You might also like
- Attrition MillsDocument8 pagesAttrition MillsKeerthy VenthenNo ratings yet
- Pharmaco Gnostic AlDocument3 pagesPharmaco Gnostic AldediraihanNo ratings yet
- A CFD-aided Experimental Study On Bending of Micro Glass PipettesDocument8 pagesA CFD-aided Experimental Study On Bending of Micro Glass PipettesKeerthy VenthenNo ratings yet
- Medicinal FunctionsDocument5 pagesMedicinal FunctionsKeerthy VenthenNo ratings yet
- 608 2616 1 PBDocument5 pages608 2616 1 PBKeerthy VenthenNo ratings yet
- Cycle Basic PhasesDocument5 pagesCycle Basic PhasesKeerthy VenthenNo ratings yet
- 1 Principles of BioenergeticsDocument5 pages1 Principles of BioenergeticsFatahany FadhilaNo ratings yet
- METICRANEDocument7 pagesMETICRANEKeerthy VenthenNo ratings yet
- Pra Formulas IDocument28 pagesPra Formulas IKeerthy VenthenNo ratings yet
- How Stress FormDocument5 pagesHow Stress FormKeerthy VenthenNo ratings yet
- VerapamilDocument5 pagesVerapamilKeerthy VenthenNo ratings yet
- Function of Protein in Immune SystemDocument8 pagesFunction of Protein in Immune SystemKeerthy VenthenNo ratings yet
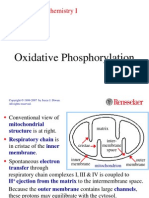
- 13 OxphosDocument47 pages13 OxphosMuhammad Fakhar AbbasNo ratings yet
- How Stress FormDocument5 pagesHow Stress FormKeerthy VenthenNo ratings yet
- How Stress FormDocument5 pagesHow Stress FormKeerthy VenthenNo ratings yet
- AlkaloidsDocument11 pagesAlkaloidsKeerthy VenthenNo ratings yet
- Essential Fatty Acids Makalah FinalDocument77 pagesEssential Fatty Acids Makalah FinalKeerthy VenthenNo ratings yet
- Verapamil HydrochlorideDocument13 pagesVerapamil HydrochlorideKeerthy VenthenNo ratings yet
- Verapamil HydrochlorideDocument13 pagesVerapamil HydrochlorideKeerthy VenthenNo ratings yet
- Binding Studies and Effect of Light On The Conductance of Intercalated Curcumin Into DNADocument8 pagesBinding Studies and Effect of Light On The Conductance of Intercalated Curcumin Into DNAKeerthy VenthenNo ratings yet
- Tugasan ToksikologiDocument12 pagesTugasan ToksikologiKeerthy VenthenNo ratings yet
- Notes CarbohydratesDocument21 pagesNotes CarbohydratesChris_Barber09100% (1)
- 53Document29 pages53Keerthy Venthen100% (1)
- Anions and CationsDocument10 pagesAnions and CationsKeerthy VenthenNo ratings yet
- Intermolecular ForceDocument1 pageIntermolecular ForceKeerthy VenthenNo ratings yet
- Acetaminophen Overview: Acetyl-Para-Aminophenol (APAP)Document17 pagesAcetaminophen Overview: Acetyl-Para-Aminophenol (APAP)Keerthy VenthenNo ratings yet
- 463-PHT Student NoteDocument28 pages463-PHT Student NoteKeerthy VenthenNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pediatric Nursing Process Worksheet: USF College of Nursing: NUR 4467LDocument4 pagesPediatric Nursing Process Worksheet: USF College of Nursing: NUR 4467Lapi-324566318No ratings yet
- Portable Toilet For Disaster Relief KinstedtDocument3 pagesPortable Toilet For Disaster Relief KinstedtMustafa HyaliNo ratings yet
- Rubella: Congenital Clinically Significant Congenital MalformationsDocument8 pagesRubella: Congenital Clinically Significant Congenital MalformationsAlexandraNo ratings yet
- NCP For Laryngeal CancerDocument5 pagesNCP For Laryngeal CancerMădălina PinciucNo ratings yet
- M1 Introduction To Manual TherapyDocument101 pagesM1 Introduction To Manual TherapySylvia LoongNo ratings yet
- Catalogue v09Document4 pagesCatalogue v09KRISHNA L BAISETTINo ratings yet
- Sleep Related Problems (GROUP 2)Document3 pagesSleep Related Problems (GROUP 2)april hortilanoNo ratings yet
- Doctor's OrdersDocument6 pagesDoctor's OrdersKryza Dale Bunado BaticanNo ratings yet
- Ajodo 1Document7 pagesAjodo 1ayis100% (1)
- Hamberger-Hastings1988 Article SkillsTrainingForTreatmentOfSpDocument10 pagesHamberger-Hastings1988 Article SkillsTrainingForTreatmentOfSpFer MuaNo ratings yet
- Labs and Impaired Tissue...Document40 pagesLabs and Impaired Tissue...Lea FestejoNo ratings yet
- Water Treatment Plant Residue Management ModificationDocument33 pagesWater Treatment Plant Residue Management ModificationNitisha Rathore50% (2)
- Nomenklatur IBS Edit THTDocument291 pagesNomenklatur IBS Edit THTriezki_pattikratonMDNo ratings yet
- 2 CP Bekam Angin Tahap 3Document8 pages2 CP Bekam Angin Tahap 3Norhissam MustafaNo ratings yet
- Cognitive MedsDocument2 pagesCognitive MedsRNStudent1100% (1)
- Post Traumatic Stress Disorder PTSD As An Over Activation of Sympathetic Nervous System An Alternative View 2167 1222.1000181Document3 pagesPost Traumatic Stress Disorder PTSD As An Over Activation of Sympathetic Nervous System An Alternative View 2167 1222.1000181Andi ANDIKANo ratings yet
- Imaging of The Genitourinary Tract: Mashuri, DR.,SP - Rad.,M.KesDocument90 pagesImaging of The Genitourinary Tract: Mashuri, DR.,SP - Rad.,M.KesmirzasullivanNo ratings yet
- Hypertension Management: Key RecommendationsDocument76 pagesHypertension Management: Key RecommendationsPritam DugarNo ratings yet
- A Long-Term Study of 370 Autotransplanted Premolars. Part II. Tooth Survival and Pulp Healing Subsequent To TransplantationDocument11 pagesA Long-Term Study of 370 Autotransplanted Premolars. Part II. Tooth Survival and Pulp Healing Subsequent To TransplantationRudnapon AmornlaksananonNo ratings yet
- Acute Necrotizing PancreatitisDocument37 pagesAcute Necrotizing PancreatitisVania SuSanchezNo ratings yet
- Interview Questions Band 5 PTDocument7 pagesInterview Questions Band 5 PTGeorge Noorland50% (2)
- The GcMAF BookDocument79 pagesThe GcMAF BookVíctor Valdez100% (1)
- Parasitology Lec 3.01a Intestinal NematodesDocument16 pagesParasitology Lec 3.01a Intestinal NematodesEnaWahahaNo ratings yet
- NCP 1Document4 pagesNCP 1Ke EjieNo ratings yet
- Borderline Personality DisorderDocument25 pagesBorderline Personality DisordersindhurajNo ratings yet
- Module 5 Cognitive Mental AssessmentDocument12 pagesModule 5 Cognitive Mental Assessmentlagathurc100% (2)
- Biodecoding Total BiologyDocument7 pagesBiodecoding Total Biologygrailfinder75% (4)
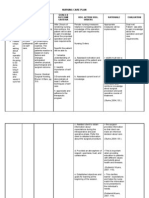
- Assessment Needs Nursing Diagnos IS Goal/Obj Ective Intervention Rationale EvaluationDocument10 pagesAssessment Needs Nursing Diagnos IS Goal/Obj Ective Intervention Rationale EvaluationApol Pen67% (3)
- Patient and Family Guide To The CANMAT and ISBD Guidelines On The Management of Bipolar DisorderDocument34 pagesPatient and Family Guide To The CANMAT and ISBD Guidelines On The Management of Bipolar DisorderLucila VialeNo ratings yet
- Mindfulness and Acceptance For Counseling College Students - Jacqueline Pistorello Ph.D.Document298 pagesMindfulness and Acceptance For Counseling College Students - Jacqueline Pistorello Ph.D.Vida Saludable100% (1)