You might also like
- Form - Student Health Certificate-1Document2 pagesForm - Student Health Certificate-1hmhida33% (3)
- CBO UPK Registration PacketDocument9 pagesCBO UPK Registration Packetstar5449No ratings yet
- KHA - 1-11 Kindergarten Health Assessment Report NCDHHS NCDPIDocument2 pagesKHA - 1-11 Kindergarten Health Assessment Report NCDHHS NCDPIA.P. DillonNo ratings yet
- Kaiser Application FormsDocument1 pageKaiser Application FormsdcpanganibanNo ratings yet
- Diploma Module 1Document283 pagesDiploma Module 1Joseph OyomNo ratings yet
- Math Anxiety The Math GapDocument10 pagesMath Anxiety The Math Gapapi-443776228No ratings yet
- Christmas Plans Members PDFDocument179 pagesChristmas Plans Members PDFAndrei DinuNo ratings yet
- Management of Early Childhood Education Program (ECE 18)Document45 pagesManagement of Early Childhood Education Program (ECE 18)Fretzel Vann Ayoon100% (2)
- International School Guidebook PDFDocument117 pagesInternational School Guidebook PDFDavidNo ratings yet
- Florida School Entry Health ExamDocument2 pagesFlorida School Entry Health ExamPeterBurkeNo ratings yet
- DHS CFS 600 Certificate of Child Examination Form IL444-4737Document2 pagesDHS CFS 600 Certificate of Child Examination Form IL444-4737ArtueroNo ratings yet
- School Medical Examination FormDocument2 pagesSchool Medical Examination FormElite Mission HospitalNo ratings yet
- HealthapprasalDocument2 pagesHealthapprasalapi-235111661No ratings yet
- Health DeclarationDocument5 pagesHealth Declarationust dol100% (1)
- Student Application 2008Document15 pagesStudent Application 2008mariavrfNo ratings yet
- Abcd Early Learning Application Packet: Office Use OnlyDocument11 pagesAbcd Early Learning Application Packet: Office Use OnlyrockyNo ratings yet
- Nternational Chool Anila: STUDENT ID# - Please Print The Information Requested BelowDocument4 pagesNternational Chool Anila: STUDENT ID# - Please Print The Information Requested Belowainsleydevilla8079No ratings yet
- School Entry Health Exam Form FL (Sample)Document2 pagesSchool Entry Health Exam Form FL (Sample)chase1828No ratings yet
- UHS Employee Health Info FormDocument7 pagesUHS Employee Health Info FormCrystal AnnNo ratings yet
- 8th Grade Opt Out Form 2014Document1 page8th Grade Opt Out Form 2014Olivia NovakNo ratings yet
- Application IMPH Program Israel 2012-2013Document6 pagesApplication IMPH Program Israel 2012-2013Habla GuateNo ratings yet
- Registration Form - TCSDocument2 pagesRegistration Form - TCSSP.PrimersNo ratings yet
- AP Medical ReportDocument3 pagesAP Medical ReportKatia KatiaNo ratings yet
- Health DeclarationDocument2 pagesHealth Declarationemilyaguinod35No ratings yet
- Health Declaration and Medical Examination Form: Scholarship DivisionDocument5 pagesHealth Declaration and Medical Examination Form: Scholarship Divisionnazrin sarajuddinNo ratings yet
- A B Epsdt S T F: PpendixDocument20 pagesA B Epsdt S T F: PpendixasadNo ratings yet
- Medical Application Form: Insured Name: Inception DateDocument3 pagesMedical Application Form: Insured Name: Inception DateDidier G PeñuelaNo ratings yet
- DHA Medical FormsDocument3 pagesDHA Medical Formsfifth193No ratings yet
- Juvenile - FMR - PDF For MINORDocument2 pagesJuvenile - FMR - PDF For MINORHemant JhaNo ratings yet
- Health History FormDocument4 pagesHealth History Formganesh chowdaryNo ratings yet
- Maryland Occ1215Document3 pagesMaryland Occ1215why2kliuNo ratings yet
- Health Assessment Record: State of Connecticut Department of EducationDocument3 pagesHealth Assessment Record: State of Connecticut Department of EducationVishwanath SinduvadiNo ratings yet
- Application Form For Scholarship and Student Financial Assistance ProgramsDocument8 pagesApplication Form For Scholarship and Student Financial Assistance ProgramsXandra Yzabelle T. EbdalinNo ratings yet
- Dental Explorers Program Summer 2011 Application For ParticipationDocument4 pagesDental Explorers Program Summer 2011 Application For ParticipationuscblogsNo ratings yet
- Health DeclarationDocument2 pagesHealth Declarationrosabelromero09No ratings yet
- Prin. L.N.Welingkar Institute of Management Development and ResearchDocument4 pagesPrin. L.N.Welingkar Institute of Management Development and ResearchKavish JainNo ratings yet
- Admissions Application 2011-2012Document4 pagesAdmissions Application 2011-2012Rodrick SamuelsNo ratings yet
- 5ab OralHealth NotificationLetter - AssessmentWaiver FormDocument3 pages5ab OralHealth NotificationLetter - AssessmentWaiver FormGenevieve AlcalaNo ratings yet
- CSC Proforma - GeneralDocument6 pagesCSC Proforma - General127 Shruthik Patel ThotaNo ratings yet
- Medical Examination 5Document1 pageMedical Examination 5Melanie AgustinNo ratings yet
- ICICI Prudential Life Insurance Co LTD - Attachment - 6Document2 pagesICICI Prudential Life Insurance Co LTD - Attachment - 6vermalabNo ratings yet
- UHSAA Preparticipation FormDocument4 pagesUHSAA Preparticipation FormThe Salt Lake TribuneNo ratings yet
- Enrolment Form ECD SchoolDocument5 pagesEnrolment Form ECD SchooleliahNo ratings yet
- Lifestyle Department Student Information - Fillable v2Document8 pagesLifestyle Department Student Information - Fillable v2Daniel TepermanNo ratings yet
- Reach 52 ProfilingDocument3 pagesReach 52 ProfilingJer SonNo ratings yet
- Consent Form EnglishDocument2 pagesConsent Form Englishapi-299052382No ratings yet
- DM No. 296 S. 2022 Medical and Dental Assessment Profiling of School LearnersDocument10 pagesDM No. 296 S. 2022 Medical and Dental Assessment Profiling of School LearnersGemmarlyn TingNo ratings yet
- Health Questionnaire FormDocument7 pagesHealth Questionnaire FormSadaf ShaukatNo ratings yet
- Department of Education: Directions: The Following Are Medical Conditions That Are ConsideredDocument2 pagesDepartment of Education: Directions: The Following Are Medical Conditions That Are ConsideredRENEBOY SAY-ANo ratings yet
- Members Application Form: Name & Surname ID NumberDocument8 pagesMembers Application Form: Name & Surname ID NumberJacques MorrisonNo ratings yet
- PAR1514 Medical HistoryDocument5 pagesPAR1514 Medical Historyloxav71284No ratings yet
- Occupational Health QuestionnaireDocument13 pagesOccupational Health QuestionnaireMohamed HafezNo ratings yet
- Physician S Health Evaluation FormDocument2 pagesPhysician S Health Evaluation FormJessica Mayleen MartinezNo ratings yet
- Health AssessmentDocument2 pagesHealth AssessmentfahrezaSRNo ratings yet
- MM Fellowship Primary Application '10-'11Document6 pagesMM Fellowship Primary Application '10-'11USCBISCNo ratings yet
- A - FormDocument2 pagesA - FormKashifNo ratings yet
- Maklumat Penting - Atau Hospital/Klinik Swasta. - : Form Pd1Document9 pagesMaklumat Penting - Atau Hospital/Klinik Swasta. - : Form Pd1Syazwi BaharuddinNo ratings yet
- Peha FormsDocument7 pagesPeha FormsCode OneNo ratings yet
- Caregiver MedicalDocument2 pagesCaregiver Medicaloliverfox654No ratings yet
- Session 3 Registration PacketDocument4 pagesSession 3 Registration PacketASYMCA YCONo ratings yet
- Immunization Titer FormsDocument19 pagesImmunization Titer FormsCole GarrettNo ratings yet
- Forms 1 5 For Registration 2021 Mame 1Document15 pagesForms 1 5 For Registration 2021 Mame 1Emma DionedaNo ratings yet
- Childhood Obesity: Causes and Consequences, Prevention and Management.From EverandChildhood Obesity: Causes and Consequences, Prevention and Management.No ratings yet
- Social Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsFrom EverandSocial Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsNo ratings yet
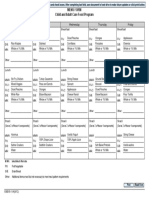
- Menu Form Child and Adult Care Food ProgramDocument1 pageMenu Form Child and Adult Care Food ProgramivyleagueelaNo ratings yet
- Ivy League Bronx Food Menu: Week 3Document1 pageIvy League Bronx Food Menu: Week 3ivyleagueelaNo ratings yet
- Manhattan MenuDocument5 pagesManhattan MenuivyleagueelaNo ratings yet
- Ivy League Bronx Food Menu: Week 1Document1 pageIvy League Bronx Food Menu: Week 1ivyleagueelaNo ratings yet
- Menu Form Child and Adult Care Food ProgramDocument1 pageMenu Form Child and Adult Care Food ProgramivyleagueelaNo ratings yet
- Bronx Edition: Note From The AdministrationDocument2 pagesBronx Edition: Note From The AdministrationivyleagueelaNo ratings yet
- Ivy League Bronx Food Menu: Week 4Document1 pageIvy League Bronx Food Menu: Week 4ivyleagueelaNo ratings yet
- Newsletter-October 2015 BaysideDocument2 pagesNewsletter-October 2015 BaysideivyleagueelaNo ratings yet
- Deer Park Ivy League E.L.A: November 2015 - Thanks and GivingDocument3 pagesDeer Park Ivy League E.L.A: November 2015 - Thanks and GivingivyleagueelaNo ratings yet
- Ivy League Bronx Food Menu: Week 2Document1 pageIvy League Bronx Food Menu: Week 2ivyleagueelaNo ratings yet
- March 2016 Deer ParkDocument3 pagesMarch 2016 Deer ParkivyleagueelaNo ratings yet
- Bayside Newsletter November 2015Document2 pagesBayside Newsletter November 2015ivyleagueelaNo ratings yet
- Deer Park Ivy League E.L.A: January 2015 - Happy New Year!Document3 pagesDeer Park Ivy League E.L.A: January 2015 - Happy New Year!ivyleagueelaNo ratings yet
- Newsletter - August 2015 BaysideDocument2 pagesNewsletter - August 2015 BaysideivyleagueelaNo ratings yet
- Bronx September NewsletterDocument3 pagesBronx September NewsletterivyleagueelaNo ratings yet
- October Newsletter 2015 BronxDocument2 pagesOctober Newsletter 2015 BronxivyleagueelaNo ratings yet
- Bayside September NewsletterDocument2 pagesBayside September NewsletterivyleagueelaNo ratings yet
- August 2015 Newsletter Staten IslandDocument1 pageAugust 2015 Newsletter Staten IslandivyleagueelaNo ratings yet
- Scope and Sequence 2015-2016Document4 pagesScope and Sequence 2015-2016ivyleagueelaNo ratings yet
- Deer Park Ivy League E.L.A: August 2015 - Midsummer Fun!Document3 pagesDeer Park Ivy League E.L.A: August 2015 - Midsummer Fun!ivyleagueelaNo ratings yet
- Ivy League Early Learning Academy: Bronx Edition June 2015Document6 pagesIvy League Early Learning Academy: Bronx Edition June 2015ivyleagueelaNo ratings yet
- Ivy League Early Learning Academy: Bronx Edition May 2015Document5 pagesIvy League Early Learning Academy: Bronx Edition May 2015ivyleagueelaNo ratings yet
- Deer Park Ivy League E.L.A: May 2015 - We Are Busy Bees!Document3 pagesDeer Park Ivy League E.L.A: May 2015 - We Are Busy Bees!ivyleagueelaNo ratings yet
- Ivy League Enrollment FormsDocument13 pagesIvy League Enrollment FormsivyleagueelaNo ratings yet
- Manhattan January 2015 FlyerDocument2 pagesManhattan January 2015 FlyerivyleagueelaNo ratings yet
- Ivy League Enrollment FormsDocument5 pagesIvy League Enrollment FormsivyleagueelaNo ratings yet
- Manhattan November 2014Document2 pagesManhattan November 2014ivyleagueelaNo ratings yet
- Domains 2-3Document1 pageDomains 2-3ivyleagueelaNo ratings yet
- Deer Park Ivy League E.L.A: October 2014 News - It Is October Already!Document3 pagesDeer Park Ivy League E.L.A: October 2014 News - It Is October Already!ivyleagueelaNo ratings yet
- Bronx October Newsletters 2014Document4 pagesBronx October Newsletters 2014ivyleagueelaNo ratings yet
- NJ 082813Document16 pagesNJ 082813sarahloren_thepressNo ratings yet
- New Legacy ELC Lead TeacherDocument3 pagesNew Legacy ELC Lead Teacheryunie poohNo ratings yet
- Bai Tap Thuc Hanh Anh 6 MlhdocxDocument116 pagesBai Tap Thuc Hanh Anh 6 MlhdocxNhã NguyễnNo ratings yet
- BEED Preschool ChecklistDocument6 pagesBEED Preschool ChecklistvisayasstateuNo ratings yet
- Learner's Home Guide (KINDER) Week 7: Advance Montessori Education Center of Isabela, Inc. Maligaya, Tumauini, IsabelaDocument3 pagesLearner's Home Guide (KINDER) Week 7: Advance Montessori Education Center of Isabela, Inc. Maligaya, Tumauini, IsabelaJesieca BulauanNo ratings yet
- Dingwall Primary Brochure 2016 17Document26 pagesDingwall Primary Brochure 2016 17Steven FlynnNo ratings yet
- Brown J D 2009 Language Curriculum DevelDocument22 pagesBrown J D 2009 Language Curriculum DevelDuchshund AleakimNo ratings yet
- Application For EmploymentDocument5 pagesApplication For EmploymentDewi Zulviana DariusNo ratings yet
- Education in India - WikipediaDocument185 pagesEducation in India - WikipediaAnu AnuNo ratings yet
- Schools: in and Around The Parramatta City Council AreaDocument11 pagesSchools: in and Around The Parramatta City Council AreaManish AgrawalNo ratings yet
- Educ-10 Chapter 3 Group ActDocument6 pagesEduc-10 Chapter 3 Group ActAliah MosqueraNo ratings yet
- Chapter Iii-The Code of Ethics For Professional Teachers:: Learning OutcomesDocument21 pagesChapter Iii-The Code of Ethics For Professional Teachers:: Learning OutcomesShaira B. Anonat Coed100% (2)
- Time Sample Play Pattern FormDocument6 pagesTime Sample Play Pattern Formapi-512270694No ratings yet
- Alyssa Kulik-ResumeDocument2 pagesAlyssa Kulik-Resumeapi-309886323No ratings yet
- Kayron International Schools Weekly Diary: Welcome BackDocument3 pagesKayron International Schools Weekly Diary: Welcome BackStan IkechukwuNo ratings yet
- Help With Child Development CourseworkDocument7 pagesHelp With Child Development Courseworkafiwjkfpc100% (2)
- The Effect of A Story - Based Programme On Developing Moral Values at The Kindergarten StageDocument26 pagesThe Effect of A Story - Based Programme On Developing Moral Values at The Kindergarten StagemariangoudNo ratings yet
- Newsletter - Spring 2012Document14 pagesNewsletter - Spring 2012אמיר סטרנסNo ratings yet
- Katherine Smith Final Montana ResumeDocument5 pagesKatherine Smith Final Montana Resumeapi-278225936No ratings yet
- Pennsylvania Kindergarten StandardsDocument92 pagesPennsylvania Kindergarten StandardsBarbara MillerNo ratings yet
- DEWA - Term ReportDocument34 pagesDEWA - Term ReportAthar Ali KhichiNo ratings yet
- Out of The Frying Pan, Into The Fire?Document4 pagesOut of The Frying Pan, Into The Fire?Speech & Language Therapy in PracticeNo ratings yet
- 5 3672 Ivica IvekovicDocument41 pages5 3672 Ivica IvekovicplavaadresaNo ratings yet
- Barney The Dinosaur's PageDocument5 pagesBarney The Dinosaur's PagechefchadsmithNo ratings yet
- University of Caloocan City Graduate SchoolDocument117 pagesUniversity of Caloocan City Graduate SchoolMay Ann RebambaNo ratings yet