Tl(]([(ST||
ST-segment depression during dipyridamole
201
Tl myocardial perfusion imaging
or fixed perfusion abnormalities in myocardial perfusion
SPECT. However, Subsequent coronary angiography showed
significant stenosis in the left main and two coronary arte-
ries. This result correlates with the previous reports. The
absence of myocardial perfusion defects may represent
balanced ischemia in our case.
Several studies have estimated the clinical significance
of DISTD during
201
Tl myocardial imaging. Villanueva et al.
[12] observed that DISTD occurred in 15% (28/182) of the
patients receiving
201
Tl studies. They also found that
201
Tl
redistribution and
201
Tl images of a multi-vessel pattern were
more frequently seen in patients with ST-segment depression
than those without. In the study of Chambers et al. [11], 41
patients with angiographic evidence of CAD were collected
among 127 dipyridamole
201
Tl studies. DISTD occurred in
34% (14/41) of these patients. Larrman et al. [8] performed
201
Tl scintigraphy after dipyridamole infusion with low-level
exercise in 98 subjects. DISTD was observed in 30/98
(31%), and particularly, 28/30 (93%) had significant CAD.
In our case, although no reversible defect was observed, the
finding of DISTD suggested the presence of CAD.
Normal dipyridamole
201
Tl myocardial perfusion
images with DISTD have been noted in the previous reports.
In the study of Laarman et al. [8], there were four patients
with ST depression and normal
201
Tl images, and all of them
(4/4) had CAD. In the report of Chamber et al. [11], there
was one patient who had normal
201
Tl images with DISTD in
all 41 patients with angiographically documented CAD.
Marshall et al. [17] used another pharmacologic agent,
adenosine, to perform myocardial perfusion imaging. There
were 13 patients classified as normal
201
Tl scans with DISTD,
and 4/13 (31%) had a subsequent cardiac event at the follo-
wing 1 to 3 years period. Our reporting case demonstrates a
similar result. DISTD helped us to identify the significant
left main and multi-vessel CAD in this patient whose
201
Tl
images were normal.
Factors that influence frequency and location of stress-
induced ST depression in the ECG is incompletely under-
stood [18]. Previous reports have demonstrated the inability
of ECG lead location of ST depression
during exercise to localize areas of
ischemic myocardium [18-23]. Tavel et
al. [18] showed that the number of areas
that demonstrated ST depression was
related to severity of ischemia, but the
distribution of ST depression did not
correlate with location of ischemia. In
our patient, DISTD was found in the
inferior leads (II, III, aVF). Although it
was not the site showing the most
severe narrowing in angiography,
according to the previous reports, sig-
nificant ST depression in multiple leads
indicated the presence of CAD.
2005;18:51-56 20053) 181)
53
Figure 3.
201
Tl myocardial perfusion SPECT reveals no tran-
sient or fixed defect.
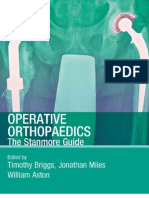
Figure 4. (A) Coronary angiogram shows 81% stenosis in the distal left main coro-
nary artery involving the ostium of the left circumflex coronary artery. (B) Coronary
angiogram shows that the ostium of the left anterior descending coronary artery has
61% stenosis.
A B
Huang YE et al
In our reporting case, if we had used the perfusion
imaging alone, the extensive coronary disease could have
been missed. Therefore, we emphasize the importance of
accessing ST-segment depression during performing dipyri-
damole myocardial perfusion imaging. If normal dipyri-
damole
201
Tl myocardial perfusion images combine with
DISTD, it still implies the presence of CAD.
References
1. Heller GV, Ahmed I, Tilkemeier PL, Barbour MM,
Garber CE. Influence of exercise intensity on the pre-
sence, distribution, and size of thallium-201 defects. Am
Heart J 1992;123:909-916.
2. Iskandrian AS, Heo J, Kong B, Lyons E. Effect of exer-
cise level on the ability of thallium-201 tomographic
imaging in detecting coronary artery disease: analysis of
461 patients. J Am Coll Cardiol 1989;14:1477-1486.
3. Esquivel L, Pollock SG, Beller GA, Gibson RS, Watson
DD, Kaul S. Effect of the degree of effort on the sensitiv-
ity of the exercise thallium-201 stress test in sympto-
matic coronary artery disease. Am J Cardiol
1989;63:160-165.
4. Varma SK, Watson DD, Beller GA. Quantitative compa-
rison of thallium-201 scintigraphy after exercise and
dipyridamole in coronary artery disease. Am J Cardiol
1989;64:871-877.
5. Gimple LW, Hutter AM Jr, Guiney TE, Boucher CA.
Prognostic utility of predischarge dipyridamole-thallium
imaging compared to predischarge submaximal exercise
electrocardiography and maximal exercise thallium
imaging after uncomplicated acute myocardial infarction.
Am J Cardiol 1989;64:1243-1248.
6. Coyne EP, Belvedere DA, Vande Streek PR, Weiland FL,
Evans RB, Spaccavento LJ. Thallium-201 scintigraphy
after intravenous infusion of adenosine compared with
exercise thallium testing in the diagnosis of coronary
artery disease. J Am Coll Cardiol 1991;17:1289-1294.
7. Verani MS. Pharmacologic stress testing and other alter-
native techniques in the diagnosis of coronary artery dis-
ease. In: Iskandrian AE, Verani MS, ed. Nuclear Cardiac
Imaging Principles and Applications. 3rd ed. New York:
Oxford University Press, Inc.; 2003:170.
8. Laarman GJ, Serruys PW, Verzijlbergen JF, Ascoop CA.
Thallium-201 scintigraphy after dipyridamole infusion
with low-level exercise. III. Clinical significance and
additional diagnostic value of ST segment depression
and angina pectoris during the test. Eur Heart J
1990;11:705-711.
9. Pearlman JD, Boucher CA. Diagnostic value for coro-
nary artery disease of chest pain during dipyridamole-
thallium stress testing. Am J Cardiol 1988;61:43-45.
10. Leppo J, Boucher CA, Okada RD, Newell JB, Strauss
HW, Pohost GM. Serial thallium-201 myocardial imag-
ing after dipyridamole infusion: diagnostic utility in
detecting coronary stenoses and relationship to regional
wall motion. Circulation 1982;66:649-657.
11. Chambers CE, Brown KA. Dipyridamole-induced ST
segment depression during thallium-201 imaging in
patients with coronary artery disease: angiographic and
hemodynamic determinants. J Am Coll Cardiol
1988;12:37-41.
12. Villanueva FS, Smith WH, Watson DD, Beller GA. ST-
segment depression during dipyridamole infusion, and its
clinical, scintigraphic and hemodynamic correlates. Am J
Cardiol 1992;69:445-448.
13. Rehn T, Griffith LS, Achuff SC, et al. Exercise thallium-
201 myocardial imaging in left main coronary artery di-
sease: sensitive but not specific. Am J Cardiol
1981;48:217-223.
14. Christian TF, Miller TD, Bailey KR, Gibbons RJ.
Noninvasive identification of severe coronary artery di-
sease using exercise tomographic thallium-201 imaging.
Am J Cardiol 1992;70:14-20.
15. Chae SC, Heo J, Iskandrian AS, Wasserleben V, Cave V.
Identification of extensive coronary artery disease in
women by exercise single-photon emission computed
tomographic (SPECT) thallium imaging. J Am Coll
Cardiol 1993;21:1305-1311.
16. Yamagishi H, Shirai N, Yoshiyama M, et al. Incremental
value of left ventricular ejection fraction for detection of
multivessel coronary artery disease in exercise Tl-201
gated myocardial perfusion imaging. J Nucl Med
2002;43:131-139.
17. Marshall ES, Raichlen JS, Kim SM, et al. Prognostic sig-
Ann Nucl Med Sci 2005;18:51-56 Vol. 18 No. 1 March 2005
54
Dipyridamole
201
Tl(]([(ST||
ST-segment depression during dipyridamole
201
Tl myocardial perfusion imaging
nificance of ST-segment depression during adenosine
perfusion imaging. Am Heart J 1995;130:58-66.
18. Tavel ME, Shaar C. Relation between the electrocardio-
graphic stress test and degree and location of myocardial
ischemia. Am J Cardiol 1999;84:119-124.
19. Mark DB, Hlatky MA, Lee KL, Harrell FE Jr, Califf
RM, Pryor DB. Localizing coronary artery obstructions
with the exercise treadmill test. Ann Intern Med
1987;106:53-55.
20. Fuchs RM, Achuff SC, Grunwald L, Yin FC, Griffith LS.
Electrocardiographic localization of coronary artery nar-
rowings: studies during myocardial ischemia and infarc-
tion in patients with one-vessel disease. Circulation
1982;66:1168-1176.
21. Dunn RF, Freedman B, Bailey IK, Uren RF, Kelly DT.
Localization of coronary artery disease with exercise
electrocardiography: correlation wit thallium-201
myocardial perfusion scanning. Am J Cardiol
1981;48:837-843.
22. Abouantoun S, Ahnve S, Savvides M, Witztum K,
Jensen D, Froelicher V. Can areas of myocardial
ischemia be localized by the exercise electrocardiogram?
A correlative study with thallium-201 scintigraphy. Am
Heart J 1984;108:933-941.
23. Kang X, Berman DS, Lewin HC, et al. Comparative
localization of myocardial ischemia by exercise electro-
cardiography and myocardial perfusion SPECT. J Nucl
Cardiol 2000;7:140-145.
2005;18:51-56 20053) 181)
55
Huang YE et al
Ann Nucl Med Sci 2005;18:51-56 Vol. 18 No. 1 March 2005
56
Dipyridamole-201{@@u{q)ST[|J#
q@jj]|]]]]
72 dipyridamole -201
dipyridamole ST
dipyridamole ST
dipyridamole -201 dipyridamole ST
dipyridamole -201 ST
2005;18:51-56
939)2j 9312)14, 9312)16]]]
j|fj] ,833)]#j123 ,)|jjj]j| (07)7317123]2627 [[(07)-7317123]2631 j/
lee4cgmh@mail.ht.net.tw
You might also like
- The Cleveland Clinic Cardiology Board ReviewDocument114 pagesThe Cleveland Clinic Cardiology Board ReviewSohil Elfar100% (1)
- The Ischemic ElectrocardiogramDocument16 pagesThe Ischemic ElectrocardiogramAdiel OjedaNo ratings yet
- Electrocardiography For Healthcare ProfessionalsDocument6 pagesElectrocardiography For Healthcare ProfessionalsOasisBogo Med0% (1)
- Braunwald: Chronic Coronary Artery DiseaseDocument122 pagesBraunwald: Chronic Coronary Artery Diseaseusfcards100% (1)
- Theischemic Electrocardiogram: Daniel L. KreiderDocument16 pagesTheischemic Electrocardiogram: Daniel L. KreiderAlejandro Peñaloza TapiaNo ratings yet
- The Ischemic Electrocardiogram: Daniel L. KreiderDocument12 pagesThe Ischemic Electrocardiogram: Daniel L. Kreidermarianagonzalezgil11No ratings yet
- Stress-Related Cardiomyopathy or Tako-Tsubo Syndrome: Current ConceptsDocument6 pagesStress-Related Cardiomyopathy or Tako-Tsubo Syndrome: Current ConceptslivroinglesNo ratings yet
- Lapkas VT RevisiDocument13 pagesLapkas VT RevisiRannyNo ratings yet
- Cardiogenic Shock Workup (Medscape)Document8 pagesCardiogenic Shock Workup (Medscape)Tia WasrilNo ratings yet
- European Heart Journal (2003) 24, 787-788Document2 pagesEuropean Heart Journal (2003) 24, 787-788api-26263700No ratings yet
- Myocardial Infarction, Acute Case FileDocument7 pagesMyocardial Infarction, Acute Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Hollamby Mitchell s5001226 Case 1 DtgaDocument13 pagesHollamby Mitchell s5001226 Case 1 Dtgaapi-299009880No ratings yet
- Bader Madoukh, Ayman Battisha, Henry Ukwu, Mohammed Al-Sadawi, Shakil ShaikhDocument4 pagesBader Madoukh, Ayman Battisha, Henry Ukwu, Mohammed Al-Sadawi, Shakil ShaikhputriayuratnasariNo ratings yet
- Heart Failure AbnetDocument119 pagesHeart Failure AbnetAbnet WondimuNo ratings yet
- ST-segment Depression: All Are Not Created Equal!Document6 pagesST-segment Depression: All Are Not Created Equal!asclepiuspdfsNo ratings yet
- 1 s2.0 S1878540912000473 MainDocument3 pages1 s2.0 S1878540912000473 MainIoana SusNo ratings yet
- Letter To The Editor: Clinical Case Nr. 2Document3 pagesLetter To The Editor: Clinical Case Nr. 2melisaberlianNo ratings yet
- Ajmcr 6 8 3Document4 pagesAjmcr 6 8 3Dewa Aix61No ratings yet
- Cardiac Resynchronisation Therapy For Patients With Heart FailureDocument5 pagesCardiac Resynchronisation Therapy For Patients With Heart FailureIpar DayNo ratings yet
- Cairns 1976Document14 pagesCairns 1976Direvald WesterosNo ratings yet
- Jurnal Blok 10Document3 pagesJurnal Blok 10Yunus Lumban RajaNo ratings yet
- Acute Coronary Syndrome Case FileDocument4 pagesAcute Coronary Syndrome Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Electrocardiograph Changes in Acute Ischemic Cerebral StrokeDocument6 pagesElectrocardiograph Changes in Acute Ischemic Cerebral StrokeFebniNo ratings yet
- Acute Myocarditis Mimicking ST-elevation Myocardial Infarction: A Diagnostic Challenge For Frontline CliniciansDocument3 pagesAcute Myocarditis Mimicking ST-elevation Myocardial Infarction: A Diagnostic Challenge For Frontline CliniciansZazaNo ratings yet
- Pseudonormalization: Clinical, Electrocardiographic, Echocardiographic, and Angiographic CharacteristicsDocument3 pagesPseudonormalization: Clinical, Electrocardiographic, Echocardiographic, and Angiographic CharacteristicspavithranmbbsNo ratings yet
- Alteraciones Ecocardiograficas en JovenesDocument5 pagesAlteraciones Ecocardiograficas en JovenesFelicia Rolón CárdenasNo ratings yet
- ArticuloDocument24 pagesArticuloGiovanni EscobarNo ratings yet
- Angina Pectoris in Patients With A History of Myocardial InfarctionDocument5 pagesAngina Pectoris in Patients With A History of Myocardial Infarctionger4ld1nNo ratings yet
- Increasingly Sensitive Assays For Cardiac TroponinsDocument8 pagesIncreasingly Sensitive Assays For Cardiac TroponinsAbel Espinoza MedallaNo ratings yet
- 2016-02 Imaging in ACS, FinalDocument27 pages2016-02 Imaging in ACS, FinalMakhyan JibrilNo ratings yet
- Spon Artery DissceDocument6 pagesSpon Artery DissceMuhammad JunaidNo ratings yet
- Falla Cardiaca ReviewDocument9 pagesFalla Cardiaca ReviewYasmin CarhuamacaNo ratings yet
- Corazon y SojenDocument7 pagesCorazon y Sojenmaria cristina aravenaNo ratings yet
- 10.1007@s00296 008 0601 0Document3 pages10.1007@s00296 008 0601 0Kuber RawaNo ratings yet
- Electrocardiographic Changes and Intracranial Pathology: Geraldine Syverud, Crna, BSNDocument4 pagesElectrocardiographic Changes and Intracranial Pathology: Geraldine Syverud, Crna, BSNchuck55No ratings yet
- Abdominal Aortic AneurysmDocument10 pagesAbdominal Aortic AneurysmPrince K. TaileyNo ratings yet
- CardioDocument146 pagesCardiobbdddNo ratings yet
- Cardio 1.5Document2 pagesCardio 1.5ChibuNo ratings yet
- In-Hospital Arrhythmia Development and Outcomes in Pediatric Patients With Acute MyocarditisDocument15 pagesIn-Hospital Arrhythmia Development and Outcomes in Pediatric Patients With Acute MyocarditisAnonymous OU6w8lX9No ratings yet
- Cric2018 7237454Document4 pagesCric2018 7237454Muhammad Nur Ardhi LahabuNo ratings yet
- Case Report Missed Connections: Identification of Atrial Septal Defect by MRIDocument4 pagesCase Report Missed Connections: Identification of Atrial Septal Defect by MRIMuhammad Nur Ardhi LahabuNo ratings yet
- Circulation 1973 ALONSO 588 96Document10 pagesCirculation 1973 ALONSO 588 96Jessica ARNo ratings yet
- 67-Article Text-115-1-10-20171026Document5 pages67-Article Text-115-1-10-20171026Maria MiripNo ratings yet
- Massive Pulmonary Embolism Presenting As Seizures: December 2008 Vol 10 No 4Document4 pagesMassive Pulmonary Embolism Presenting As Seizures: December 2008 Vol 10 No 4BelladonnaRoxNo ratings yet
- Review WellenDocument10 pagesReview WellenJihanirani LubisNo ratings yet
- Cardiogenic Shock - FINALDocument79 pagesCardiogenic Shock - FINALIgor StefanetNo ratings yet
- 1 s2.0 S0735675715005483 MainDocument3 pages1 s2.0 S0735675715005483 Mainfebriandika gawlNo ratings yet
- Nikhil Thesis AbstractDocument28 pagesNikhil Thesis AbstractNikhil KalasareNo ratings yet
- Article 1Document4 pagesArticle 1Fakhar Mahmood ShahidNo ratings yet
- Modified Sgarbossa CriteriaDocument13 pagesModified Sgarbossa CriteriaJenny de OzNo ratings yet
- Jurnal Kedokteran Dan Kesehatan IndonesiaDocument7 pagesJurnal Kedokteran Dan Kesehatan IndonesiaAlfix AnugrahNo ratings yet
- T 20 CardiologyDocument51 pagesT 20 Cardiologydrkhalid12100% (3)
- Rheumatic Heart Disease With Complication of Atrial FibrillationDocument3 pagesRheumatic Heart Disease With Complication of Atrial FibrillationsamudraandiNo ratings yet
- 45 1057Document5 pages45 1057Gabriela PinticanNo ratings yet
- Clinical Research: Heart Failure/cardiomyopathyDocument11 pagesClinical Research: Heart Failure/cardiomyopathyGustavo HenriqueNo ratings yet
- The Effect of Cilostazol On Right Heart FunctionDocument43 pagesThe Effect of Cilostazol On Right Heart FunctionGunawan YogaNo ratings yet
- Diagnostic Examinations in Acute Ischemic Heart DiseaseDocument6 pagesDiagnostic Examinations in Acute Ischemic Heart DiseasenoemilauNo ratings yet
- Role of Echocardiography in Acute Pulmonary EmbolismDocument15 pagesRole of Echocardiography in Acute Pulmonary Embolismpaola andrea bolivar collantesNo ratings yet
- Acute Myocardial Infarction en Estenosis Aortica Severa Con Coronarias NormalesDocument4 pagesAcute Myocardial Infarction en Estenosis Aortica Severa Con Coronarias NormalesfabiandionisioNo ratings yet
- De Novo Acute Heart Failure and Acutely Decompensated Chronic Heart Failure PDFDocument14 pagesDe Novo Acute Heart Failure and Acutely Decompensated Chronic Heart Failure PDFEffika PutriNo ratings yet
- Case-Based Device Therapy for Heart FailureFrom EverandCase-Based Device Therapy for Heart FailureUlrika Birgersdotter-GreenNo ratings yet
- Carbapenem-Resistant Acinetobacter Baumannii Infections After Organ TransplantationDocument7 pagesCarbapenem-Resistant Acinetobacter Baumannii Infections After Organ TransplantationsserggiosNo ratings yet
- Fulminant Endocarditis and Disseminated Infection Caused by Carbapenem Resistant Acinetobacter Baumannii in A Renal Pancreas Transplant RecipientDocument8 pagesFulminant Endocarditis and Disseminated Infection Caused by Carbapenem Resistant Acinetobacter Baumannii in A Renal Pancreas Transplant RecipientsserggiosNo ratings yet
- Carbapenem-Resistant Enterobacteriaceae in Special Populations Solid Organ TransplantDocument13 pagesCarbapenem-Resistant Enterobacteriaceae in Special Populations Solid Organ TransplantsserggiosNo ratings yet
- Evolution of Drug-Resistant Acinetobacter Baumannii After DCD Renal TransplantationDocument9 pagesEvolution of Drug-Resistant Acinetobacter Baumannii After DCD Renal TransplantationsserggiosNo ratings yet
- Evolution of Drug-Resistant Acinetobacter Baumannii After DCD Renal TransplantationDocument9 pagesEvolution of Drug-Resistant Acinetobacter Baumannii After DCD Renal TransplantationsserggiosNo ratings yet
- Carbapenem-Resistant Acinetobacter Baumannii Infections After Organ TransplantationDocument7 pagesCarbapenem-Resistant Acinetobacter Baumannii Infections After Organ TransplantationsserggiosNo ratings yet
- Fulminant Endocarditis and Disseminated Infection Caused by Carbapenem Resistant Acinetobacter Baumannii in A Renal Pancreas Transplant RecipientDocument8 pagesFulminant Endocarditis and Disseminated Infection Caused by Carbapenem Resistant Acinetobacter Baumannii in A Renal Pancreas Transplant RecipientsserggiosNo ratings yet
- Carbapenem-Resistant Enterobacteriaceae in Special Populations Solid Organ TransplantDocument13 pagesCarbapenem-Resistant Enterobacteriaceae in Special Populations Solid Organ TransplantsserggiosNo ratings yet
- High Mortality Rates Among Solid Organ Transplant Recipients Infected With Extensively Drug-Resistant Acinetobacter BaumanniiDocument7 pagesHigh Mortality Rates Among Solid Organ Transplant Recipients Infected With Extensively Drug-Resistant Acinetobacter BaumanniisserggiosNo ratings yet
- Epidemiology, Clinical Characteristics and Outcomes of Extensively Drug-Resistant Acinetobacter BaumanniiDocument10 pagesEpidemiology, Clinical Characteristics and Outcomes of Extensively Drug-Resistant Acinetobacter BaumanniisserggiosNo ratings yet
- High Mortality Rates Among Solid Organ Transplant Recipients Infected With Extensively Drug-Resistant Acinetobacter BaumanniiDocument7 pagesHigh Mortality Rates Among Solid Organ Transplant Recipients Infected With Extensively Drug-Resistant Acinetobacter BaumanniisserggiosNo ratings yet
- Epidemiology, Clinical Characteristics and Outcomes of Extensively Drug-Resistant Acinetobacter BaumanniiDocument10 pagesEpidemiology, Clinical Characteristics and Outcomes of Extensively Drug-Resistant Acinetobacter BaumanniisserggiosNo ratings yet
- Carbapenem-Resistant Acinetobacter Baumannii Infections After Organ TransplantationDocument7 pagesCarbapenem-Resistant Acinetobacter Baumannii Infections After Organ TransplantationsserggiosNo ratings yet
- Carbapenem-Resistant Enterobacteriaceae in Special Populations Solid Organ TransplantDocument13 pagesCarbapenem-Resistant Enterobacteriaceae in Special Populations Solid Organ TransplantsserggiosNo ratings yet
- Legionella Pneumophila PeritonitisDocument5 pagesLegionella Pneumophila PeritonitissserggiosNo ratings yet
- Journal of Advanced Research: Usama A.A. Sharaf El Din, Mona M. Salem, Dina O. AbdulazimDocument12 pagesJournal of Advanced Research: Usama A.A. Sharaf El Din, Mona M. Salem, Dina O. AbdulazimNorman RiyadiNo ratings yet
- Nocardia Infection in KidneyDocument20 pagesNocardia Infection in KidneysserggiosNo ratings yet
- Fulminant Endocarditis and Disseminated Infection Caused by Carbapenem Resistant Acinetobacter Baumannii in A Renal Pancreas Transplant RecipientDocument8 pagesFulminant Endocarditis and Disseminated Infection Caused by Carbapenem Resistant Acinetobacter Baumannii in A Renal Pancreas Transplant RecipientsserggiosNo ratings yet
- Evolution of Drug-Resistant Acinetobacter Baumannii After DCD Renal TransplantationDocument9 pagesEvolution of Drug-Resistant Acinetobacter Baumannii After DCD Renal TransplantationsserggiosNo ratings yet
- A Retrospective Review at Two US TransplantDocument6 pagesA Retrospective Review at Two US TransplantsserggiosNo ratings yet
- Recent Advances and Clinical Outcomes of Kidney TransplantationDocument18 pagesRecent Advances and Clinical Outcomes of Kidney TransplantationsserggiosNo ratings yet
- Systematic Review of Metabolic Syndrome Biomarkers: A Panel For Early Detection, Management, and Risk Stratification in The West Virginian PopulationDocument14 pagesSystematic Review of Metabolic Syndrome Biomarkers: A Panel For Early Detection, Management, and Risk Stratification in The West Virginian PopulationDany RamdhaniNo ratings yet
- UK Standards for Microbiology Investigations: Detection of Enterobacteriaceae producing Extended Spectrum β-LactamasesDocument28 pagesUK Standards for Microbiology Investigations: Detection of Enterobacteriaceae producing Extended Spectrum β-LactamasessserggiosNo ratings yet
- Kidney TransplantationDocument4 pagesKidney TransplantationsserggiosNo ratings yet
- Reviews: The Spectrum of Celiac Disease: Epidemiology, Clinical Aspects and TreatmentDocument10 pagesReviews: The Spectrum of Celiac Disease: Epidemiology, Clinical Aspects and TreatmentsserggiosNo ratings yet
- Report of Twenty CasesDocument16 pagesReport of Twenty CasessserggiosNo ratings yet
- Annsurg01228 0005Document12 pagesAnnsurg01228 0005sserggiosNo ratings yet
- BMJ 336 7638 CR 00269Document4 pagesBMJ 336 7638 CR 00269sserggiosNo ratings yet
- The Molecular Investigation of Celiac DiseaseDocument7 pagesThe Molecular Investigation of Celiac DiseasesserggiosNo ratings yet
- Paper 1Document9 pagesPaper 1sserggiosNo ratings yet
- Exercise Stress TestingDocument54 pagesExercise Stress TestingSaranya R S100% (2)
- iHFG Part B Cardiac Investigation UnitDocument21 pagesiHFG Part B Cardiac Investigation UnitEmmanuel OENo ratings yet
- Leading A Culture of Safety-A Blueprint For SuccessDocument48 pagesLeading A Culture of Safety-A Blueprint For Successsaphena parvaNo ratings yet
- S2HY SlideHandoutsDocument511 pagesS2HY SlideHandoutsDorin Cristian AntalNo ratings yet
- Treadmill ThesisDocument8 pagesTreadmill Thesislaurenbrownprovo100% (2)
- Introduction To Exercise PrescriptionDocument46 pagesIntroduction To Exercise PrescriptionabhijeetNo ratings yet
- Previous Question Paper 1 CardiologyDocument5 pagesPrevious Question Paper 1 CardiologyDeepthi DNo ratings yet
- Step 2 CK Review - CardiologyDocument28 pagesStep 2 CK Review - Cardiologyrsmd1986100% (1)
- Isokinetic Muscular Strength and - Aerobic - Physical.43Document8 pagesIsokinetic Muscular Strength and - Aerobic - Physical.43Fabricio BoscoloNo ratings yet
- Exercise Stress TestingDocument18 pagesExercise Stress TestingSereinNo ratings yet
- Yap, Dran - Cardio Module 1Document8 pagesYap, Dran - Cardio Module 1Dran YapNo ratings yet
- Preoperative Cardiopulmonary Exercise Testing Improves Risk Assessment of Morbidity and Length of Stay Following Cytoreductive Surgery With Hyperthermic Intraperitoneal ChemotherapyDocument10 pagesPreoperative Cardiopulmonary Exercise Testing Improves Risk Assessment of Morbidity and Length of Stay Following Cytoreductive Surgery With Hyperthermic Intraperitoneal ChemotherapyJoao da HoraNo ratings yet
- ACSM Health/Fitness Instructor ExamDocument25 pagesACSM Health/Fitness Instructor ExamRosendo Smith100% (1)
- Exercise Stress TestDocument22 pagesExercise Stress Testafrin nirfaNo ratings yet
- Multi-Slice CT For Coronary Calcium Scoring and Coronary AngiographyDocument63 pagesMulti-Slice CT For Coronary Calcium Scoring and Coronary AngiographyAnnisaa FitrianiNo ratings yet
- AHA ACC Test Ergo Met RicoDocument56 pagesAHA ACC Test Ergo Met RicoValentina VaccaroNo ratings yet
- Genres Reader 2014 PDFDocument305 pagesGenres Reader 2014 PDFMarina PenelopeNo ratings yet
- A Case of Myocardial Bridging: Marco Guglielmo, MD, Feacvi, FSCCTDocument23 pagesA Case of Myocardial Bridging: Marco Guglielmo, MD, Feacvi, FSCCTRaul CincaNo ratings yet
- Operative Orthopaedics Stanmore Guide 2010Document329 pagesOperative Orthopaedics Stanmore Guide 2010Shourjendra Datta100% (11)
- MF3 - Ischemic Heart DiseaseDocument28 pagesMF3 - Ischemic Heart DiseaseAnnbe BarteNo ratings yet
- 2012 Guidelines StableIschemicHeartDisease 11-20-12Document121 pages2012 Guidelines StableIschemicHeartDisease 11-20-12cephalicaNo ratings yet
- Diagnostic Evaluation of The HeartDocument3 pagesDiagnostic Evaluation of The HeartClaire GidoNo ratings yet
- Diagnosis and Management of Stable AnginaDocument14 pagesDiagnosis and Management of Stable AnginaDiosvel José SarmientoNo ratings yet
- Cardiac Stress TestingDocument90 pagesCardiac Stress TestingFrancesca Isabel BunyiNo ratings yet
- Coronary Artery DiseaseDocument15 pagesCoronary Artery Diseasektae337No ratings yet
- Thoracic Post Op Complications PDFDocument169 pagesThoracic Post Op Complications PDFMayang Nurul100% (1)
- ASE Reference Book PDFDocument68 pagesASE Reference Book PDFrentedmule00No ratings yet
- Treatment Guidelines PDFDocument293 pagesTreatment Guidelines PDFgautambobNo ratings yet