You might also like
- Date and PlaceDocument1 pageDate and PlaceAndika GhifariNo ratings yet
- Ventricular Shunting ProceduresDocument22 pagesVentricular Shunting ProceduresAndika GhifariNo ratings yet
- TAB【Digimon Adventure Tri】-【Butterfly!】MusicGDocument3 pagesTAB【Digimon Adventure Tri】-【Butterfly!】MusicGAndika GhifariNo ratings yet
- Background, Objectives, and OutcomesDocument1 pageBackground, Objectives, and OutcomesAndika GhifariNo ratings yet
- LicenseDocument1 pageLicenseAndika GhifariNo ratings yet
- RefDocument1 pageRefAndika GhifariNo ratings yet
- Leptospirosis Pada Hewan Dan ManusiaDocument7 pagesLeptospirosis Pada Hewan Dan ManusiaAndika GhifariNo ratings yet
- Bebas Neue - SIL Open Font License 1.1Document4 pagesBebas Neue - SIL Open Font License 1.1SiswantoBudiNo ratings yet
- RefDocument1 pageRefAndika GhifariNo ratings yet
- Acl PDFDocument2 pagesAcl PDFAndika GhifariNo ratings yet
- Acl PDFDocument2 pagesAcl PDFAndika GhifariNo ratings yet
- EXP CoverSheetDocument3 pagesEXP CoverSheetAndika GhifariNo ratings yet
- Leptospirosis - Ferri's Clinical AdvisorDocument2 pagesLeptospirosis - Ferri's Clinical AdvisorAndika GhifariNo ratings yet
- Leptospirosis - Ferri's Clinical AdvisorDocument2 pagesLeptospirosis - Ferri's Clinical AdvisorAndika GhifariNo ratings yet
- LicenseDocument13 pagesLicensekarlaNo ratings yet
- Isokinetic Torque, Flexion/Extension Average Ratios in Power, and Nondisabled Adults and Adults With Mental RetardationDocument5 pagesIsokinetic Torque, Flexion/Extension Average Ratios in Power, and Nondisabled Adults and Adults With Mental RetardationAndika GhifariNo ratings yet
- 114 - Genetic Origins of Brain TumorsDocument10 pages114 - Genetic Origins of Brain TumorsAndika GhifariNo ratings yet
- Pediatric NeurologyDocument24 pagesPediatric NeurologyAndika GhifariNo ratings yet
- Dafpus Lama ReferatDocument2 pagesDafpus Lama ReferatAndika GhifariNo ratings yet
- AnnouncementDocument20 pagesAnnouncementAndika GhifariNo ratings yet
- Replikasi of DNADocument49 pagesReplikasi of DNAAndika Ghifari0% (1)
- Fever: Anca Ba Cârea, Alexandru SchiopuDocument24 pagesFever: Anca Ba Cârea, Alexandru SchiopuAndika GhifariNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
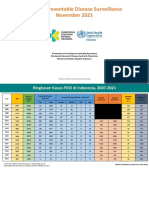
- 11 - VPD Surveillance Performance Analysis 2021 November 2021 (29122021)Document57 pages11 - VPD Surveillance Performance Analysis 2021 November 2021 (29122021)Kiky RizkyNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsSushilNo ratings yet
- Polio OutbreakDocument3 pagesPolio OutbreakAyn Jel MayNo ratings yet
- Vaccines and AntiserumsDocument2 pagesVaccines and AntiserumsAbdhan DjauhariNo ratings yet
- Are Vaccines Up For DebateDocument2 pagesAre Vaccines Up For DebateNiyah fairNo ratings yet
- AMOpportunities Certificate of ImmunizationDocument1 pageAMOpportunities Certificate of ImmunizationАида АрзуманянNo ratings yet
- Adult Combined Schedule BWDocument6 pagesAdult Combined Schedule BWalbatros4816No ratings yet
- Adult Combined ScheduleDocument13 pagesAdult Combined ScheduleJustin Ng SincoNo ratings yet
- Facts About Tetanus DeseaseDocument1 pageFacts About Tetanus DeseasechaariaNo ratings yet
- NGL - Covid-19 - ELA-Reading Lesson - WS - FPPDocument5 pagesNGL - Covid-19 - ELA-Reading Lesson - WS - FPPAhmed ElabbacyNo ratings yet
- AAEP Core Vaccinations For Adult HorsesDocument1 pageAAEP Core Vaccinations For Adult HorsesLauren ThompsonNo ratings yet
- Immunological ProductsDocument19 pagesImmunological ProductsPharma 24No ratings yet
- Jan. 13 Grand Forks Howell Vaccine ResponseDocument3 pagesJan. 13 Grand Forks Howell Vaccine ResponseJoe BowenNo ratings yet
- K - 12 Grade: California Immunization Requirements ForDocument2 pagesK - 12 Grade: California Immunization Requirements Forjulian14No ratings yet
- ImmunizationDocument10 pagesImmunizationHusseini ElghamryNo ratings yet
- Student Tracking SystemDocument2 pagesStudent Tracking SystemCynthia LuayNo ratings yet
- Vaccine Project - FinalDocument2 pagesVaccine Project - Finalchelsea garzaNo ratings yet
- NCP For ImmunizationsDocument2 pagesNCP For ImmunizationsJullienne Ysabelle AngNo ratings yet
- Polio PDFDocument10 pagesPolio PDFJohn Edward EscoteNo ratings yet
- COVID-19 - Landscape of Novel Coronavirus Candidate Vaccine Development WorldwideDocument13 pagesCOVID-19 - Landscape of Novel Coronavirus Candidate Vaccine Development WorldwideDeka AdeNo ratings yet
- Journal CubDocument33 pagesJournal CubHaritha K MuraleedharanNo ratings yet
- Grade School Parents Consent LetterDocument2 pagesGrade School Parents Consent LetterDario Basilio SaminNo ratings yet
- dm2022 0204Document8 pagesdm2022 0204Charlemagne Sabio GalamgamNo ratings yet
- PIIS1341321X19303721Document9 pagesPIIS1341321X19303721A AnonimyNo ratings yet
- Immunization Knowledge, Attitude and Practice Among Mothers of Children From 0 To 5 YearsDocument7 pagesImmunization Knowledge, Attitude and Practice Among Mothers of Children From 0 To 5 YearsUlil Amri Pramadani100% (1)
- Immunization HandbookDocument200 pagesImmunization Handbooktakumikuroda100% (1)
- FDA Briefing Document: Future Vaccination Regimens Addressing COVID-19Document25 pagesFDA Briefing Document: Future Vaccination Regimens Addressing COVID-19Jackson SinnenbergNo ratings yet
- Local Health Board Minutes6Document11 pagesLocal Health Board Minutes6JAMIL ASUMNo ratings yet
- Certificate PDFDocument1 pageCertificate PDFSanjay KudadaNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsNikhil shindeNo ratings yet