You might also like
- Adler - Individual PsychologyDocument51 pagesAdler - Individual PsychologySafira YulfaNo ratings yet
- Retinal DetachmentDocument8 pagesRetinal DetachmentJohanLazuardiNo ratings yet
- Iritis 8Document14 pagesIritis 8Alvis KurniawanNo ratings yet
- Elements of Exercise ProgramDocument4 pagesElements of Exercise ProgramMariam Gamos100% (1)
- Feline UveitesDocument9 pagesFeline UveitesErick ConfickeerzNo ratings yet
- Take One Nursing Final Coaching Ms CriticalDocument29 pagesTake One Nursing Final Coaching Ms Criticalnot your medz duranNo ratings yet
- Hemodialysis, Phosphorus and Calcium, Peritoneal DialysisDocument29 pagesHemodialysis, Phosphorus and Calcium, Peritoneal DialysisTrizha MaeNo ratings yet
- Medical Management of BlepharitisDocument6 pagesMedical Management of BlepharitisAl NaifNo ratings yet
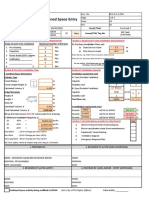
- Ventilation Plan For Confined Space EntryDocument9 pagesVentilation Plan For Confined Space EntryMohamad Nazmi Mohamad Rafian100% (1)
- A Case Study On The Improper Waste Disposal in General Santos CityDocument22 pagesA Case Study On The Improper Waste Disposal in General Santos CityJino Onij BolandoNo ratings yet
- Catalog Snibe Maglumi 800 English PDFDocument7 pagesCatalog Snibe Maglumi 800 English PDFAniket DubeyNo ratings yet
- Nursing Theory of Ramona T. Mercer MaterDocument8 pagesNursing Theory of Ramona T. Mercer MaterMark Norriel Cajandab100% (1)
- Thyroid Ophthalmopathy: Yash ShahDocument6 pagesThyroid Ophthalmopathy: Yash ShahCATALINMARCUNo ratings yet
- Nightingale Institute of Nursing: AssignmentDocument18 pagesNightingale Institute of Nursing: AssignmentDhAiRyA ArOrANo ratings yet
- Blepharitis - UpToDateDocument22 pagesBlepharitis - UpToDateanisa maria ulfaNo ratings yet
- Differential Diagnosis of The Swollen Red Eyelid - AAFPDocument16 pagesDifferential Diagnosis of The Swollen Red Eyelid - AAFPtorome4979No ratings yet
- Yanoff DukerDocument8 pagesYanoff DukerFerdinando BaehaNo ratings yet
- Approach To The Adult With Acute Persistent Visual LossDocument17 pagesApproach To The Adult With Acute Persistent Visual LossMauricio SvNo ratings yet
- How to take an eye exam historyDocument5 pagesHow to take an eye exam historyChris KingNo ratings yet
- Retinoblastoma PDFDocument5 pagesRetinoblastoma PDFRiska PermatasariNo ratings yet
- Blepharitis - UpToDateDocument38 pagesBlepharitis - UpToDatecamiloedaza1977No ratings yet
- New 5-FU option for epithelial downgrowthDocument4 pagesNew 5-FU option for epithelial downgrowthDelila MaharaniNo ratings yet
- Red Eye Clinical Presentation: History and Physical ExaminationDocument11 pagesRed Eye Clinical Presentation: History and Physical ExaminationLaiba KhanNo ratings yet
- 1-8 Eyelid DisordersDocument6 pages1-8 Eyelid Disorderssien99100% (1)
- OpthaDocument5 pagesOpthavarun2k6No ratings yet
- Uveitis GlaukomaDocument13 pagesUveitis GlaukomaDede FatmawatiNo ratings yet
- Referat Cystoid Macular Edema Periode 17 Juni - 20 Juli 2019Document25 pagesReferat Cystoid Macular Edema Periode 17 Juni - 20 Juli 2019CharlotteGraceNusiferaNo ratings yet
- Overlooked Complication ofDocument9 pagesOverlooked Complication ofdoctorbanNo ratings yet
- Chronic Closed Angle Glaucoma - StatPearls - NCBI BookshelfDocument6 pagesChronic Closed Angle Glaucoma - StatPearls - NCBI BookshelfAngel LimNo ratings yet
- Damage Control Surgery Ocular Traumatology (Injury)Document7 pagesDamage Control Surgery Ocular Traumatology (Injury)Shirakawa AlmiraNo ratings yet
- Review ArticleDocument10 pagesReview ArticleAnonymous Hic7yE7I8INo ratings yet
- Protrusion OjoDocument16 pagesProtrusion OjoAntonio ReaNo ratings yet
- Dry Eye Syndrome - StatPearls - NCBI Bookshelf PDFDocument7 pagesDry Eye Syndrome - StatPearls - NCBI Bookshelf PDFnum padNo ratings yet
- 1 SMDocument7 pages1 SMAriNo ratings yet
- Graves 508Document6 pagesGraves 508VellaNo ratings yet
- Keratoconus: Picture 1Document6 pagesKeratoconus: Picture 1BuiyiWongNo ratings yet
- Keratoconus: Picture 1Document6 pagesKeratoconus: Picture 1BuiyiWongNo ratings yet
- Silo - Tips - How To Take An Ophthalmic HistoryDocument5 pagesSilo - Tips - How To Take An Ophthalmic HistorySumon SarkarNo ratings yet
- Ptosis (Wiki)Document6 pagesPtosis (Wiki)lochnezNo ratings yet
- Corneal DystrophyDocument5 pagesCorneal DystrophyDejan JanevNo ratings yet
- Dry Eye Disease GuideDocument25 pagesDry Eye Disease Guide215045 zulfa laili aNo ratings yet
- Oftalmitis SimpatikaDocument12 pagesOftalmitis SimpatikaKarina HelsaNo ratings yet
- Treating Epithelial Downgrowth with 5-Fluorouracil InjectionsDocument5 pagesTreating Epithelial Downgrowth with 5-Fluorouracil Injectionsaghnia jolandaNo ratings yet
- Congenital Ptosis CaseDocument8 pagesCongenital Ptosis CaseHitesh Sharma67% (3)
- Equine Recurrent Uveitis: U.S.A.M.V. Cluj-Napoca Facultatea de Medicină Veterinară Disciplina: OftalmologieDocument9 pagesEquine Recurrent Uveitis: U.S.A.M.V. Cluj-Napoca Facultatea de Medicină Veterinară Disciplina: OftalmologiePatricia PopNo ratings yet
- Blowoutfractures PresentationDocument38 pagesBlowoutfractures PresentationVISHAKHANo ratings yet
- Fundoscopy Guide for OSCE ExamsDocument19 pagesFundoscopy Guide for OSCE ExamsMohamed Anas SayedNo ratings yet
- Congenital PtosisDocument15 pagesCongenital PtosisRobiniskandarNo ratings yet
- Ptosis (Eyelid) - WikipediaDocument26 pagesPtosis (Eyelid) - WikipediaRishabh ParakhNo ratings yet
- Seasonal Monthly Variation Amongst Reported Cataract Surgeries in IndiaDocument92 pagesSeasonal Monthly Variation Amongst Reported Cataract Surgeries in IndiafriendsofindiaNo ratings yet
- Exposure KeratopathyDocument12 pagesExposure KeratopathyFahyuniNo ratings yet
- Eye & ENTDocument12 pagesEye & ENTShandar SadafNo ratings yet
- Pan Uveitis (Causes and MGT of Sympathetic Ophthalmitis)Document21 pagesPan Uveitis (Causes and MGT of Sympathetic Ophthalmitis)Edoga Chima EmmanuelNo ratings yet
- MyopiaDocument11 pagesMyopiablueiceNo ratings yet
- Congenital Ptosis - GenetikaDocument28 pagesCongenital Ptosis - GenetikaJohanes Arie SetiawanNo ratings yet
- Internuclear OphthalmoplegiaDocument7 pagesInternuclear OphthalmoplegiaGrozaAlinaNo ratings yet
- Treatment of Blepharitis Recent Clinical TrialsDocument12 pagesTreatment of Blepharitis Recent Clinical TrialsSandra PeñuelaNo ratings yet
- MiddleEastAfrJOphthalmol19113-4844325 132723Document9 pagesMiddleEastAfrJOphthalmol19113-4844325 132723Vincent LivandyNo ratings yet
- The Association of Carotid Cavernous Fistula With Graves' Ophthalmopathy Brief CommunicationsDocument3 pagesThe Association of Carotid Cavernous Fistula With Graves' Ophthalmopathy Brief CommunicationsRiris SihotangNo ratings yet
- Primary vs. Secondary Angle Closure Glaucoma: DiseaseDocument1 pagePrimary vs. Secondary Angle Closure Glaucoma: Diseasefarah azizahNo ratings yet
- Blepharitis - UpToDateDocument37 pagesBlepharitis - UpToDateJorge Leonardo BedoyaNo ratings yet
- Diagnosis and Management of Pseudoexfoliation Glaucoma - American Academy of Ophthalmology PDFDocument7 pagesDiagnosis and Management of Pseudoexfoliation Glaucoma - American Academy of Ophthalmology PDFnoviaNo ratings yet
- Eye Trauma: Brief IntroductionDocument16 pagesEye Trauma: Brief IntroductionOchi D. GreenNo ratings yet
- MR 180 EditedDocument6 pagesMR 180 EditedfatmadianaNo ratings yet
- Miopi X Katarak 4Document5 pagesMiopi X Katarak 4Melati Nurul UtamiNo ratings yet
- Fundus Autofluorescence and Optical Coherence TomoDocument4 pagesFundus Autofluorescence and Optical Coherence TomoAndi Tiara S. AdamNo ratings yet
- Complications in UveitisFrom EverandComplications in UveitisFrancesco PichiNo ratings yet
- Skin Manifestations Associated With COVID-19: Current Knowledge and Future PerspectivesDocument12 pagesSkin Manifestations Associated With COVID-19: Current Knowledge and Future PerspectivesruditacitrahahaNo ratings yet
- Skin Manifestations Associated With COVID-19: Current Knowledge and Future PerspectivesDocument12 pagesSkin Manifestations Associated With COVID-19: Current Knowledge and Future PerspectivesruditacitrahahaNo ratings yet
- Bahan PanuveitisDocument28 pagesBahan PanuveitisruditacitrahahaNo ratings yet
- Daftar PustakaDocument1 pageDaftar PustakaruditacitrahahaNo ratings yet
- Peters AnomalyDocument7 pagesPeters AnomalyruditacitrahahaNo ratings yet
- TOEFLDocument3 pagesTOEFLruditacitrahahaNo ratings yet
- Jurnal1 PDFDocument6 pagesJurnal1 PDFruditacitrahahaNo ratings yet
- Ge 5 Lesson 5Document29 pagesGe 5 Lesson 5Lea MendarosNo ratings yet
- Daily Time Record Daily Time Record: Hazel Mae A. Monterde, RN Hazel Mae A. Monterde, RNDocument1 pageDaily Time Record Daily Time Record: Hazel Mae A. Monterde, RN Hazel Mae A. Monterde, RNTyler BertNo ratings yet
- MSC114 LessonsDocument54 pagesMSC114 Lessonsgrashew maanNo ratings yet
- Vasa Praevia RCOG GTGDocument13 pagesVasa Praevia RCOG GTGMariaBrincatNo ratings yet
- Obesity Obesity OverviewDocument6 pagesObesity Obesity OverviewLorena IbarrolaNo ratings yet
- Orthodontics & Dentofacial Orthopaedics: Page 1 of 24Document24 pagesOrthodontics & Dentofacial Orthopaedics: Page 1 of 24Abdul MohaiminNo ratings yet
- Taklimat Akademik Program MSC Counselling, MSW, MSC Correctional Science 6 September 2020 PDFDocument30 pagesTaklimat Akademik Program MSC Counselling, MSW, MSC Correctional Science 6 September 2020 PDFNCNNo ratings yet
- ANNEX DQAC Member List 29 OctDocument29 pagesANNEX DQAC Member List 29 OctSpace HR100% (1)
- Special Release 3 - Women and Men in Western Visayas PDFDocument8 pagesSpecial Release 3 - Women and Men in Western Visayas PDFJing PanganibanNo ratings yet
- Nevada CTE Recommended Equipment for Foods and Nutrition ProgramsDocument2 pagesNevada CTE Recommended Equipment for Foods and Nutrition Programsnithya nithyaNo ratings yet
- 1.principles of Business EthicsDocument7 pages1.principles of Business Ethicslegacy guptaNo ratings yet
- ® Whitening Fluoride Toothpaste: Product Overview Frequently Asked QuestionsDocument2 pages® Whitening Fluoride Toothpaste: Product Overview Frequently Asked QuestionsDina TrinidadNo ratings yet
- Preliminary Findings From RULER Approach in Spanish Teachers' Emotional Intelligence and Work EngagementDocument24 pagesPreliminary Findings From RULER Approach in Spanish Teachers' Emotional Intelligence and Work EngagementDaniela MendozaNo ratings yet
- Lisa Maley: Elementary School Teacher 4 Or5 GradeDocument2 pagesLisa Maley: Elementary School Teacher 4 Or5 Gradeapi-279892655No ratings yet
- IO ScriptDocument2 pagesIO ScriptShreya SagaonkarNo ratings yet
- 293 871 3 PBDocument7 pages293 871 3 PBDiana PertiwiNo ratings yet
- Inspection Checklist of Fishery Enterprises Handling Live FishDocument4 pagesInspection Checklist of Fishery Enterprises Handling Live FishBong PerezNo ratings yet
- Strength For Runners by Phily Bowden CoachingDocument7 pagesStrength For Runners by Phily Bowden CoachingKiranNo ratings yet
- Aug. 10, 2013Document10 pagesAug. 10, 2013The Delphos HeraldNo ratings yet
- ERROR DETECTION (New pattern) for Upcoming Mains ExamDocument31 pagesERROR DETECTION (New pattern) for Upcoming Mains Examishky manoharNo ratings yet
- AISD - Dental - Cigna - PPO & HMO Plan Information - 2019-2020Document1 pageAISD - Dental - Cigna - PPO & HMO Plan Information - 2019-2020Jordin TumlinsonNo ratings yet