You might also like
- PREECLAMPSIADocument9 pagesPREECLAMPSIAZAY EMNo ratings yet
- Gestational DiabetesDocument6 pagesGestational DiabetesZAY EMNo ratings yet
- DR - Reshma J.: PHD Scholar Batch 2020Document27 pagesDR - Reshma J.: PHD Scholar Batch 2020Farhana AbirNo ratings yet
- High Risk Pregnancy NewDocument16 pagesHigh Risk Pregnancy NewSurya SasidharanNo ratings yet
- Intro To High Risk PregnancyDocument10 pagesIntro To High Risk PregnancyKenneth Jake Quinagon TayabanNo ratings yet
- PIHDocument4 pagesPIHAngelica Floreza DullasNo ratings yet
- Understanding PreeclampsiaDocument11 pagesUnderstanding PreeclampsiaZoe Jeanne GarcianoNo ratings yet
- Preterm Labor (Delivery Room)Document6 pagesPreterm Labor (Delivery Room)Mara PhotxNo ratings yet
- Eclampsia and PreeclampsiaDocument5 pagesEclampsia and PreeclampsiaGerome Michael Masendo BeliranNo ratings yet
- Pregnancy Induced Hypertension: DefinitionDocument7 pagesPregnancy Induced Hypertension: Definitionkristine hinaresNo ratings yet
- Symptoms: by Mayo Clinic StaffDocument11 pagesSymptoms: by Mayo Clinic StaffSheryl OcampoNo ratings yet
- PreeclampsiaDocument1 pagePreeclampsiaapi-302415380No ratings yet
- Pregnancy Induced Hypertension (Pih) Nursing Management: EfinitionDocument3 pagesPregnancy Induced Hypertension (Pih) Nursing Management: Efinitiongebremeskel tikueNo ratings yet
- Alh 2220 Preeclampsia Research PaperDocument9 pagesAlh 2220 Preeclampsia Research Paperapi-431367905No ratings yet
- Nasterea Prematura Sarcina PrelungitaDocument34 pagesNasterea Prematura Sarcina PrelungitaelyssyNo ratings yet
- Pregnant Woman Emergency Clinical CaseDocument210 pagesPregnant Woman Emergency Clinical CaseAillenne AlambraNo ratings yet
- Health Education For Record BookDocument24 pagesHealth Education For Record BookRoselineTiggaNo ratings yet
- Case Study CP 104Document22 pagesCase Study CP 104Mor Shi DA BalutintikNo ratings yet
- IrishDocument5 pagesIrishmahin2gurlNo ratings yet
- Hypertensive Disorders of PregnancyDocument1 pageHypertensive Disorders of PregnancyMiko AragonNo ratings yet
- Preeclampsia and High Blood Pressure During Pregnancy-ACOGDocument6 pagesPreeclampsia and High Blood Pressure During Pregnancy-ACOGrenaNo ratings yet
- Case Pres Except PATHO at PADocument99 pagesCase Pres Except PATHO at PAHanwell Keith SantosNo ratings yet
- Infant of Diabetic MotherDocument14 pagesInfant of Diabetic MothersreekalaNo ratings yet
- Preeclampsia and High Blood Pressure ACOGDocument4 pagesPreeclampsia and High Blood Pressure ACOGAvicena M IqbalNo ratings yet
- Or Cases InfoDocument83 pagesOr Cases InfoAmirace ValenciaNo ratings yet
- High Blood Pressure: Gestational DiabetesDocument2 pagesHigh Blood Pressure: Gestational DiabetesKarlo ReyesNo ratings yet
- Severe Preeclampsia SymptomsDocument4 pagesSevere Preeclampsia SymptomsKristine Dela CruzNo ratings yet
- Preeclampsia: ¿Quién Está en Riesgo de La Preeclampsia?Document7 pagesPreeclampsia: ¿Quién Está en Riesgo de La Preeclampsia?juliana sotoNo ratings yet
- Importance of Prenatal CareDocument12 pagesImportance of Prenatal CarePinkymekala HasanparthyNo ratings yet
- Preterm LaborDocument3 pagesPreterm LaborMin AmadorNo ratings yet
- Preeclampsia Falco 1Document11 pagesPreeclampsia Falco 1emailNo ratings yet
- Thalassaemia Syndromes and PregnancyDocument8 pagesThalassaemia Syndromes and PregnancyWahyu PermataNo ratings yet
- RH Incompatibility HandoutDocument4 pagesRH Incompatibility HandoutMaricar Sanson FelicianoNo ratings yet
- The Early Signs of PregnancyDocument4 pagesThe Early Signs of PregnancyTomy Well100% (1)
- Postpartum Clinical QuizDocument6 pagesPostpartum Clinical QuizAmy100% (1)
- Risk factors for high-risk pregnanciesDocument3 pagesRisk factors for high-risk pregnanciesWindySeptianiIshakNo ratings yet
- High-Risk Pregnancy: The Internet Journal of Gynecology and ObstetricsDocument16 pagesHigh-Risk Pregnancy: The Internet Journal of Gynecology and ObstetricsWidelmark FarrelNo ratings yet
- The Internet Journal of Gynecology and ObstetricsDocument8 pagesThe Internet Journal of Gynecology and Obstetricsrett_ttaNo ratings yet
- Factors That Can Lead to a High-Risk PregnancyDocument6 pagesFactors That Can Lead to a High-Risk PregnancyRajalakshmiNo ratings yet
- HRPGDDocument16 pagesHRPGDyuastikapsNo ratings yet
- Case Presentation PreeclampsiaDocument41 pagesCase Presentation PreeclampsiaJomari Zapanta50% (2)
- Pregnancy Induced HypertensionDocument3 pagesPregnancy Induced HypertensionunagraciaNo ratings yet
- عرض تقديميDocument24 pagesعرض تقديميAlibeyatliNo ratings yet
- Presentation Pre EclampsiaDocument25 pagesPresentation Pre EclampsiaChidube UkachukwuNo ratings yet
- 3 Trimester CompicationsDocument33 pages3 Trimester CompicationsAyesha MeloNo ratings yet
- Assignment ON Diabetic BabyDocument12 pagesAssignment ON Diabetic BabyPriyaNo ratings yet
- The Basics of PregnancyDocument4 pagesThe Basics of PregnancyTomy WellNo ratings yet
- Complications of Bleeding Disorders in PregnancyDocument11 pagesComplications of Bleeding Disorders in PregnancyNursing ReviewerNo ratings yet
- Pre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Cause & EffectsDocument2 pagesCause & EffectsMerly Grael LigligenNo ratings yet
- Introduction To PreeclampsiaDocument3 pagesIntroduction To PreeclampsiaRandy_Jecson_8962No ratings yet
- Case Study - Incomplete Abortion Related To APSDocument8 pagesCase Study - Incomplete Abortion Related To APSRomeo ReyesNo ratings yet
- 3 Trimester CompicationsDocument37 pages3 Trimester CompicationsAyesha MeloNo ratings yet
- EclampsiaDocument18 pagesEclampsiaTipey SegismundoNo ratings yet
- Preeclampsia and High Blood Pressure During Pregnancy: Frequently Asked Questions FAQ034 PregnancyDocument4 pagesPreeclampsia and High Blood Pressure During Pregnancy: Frequently Asked Questions FAQ034 PregnancyTjoema AsriNo ratings yet
- Eclampsia Overview: Pregnancy Pregnant Preeclampsia High Blood Pressure Coma ToxemiaDocument5 pagesEclampsia Overview: Pregnancy Pregnant Preeclampsia High Blood Pressure Coma ToxemiaReyner Waynne Louise EmongNo ratings yet
- Antenatal Care and HealthDocument17 pagesAntenatal Care and HealthInggrit WulansariNo ratings yet
- Patalita PresentationDocument21 pagesPatalita PresentationkrezeltayaNo ratings yet
- Managing Your Gestational Diabetes: A Guide for You and Your Baby's Good HealthFrom EverandManaging Your Gestational Diabetes: A Guide for You and Your Baby's Good HealthRating: 1 out of 5 stars1/5 (2)
- Gestational Diabetes Diet: A Beginner's 3-Week Step-by-Step Guide with Curated Recipes and a Meal PlanFrom EverandGestational Diabetes Diet: A Beginner's 3-Week Step-by-Step Guide with Curated Recipes and a Meal PlanNo ratings yet
- Let's Crossword!: About This ActivityDocument1 pageLet's Crossword!: About This ActivityKaty-Gianina Strugaru50% (2)
- Lets Crossword Treble Clef SheetDocument1 pageLets Crossword Treble Clef SheetAnonymous pRPtEPwFhE100% (1)
- BrochureDocument18 pagesBrochureJascinth Sabanal - LumahangNo ratings yet
- Mental DisordersDocument12 pagesMental DisordersJascinth Sabanal - LumahangNo ratings yet
- Chapter Vii - Community Tax Sec. 285. Community Tax The City Hereby Levy's Community Tax in Lieu of Former Residence Tax Levied andDocument12 pagesChapter Vii - Community Tax Sec. 285. Community Tax The City Hereby Levy's Community Tax in Lieu of Former Residence Tax Levied andJascinth Sabanal - LumahangNo ratings yet
- A Detailed Lesson Plan on Jumping in Physical EducationDocument7 pagesA Detailed Lesson Plan on Jumping in Physical EducationJascinth Sabanal - Lumahang100% (6)
- Movie A Beautiful MindDocument3 pagesMovie A Beautiful Mindhang doNo ratings yet
- Nursing Care Plan for Placenta Previa with Impaired Fetal Gas ExchangeDocument2 pagesNursing Care Plan for Placenta Previa with Impaired Fetal Gas ExchangeJc RocuyanNo ratings yet
- The 14 Disability CategoriesDocument1 pageThe 14 Disability CategoriesFrance Bejosa100% (1)
- Kode ICdDocument5 pagesKode ICdAudiah F HadinataNo ratings yet
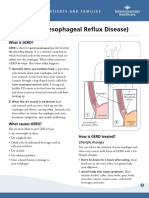
- GERD Gastroesophageal Reflux Disease Fact SheetDocument2 pagesGERD Gastroesophageal Reflux Disease Fact SheetFatimah FadilahNo ratings yet
- 08 INSARAG Patient Treatment Record PDFDocument1 page08 INSARAG Patient Treatment Record PDFluisacocaliNo ratings yet
- Orthopedic Impairment PDFDocument15 pagesOrthopedic Impairment PDFjoan arreolaNo ratings yet
- Clinical StagingDocument22 pagesClinical StagingMarcosNo ratings yet
- (B) Evaluate The Characteristics, Types and Measures of Schizophrenia and Psychotic Disorders, Including A Discussion of Case StudiesDocument1 page(B) Evaluate The Characteristics, Types and Measures of Schizophrenia and Psychotic Disorders, Including A Discussion of Case StudiesHenry Nguyen PhamNo ratings yet
- Surgical Management: SurgeryDocument5 pagesSurgical Management: SurgeryKarl Angelo MontanoNo ratings yet
- AutismDocument26 pagesAutismminangsung minangnengNo ratings yet
- Lateralizing Value of Todd's PalsyDocument3 pagesLateralizing Value of Todd's PalsyLakshya J BasumataryNo ratings yet
- BrochureDocument2 pagesBrochureapi-282047984No ratings yet
- Algorithm-ACLS Suspected Stroke 200612Document1 pageAlgorithm-ACLS Suspected Stroke 200612Kavya Shree100% (3)
- Updated BLS Unit of Competencies As of 041822 Part 2ADocument81 pagesUpdated BLS Unit of Competencies As of 041822 Part 2AAL Babaran CanceranNo ratings yet
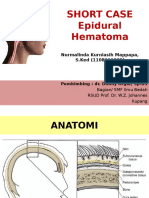
- SHORT CASE 1 Epidural HematomaDocument30 pagesSHORT CASE 1 Epidural HematomaNurmalinda MappapaNo ratings yet
- Plab2 Stations Topics New Old PDFDocument6 pagesPlab2 Stations Topics New Old PDFBeaulahNo ratings yet
- Revalida TopicsDocument3 pagesRevalida TopicsHaya CacayanNo ratings yet
- Discharge SummaryDocument1 pageDischarge SummaryBhagyashreeNo ratings yet
- Dr. Reno Rudiman Update on SepsisDocument20 pagesDr. Reno Rudiman Update on SepsisIvanRaykaNo ratings yet
- Alcohol WithdrawalDocument6 pagesAlcohol WithdrawalSangkaran KumarNo ratings yet
- FY10 ICD-9-CM Procedure Codes Linked To NHSN Operative Procedure CategoriesDocument22 pagesFY10 ICD-9-CM Procedure Codes Linked To NHSN Operative Procedure CategoriesYohan Julian Mega NandaNo ratings yet
- Altered Mental StateDocument2 pagesAltered Mental Stateizzati94No ratings yet
- SIF Determination & CategorizationDocument1 pageSIF Determination & CategorizationJosé ArévalosNo ratings yet
- Restless Leg Syndrome: The Most Common Disorder You Have Never Heard Of."Document20 pagesRestless Leg Syndrome: The Most Common Disorder You Have Never Heard Of."Maulida Manurung100% (1)
- Diagnosis of A Shared Psychotic DisorderDocument2 pagesDiagnosis of A Shared Psychotic DisorderTalia SchwartzNo ratings yet
- Assessing opioid withdrawalDocument3 pagesAssessing opioid withdrawalSergioMSaraivaNo ratings yet
- Final EPQDocument19 pagesFinal EPQtanishasen4No ratings yet
- DSM 5 Descriptions of Bipolar, Anxiety and Depressive DisordersDocument78 pagesDSM 5 Descriptions of Bipolar, Anxiety and Depressive DisordersJasmine FuyureNo ratings yet
- A Practical Guide To Treatment of Childhood Absence EpilepsyDocument10 pagesA Practical Guide To Treatment of Childhood Absence EpilepsyLorenz BelloNo ratings yet