You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- A Clinical Experience Natrum Mur Cures A Female With MenorrhagiaDocument4 pagesA Clinical Experience Natrum Mur Cures A Female With MenorrhagiaHomoeopathic PulseNo ratings yet
- Physical Exam: Anesthetic Plan: Asa #Document1 pagePhysical Exam: Anesthetic Plan: Asa #Jeremy-ann HamNo ratings yet
- Diathermy in SurgeryDocument31 pagesDiathermy in Surgeryrosybash100% (1)
- Perineal Tear: AnatomyDocument4 pagesPerineal Tear: AnatomySuhas IngaleNo ratings yet
- Fitzpatrick Summer Comp SummaryDocument13 pagesFitzpatrick Summer Comp Summaryapi-247574390No ratings yet
- Ali - Final Clinical Project CsiDocument15 pagesAli - Final Clinical Project Csiapi-247574390No ratings yet
- Ali - Service Learning IIDocument6 pagesAli - Service Learning IIapi-247574390No ratings yet
- Medical Dosimetry Resume - Ali FitzpatrickDocument2 pagesMedical Dosimetry Resume - Ali Fitzpatrickapi-247574390No ratings yet
- Dosimetry - Parotid Clinical LabDocument15 pagesDosimetry - Parotid Clinical Labapi-247574390No ratings yet
- Comprehensive Case Study 2014 - Fifth DraftDocument15 pagesComprehensive Case Study 2014 - Fifth Draftapi-247574390No ratings yet
- Dosimetry - Clinical Practicum 1 Feb Case StudyDocument9 pagesDosimetry - Clinical Practicum 1 Feb Case Studyapi-247574390No ratings yet
- Dosimetry - Mentoring EssayDocument8 pagesDosimetry - Mentoring Essayapi-247574390No ratings yet
- Dosimetry - Service Learning IIDocument6 pagesDosimetry - Service Learning IIapi-247574390No ratings yet
- LeesummaryDocument11 pagesLeesummaryapi-247490129No ratings yet
- Dosimetry - Clinical Practicum 1 Comp EvalDocument3 pagesDosimetry - Clinical Practicum 1 Comp Evalapi-247574390No ratings yet
- Dosimetry - Conformal Treatment DiscussionDocument3 pagesDosimetry - Conformal Treatment Discussionapi-247574390No ratings yet
- Dosimetry - Clinical Practicum 1 March Case StudyDocument11 pagesDosimetry - Clinical Practicum 1 March Case Studyapi-247574390No ratings yet
- Dosimetry - Clinical Practicum 1 April Case StudyDocument14 pagesDosimetry - Clinical Practicum 1 April Case Studyapi-247574390No ratings yet
- Dosimetry - Research Diss 3 WeeblyDocument6 pagesDosimetry - Research Diss 3 Weeblyapi-247574390No ratings yet
- Dosimetry - Clinical Practicum 1 Prostate Clinical LabDocument3 pagesDosimetry - Clinical Practicum 1 Prostate Clinical Labapi-247574390No ratings yet
- Dosimetry - Clinical Practicum 1 Brain Clinical LabDocument2 pagesDosimetry - Clinical Practicum 1 Brain Clinical Labapi-247574390No ratings yet
- Ama Challenge 2012Document3 pagesAma Challenge 2012api-174496267No ratings yet
- Statistics ActivityDocument5 pagesStatistics Activityapi-239878826No ratings yet
- Dosimetry - Brachytherapy Diss 3Document3 pagesDosimetry - Brachytherapy Diss 3api-247574390No ratings yet
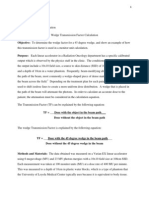
- Dosimetry - Dose Wedge Factor PaperDocument9 pagesDosimetry - Dose Wedge Factor Paperapi-247574390No ratings yet
- Dosimetry - Treatment Hetero PaperDocument8 pagesDosimetry - Treatment Hetero Paperapi-247574390No ratings yet
- Neutral Zone Technique-JCDocument43 pagesNeutral Zone Technique-JCmujtaba100% (1)
- Nur 460 Capstone Practicum Experience 4Document1 pageNur 460 Capstone Practicum Experience 4api-449295277No ratings yet
- AcsDocument103 pagesAcsVikrant WankhedeNo ratings yet
- EpilepsyDocument2 pagesEpilepsyfreezblueyNo ratings yet
- Creating A Sustainable Rural General Surgery WorkforceDocument13 pagesCreating A Sustainable Rural General Surgery WorkforceJeff CrocombeNo ratings yet
- Advocacy LetterDocument2 pagesAdvocacy Letterapi-236671577No ratings yet
- Daftar Pustaka ReferatDocument2 pagesDaftar Pustaka ReferatWidyastutiNo ratings yet
- Goldberg 1970Document8 pagesGoldberg 1970Ria Rizki JayantiNo ratings yet
- Placenta Umbilical CordDocument39 pagesPlacenta Umbilical Cordbel4ronaldoeNo ratings yet
- ArdconDocument2 pagesArdconडा. सत्यदेव त्यागी आर्यNo ratings yet
- M3 CiaDocument2 pagesM3 CiaApplePi SimpNo ratings yet
- Perceived Competence in Cardiopulmonary Resuscitation, Knowledge and Skills, Amongst 50 Qualified NursesDocument6 pagesPerceived Competence in Cardiopulmonary Resuscitation, Knowledge and Skills, Amongst 50 Qualified NursesYannis ZoldenbergNo ratings yet
- Oral Contraceptives For Functional Ovarian Cysts (Review) : CochraneDocument32 pagesOral Contraceptives For Functional Ovarian Cysts (Review) : CochraneAvneet KaurNo ratings yet
- Milestones of Fetal Growth and Development EssayDocument2 pagesMilestones of Fetal Growth and Development EssayZoe Dominique GudioNo ratings yet
- Brody 2006 Prolactin BPDocument4 pagesBrody 2006 Prolactin BPBassu RazvanNo ratings yet
- Vats and Post Op CareDocument18 pagesVats and Post Op CareVenz100% (1)
- 1AA17AT009 - Trauma Centre by Ananya KulkarniDocument43 pages1AA17AT009 - Trauma Centre by Ananya KulkarniSakshi RangnekarNo ratings yet
- Cord Prolapse ScriptDocument9 pagesCord Prolapse ScriptDarwin QuirimitNo ratings yet
- Fourth Year Logbook: Hawler Medical University College of Medicine Department of Medicine 2019-2020Document9 pagesFourth Year Logbook: Hawler Medical University College of Medicine Department of Medicine 2019-2020asia groupNo ratings yet
- Bingo Powerpoint v3 Answers AZCOM RadiologyDocument76 pagesBingo Powerpoint v3 Answers AZCOM Radiologyk5c4s89No ratings yet
- Pediatrics Clinics 2006 (Vol 53, No 4, Aug 2006) (Elsevier) WWDocument249 pagesPediatrics Clinics 2006 (Vol 53, No 4, Aug 2006) (Elsevier) WWGeorgiana Combei Ungureanu100% (1)
- Pulmonary Hypertension Associated With Bronchopulmonary Dysplasia A ReviewDocument9 pagesPulmonary Hypertension Associated With Bronchopulmonary Dysplasia A ReviewEduardo Rios DuboisNo ratings yet
- Report ViewerDocument1 pageReport Vieweradnanakhan622No ratings yet
- BreastfeedingDocument2 pagesBreastfeedingArianne KimNo ratings yet
- Endoscopic Insertion of Tympanostomy Tube in ChildrenDocument5 pagesEndoscopic Insertion of Tympanostomy Tube in ChildrenInternational Jpurnal Of Technical Research And ApplicationsNo ratings yet
- The Multidisciplinary Heart Team in Cardiovascular Medicine: Current Role and Future ChallengesDocument13 pagesThe Multidisciplinary Heart Team in Cardiovascular Medicine: Current Role and Future ChallengesMarco Palacios QuezadaNo ratings yet