You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lesson Plan 5 Medicine LabelDocument35 pagesLesson Plan 5 Medicine Labelnta tiekaNo ratings yet
- Cns-Drugs-Ppt AdrianisusantyDocument84 pagesCns-Drugs-Ppt AdrianisusantyLydistri WuisndsriNo ratings yet
- Drug StudyDocument22 pagesDrug StudyDavid CalaloNo ratings yet
- Ginkgobiloba: Indications, Mechanisms, and SafetyDocument11 pagesGinkgobiloba: Indications, Mechanisms, and SafetyEmirgibraltarNo ratings yet
- 2018 Petersons ACT Prep Guide 3Document88 pages2018 Petersons ACT Prep Guide 3minwhanrieu100% (1)
- Ans 7Document3 pagesAns 7Raghvendra DhakadNo ratings yet
- Stroke PDFDocument67 pagesStroke PDFBadrul MunirNo ratings yet
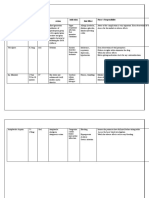
- Treatment For My Patient: Drug Dose Route Action Indication Side Effect Nurse's ResponsibilityDocument2 pagesTreatment For My Patient: Drug Dose Route Action Indication Side Effect Nurse's ResponsibilityValarmathiNo ratings yet
- J Jacc 2021 07 048Document13 pagesJ Jacc 2021 07 048Nicthe Ruiz RodríguezNo ratings yet
- Brief History of Heroin UseDocument24 pagesBrief History of Heroin UsedesmontesNo ratings yet
- Prostaglandins and LeukotrienesDocument40 pagesProstaglandins and LeukotrienesParul SinghNo ratings yet
- Pud Drug StudyDocument6 pagesPud Drug StudyLolcoma15 JaymsNo ratings yet
- Dəyər Sınaq 3 (2024)Document12 pagesDəyər Sınaq 3 (2024)nazimequliyeva2020No ratings yet
- Piroxicam: InjectionDocument2 pagesPiroxicam: Injectionintan purnamaNo ratings yet
- Katzungs Basic and Clinical Pharmacology 16th Edition Ebook PDFDocument89 pagesKatzungs Basic and Clinical Pharmacology 16th Edition Ebook PDFtheodore.maasch133No ratings yet
- In Komp A Tibi LitasDocument54 pagesIn Komp A Tibi LitasHifi Rizki.RNo ratings yet
- Antiplatelet and Thrombolytic DrugsDocument48 pagesAntiplatelet and Thrombolytic DrugsNofa PuspitaNo ratings yet
- Essential DrugsDocument352 pagesEssential DrugsEdwin WijayaNo ratings yet
- Listado Junio 9 Del 2021 Completo ActualizadoDocument17 pagesListado Junio 9 Del 2021 Completo ActualizadoVICTORIA PALACIOSNo ratings yet
- Effervescent PharmaceuticalsDocument13 pagesEffervescent PharmaceuticalsPuzhpop92% (12)
- Thrombotic Cardiovascular Events Associated With NSAID Use: Regulatory History and Results of Literature Search (RCTS)Document101 pagesThrombotic Cardiovascular Events Associated With NSAID Use: Regulatory History and Results of Literature Search (RCTS)abdurahman27No ratings yet
- February 19, 2016 Strathmore TimesDocument28 pagesFebruary 19, 2016 Strathmore TimesStrathmore TimesNo ratings yet
- Dispensing Lab ReviewerDocument4 pagesDispensing Lab ReviewerMikhail Agcaoili-CuanzonNo ratings yet
- Health.&.Nutrition May.2017 P2PDocument116 pagesHealth.&.Nutrition May.2017 P2PAbel BejanNo ratings yet
- SURGERY History and Counselling NotesDocument27 pagesSURGERY History and Counselling NotesaminaNo ratings yet
- Dispensing Lab 1 Activity 1 RX 1 2Document9 pagesDispensing Lab 1 Activity 1 RX 1 2Estella Marie SolarisNo ratings yet
- Drug StudyDocument33 pagesDrug Studyjefwy8No ratings yet
- Encyclopedia of Traditional Chinese Medicines Vol. 2Document558 pagesEncyclopedia of Traditional Chinese Medicines Vol. 2mihaela petre100% (4)
- Ibufen 600 Caplets: Summary of Product CharacteristicsDocument13 pagesIbufen 600 Caplets: Summary of Product Characteristicsddandan_2No ratings yet
- 207517Document11 pages207517angeljosechuquiureNo ratings yet