You might also like
- Activity of Some Chemicals in The Control of Botrytis Cinerea On RosesDocument1 pageActivity of Some Chemicals in The Control of Botrytis Cinerea On RosesNada HrenNo ratings yet
- Meloxicam For DogsDocument2 pagesMeloxicam For DogsNada HrenNo ratings yet
- Maxflow CaDocument10 pagesMaxflow CaNada HrenNo ratings yet
- Flavours From AminoacidsDocument31 pagesFlavours From AminoacidsNada HrenNo ratings yet
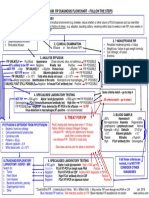
- Follow The Steps: 1. History 2. ? Effusive FipDocument1 pageFollow The Steps: 1. History 2. ? Effusive FipNada HrenNo ratings yet
- Journal of Virology-2018-Powers-e00649-18.full PDFDocument16 pagesJournal of Virology-2018-Powers-e00649-18.full PDFcfulton@maetrixgroup.comNo ratings yet
- Dickinson 2020 Antiviral Treatment Using The Adeno PDFDocument7 pagesDickinson 2020 Antiviral Treatment Using The Adeno PDFNada HrenNo ratings yet
- Control of Maillard Reactions in FoodsDocument16 pagesControl of Maillard Reactions in FoodsEdgardo Ed RamirezNo ratings yet
- Distillation HandbookDocument94 pagesDistillation HandbookEr Bali Pandhare100% (2)
- Using Feline Recombinant Omega InterferonDocument1 pageUsing Feline Recombinant Omega InterferonNada HrenNo ratings yet
- Chronic Nonregenerative Anemia - A ChallengeDocument3 pagesChronic Nonregenerative Anemia - A ChallengeNada HrenNo ratings yet
- Viruses: Clinical Aspects of Feline Retroviruses: A ReviewDocument27 pagesViruses: Clinical Aspects of Feline Retroviruses: A ReviewNada HrenNo ratings yet
- The Chemistry of Beef FlavorDocument16 pagesThe Chemistry of Beef FlavorNada Hren100% (1)
- Introduction To DistillationDocument39 pagesIntroduction To DistillationNada HrenNo ratings yet
- Biofertilizers PDFDocument18 pagesBiofertilizers PDFAmeet Kudche100% (1)
- Drainage Intraabdominal InfectionDocument5 pagesDrainage Intraabdominal InfectionNada HrenNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Psych-K Rob WilliamsDocument6 pagesPsych-K Rob WilliamsKamal Janjani67% (6)
- Abuses of Children in ClassroomDocument120 pagesAbuses of Children in ClassroomJulius de la CruzNo ratings yet
- The Competitive Imperative of LearningDocument9 pagesThe Competitive Imperative of LearningOmar S. HamdanNo ratings yet
- Hope-Focused Workbook (Created by Alexandra Wantke PsyD)Document34 pagesHope-Focused Workbook (Created by Alexandra Wantke PsyD)Jefferson Ferraz Terapeuta Familiar e CasalNo ratings yet
- FSDS Resources SDN - BHDDocument12 pagesFSDS Resources SDN - BHDRoslyna khanNo ratings yet
- Perioperative Nursing - OrIGINALDocument176 pagesPerioperative Nursing - OrIGINALJamil Lorca100% (4)
- Anxiolytic Assessment of Centella Asiatica With Elevated Zero Maze and Elevated Plus Maze in RatsDocument6 pagesAnxiolytic Assessment of Centella Asiatica With Elevated Zero Maze and Elevated Plus Maze in RatsSanjesh kumarNo ratings yet
- Fixed Space MaintainersDocument3 pagesFixed Space MaintainersElectricken21No ratings yet
- Infographic in PrinDocument1 pageInfographic in PrinShayne Angelique CongsonNo ratings yet
- EPA Methods 3015A, 3051A and 3052: Application NoteDocument3 pagesEPA Methods 3015A, 3051A and 3052: Application Noteade muchlasNo ratings yet
- Data Base EditDocument152 pagesData Base EditbobyNo ratings yet
- Fdi-Oral Cancer-Chairside GuideDocument2 pagesFdi-Oral Cancer-Chairside GuideHien TruongNo ratings yet
- C8-C10 Octocapric Acid - Safety Data SheetDocument8 pagesC8-C10 Octocapric Acid - Safety Data Sheetdaya vashishtNo ratings yet
- Debre Markos University College of Health Science Department of Public Health Epidemiology For 2 Year BSC in Medical Laboratory Science Students by Mengistie Kassahun (MPH in Field Epidemiology)Document55 pagesDebre Markos University College of Health Science Department of Public Health Epidemiology For 2 Year BSC in Medical Laboratory Science Students by Mengistie Kassahun (MPH in Field Epidemiology)Tewodros AntenehNo ratings yet
- Clean Up and Flourish or Pile Up and PerishDocument30 pagesClean Up and Flourish or Pile Up and Perishnehabhilare100% (1)
- Science 10-DDL4Document2 pagesScience 10-DDL4Jobaillah NaseefNo ratings yet
- Koch 2016Document7 pagesKoch 2016Derri PraNo ratings yet
- K2S-CW230907-BA6008-00005 - A01 - Manual Operated Valve Test ProcedureDocument13 pagesK2S-CW230907-BA6008-00005 - A01 - Manual Operated Valve Test ProcedureAzeta RobertNo ratings yet
- Behavior Based Safety HandoutsDocument7 pagesBehavior Based Safety HandoutsAnsarNo ratings yet
- Divide, Bullying and AddictionDocument54 pagesDivide, Bullying and AddictionRadical GraceNo ratings yet
- IELTS FOUNDATION - Study - Skills (Dragged)Document7 pagesIELTS FOUNDATION - Study - Skills (Dragged)Việt Anh VũNo ratings yet
- Mixed Lymphocyte Culture / Reaction (MLC / MLR)Document2 pagesMixed Lymphocyte Culture / Reaction (MLC / MLR)Muthi KhairunnisaNo ratings yet
- q1 Perdev StudentsDocument91 pagesq1 Perdev StudentsahyahxdxdNo ratings yet
- Jsa For RadiographyDocument3 pagesJsa For Radiographyjithin shankarNo ratings yet
- BTBT4 HK2 MoiDocument63 pagesBTBT4 HK2 MoiLa ZoramNo ratings yet
- Occlusal Onlay As Mordern RX PDFDocument13 pagesOcclusal Onlay As Mordern RX PDFSMART SMARNo ratings yet
- Effective Communication: Why Is It So Hard To Listen?Document3 pagesEffective Communication: Why Is It So Hard To Listen?Ariadne CulceNo ratings yet
- Why Scorebuilders PTDocument3 pagesWhy Scorebuilders PTSamarNo ratings yet
- MUCLecture 2022 32815285 PDFDocument15 pagesMUCLecture 2022 32815285 PDFobw 1408No ratings yet
- Transitional PlanDocument10 pagesTransitional PlanJorge Pereira PachecoNo ratings yet