Professional Documents
Culture Documents
RenalTubularAcidosis 000
Uploaded by
Titis Sekar Ningrum0 ratings0% found this document useful (0 votes)
14 views12 pageskesehatan
Original Title
RenalTubularAcidosis_000(1)
Copyright
© © All Rights Reserved
Available Formats
PDF, TXT or read online from Scribd
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this Documentkesehatan
Copyright:
© All Rights Reserved
Available Formats
Download as PDF, TXT or read online from Scribd
0 ratings0% found this document useful (0 votes)
14 views12 pagesRenalTubularAcidosis 000
Uploaded by
Titis Sekar Ningrumkesehatan
Copyright:
© All Rights Reserved
Available Formats
Download as PDF, TXT or read online from Scribd
You are on page 1of 12
http://cpj.sagepub.
com/
Clinical Pediatrics
http://cpj.sagepub.com/content/40/10/533
The online version of this article can be found at:
DOI: 10.1177/000992280104001001
2001 40: 533 CLIN PEDIATR
Karl S. Roth and James C. M. Chan
Renal Tubular Acidosis: A New Look at an Old Problem
Published by:
http://www.sagepublications.com
can be found at: Clinical Pediatrics Additional services and information for
http://cpj.sagepub.com/cgi/alerts Email Alerts:
http://cpj.sagepub.com/subscriptions Subscriptions:
http://www.sagepub.com/journalsReprints.nav Reprints:
http://www.sagepub.com/journalsPermissions.nav Permissions:
http://cpj.sagepub.com/content/40/10/533.refs.html Citations:
at MCMASTER UNIV LIBRARY on August 24, 2010 cpj.sagepub.com Downloaded from
Renal Tubular Acidosis: A NewLook
at an Old Problem
K arl S . Rot h , MD
J ames C . M. C h an, MD
S ummary: Alt h oug h t h e def init ion of renal t ubular acidosis ( RTA) is simp le, underst anding t h e
p h ysiolog ic basis underlying t h e v arious t yp es of t h is clinical ent it y is much more dif f icult . Th e
p at h op h ysiolog y of t h is disorder is rev iewed using t h e normal acid- base f unct ions of t h e inv olv ed
seg ment s of t h e nep h ron as a g uide t o underst anding . C linical and laborat ory f eat ures of t h e
subt yp es of RTA are addressed, and diag nosis and t reat ment discussed. Newdev elop ment s in t h e
knowledg e and underst anding of t h e associat ed g rowt h dist urbances, mineral met abolism, and mol-
ecular biolog y of RTA are also rev iewed t o p rov ide t h e most current v iewof t h is relat iv ely common
p ediat ric ent it y. C lin Pediat r. 2 0 0 1 ; 4 0 :5 3 3 - 5 4 3
I nt roduct ion
M aint enance of a normal
p H of body f luids is of
crit ical imp ort ance t o
v irt ually all cell p rocesses. Th e
abilit y of ch ang es in h ydrog en ion
concent rat ion t o af f ect t h e p h ysi-
cal conf ormat ion and t h us t h e bi-
olog ic f unct ion of p rot ein mole-
cules, is a f amiliar ex amp le of t h e
key role of p H. Moreov er, t h e h u-
man org anism p roduces subst an-
t ial q uant it ies of anions, such as,
sulf at e, p h osp h at e, and lact at e.
Th ese mat erials are collect iv ely
t ermed "unmeasured anions, "
and t h ey must be ex cret ed by t h e
kidney; accumulat ion of one or
more causes an increased p lasma
anion g ap ( [ Na+ ] - { [ C l- ] + [ HC O3 - ] D.
G enerally, such accumulat ion re-
sult s f rom increased p roduct ion
( e. g . , inborn errors of met abo-
lism) , so t h at absent such condi-
t ions most p at ient s wit h met abolic
acidosis h av e an anion g ap of less
t h an 1 6 . Alt h oug h t h e g ut makes a
sig nif icant cont ribut ion t o elec-
t rolyt e and f luid reabsorp t ion, it is
t h e renal t ubular ep it h elium t h at is
resp onsible f or def ense ag ainst ac-
cumulat ion of h ydrog en ion. Ac-
cording ly, wh en t h ere is clinical ev -
idence of met abolic acidosis wit h
no increase in t h e anion g ap , a
Dep art ment s of Pediat rics and B ioch emist ry & Molecular B iop h ysics, V irg inia C ommonwealt h
U niv ersit y, MC V C amp us, Rich mond, V irg inia.
Rep rint req uest s and corresp ondence t o: K arl S . Rot h , MD, MC V C amp us, P0 B ox 9 8 0 2 3 9 ,
Rich mond, V A 2 3 2 9 8 - 0 2 3 9 .
2 0 0 1 W est minst er Publicat ions, I nc. , 7 0 8 G len C ov e Av enue, G len Head, NY 1 1 5 4 5 , U . S . A.
search f or renal disease is a p riorit y.
* C linically, renal t ubular acido-
sis ( RTA) is ch aract eriz ed by a
normal anion g ap , h yp er-
ch loremic met abolic acidosis, and
associat ed f ailure t o t h riv e sec-
ondary t o g rowt h f ailure as well as
anorex ia. Polyuria and const ip a-
t ion can also be seen, alt h oug h
neit h er may be ap p arent in t h e
neonat al p eriod. Hyp erch loremic
met abolic acidosis in p ediat ric
p ract ice is most of t en associat ed
wit h diarrh eal disease. B ot h diar-
rh ea and RTA result in h y-
p okalemia; in a young inf ant wit h
diarrh ea and underlying RTA, t h e
t rue diag nosis may be obscured.
Th us, inordinat ely slowresolu-
t ion of h yp erch loremic met abolic
acidosis f ollowing diarrh eal dis-
ease sh ould sug g est t h e p ossibilit y
of an underlying p rimary RTA.
B eyond t h e dif f icult ies inh er-
ent in delineat ing RTA, RTA can
be subcat eg oriz ed int o dif f erent
disorders wit h dist inct ly dif f erent
p rog noses. Th e diag nost ic cat a-
O
OC TOB ER 2 0 0 1 C LI NI C ALPEDI ATRI C S 5 3 3
at MCMASTER UNIV LIBRARY on August 24, 2010 cpj.sagepub.com Downloaded from
Rot h , C h an
log uing of RTA is imp ort ant be-
cause of t h ese v aried out comes
and is based on t h e underlying
p at h op h ysiolog y. Th us, we beg in
wit h a rev iew of t h e normal
p rocesses f or renal h andling of an
acid load and p rog ress f rom t h is
t o a discussion of t h e p at h op h ysi-
olog y underlying t h e dif f erent
t yp es of RTA. F ollowing t h is, we
p rov ide an up dat ed rev iewof min-
eral met abolism in RTA and end
wit h a discussion of our current
underst anding of t h e molecular
biolog y of t h e disorder.
Ph ysiolog y and
Pat h op h ysiolog y
Prox imal Tubule
I n a f unct ional sense, t h e
nep h ron reg ulat es acid- base
h omeost asis by simult aneous
p rocesses of bicarbonat e reab-
sorp t ion and h ydrog en ion secre-
t ion. F or p urp oses of simp lif ica-
t ion we h av e ch osen t o rep resent
t h ese as base reabsorp t ion and acid
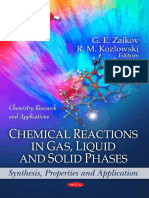
secret ion ( F ig ure 1 ) . C oncep t ually,
t h e p rox imal t ubule is ch arg ed
wit h t h e t ask of reclaiming f il-
t ered base
( - 8 5 %
of t h e t ot al) ;
f ailure of t h is p rocess leads t o re-
duct ion in syst emic base, result ing
in met abolic acidosis. I solat ed
p rox imal RTA of g enet ic orig in is
uncommon and is g enerally seen
in associat ion wit h ot h er asp ect s
of t ubular dysf unct ion. Th e nor-
mal p rocess of base salv ag e p ro-
ceeds in t h e p rox imal t ubule wit h -
out g enerat ion of a sig nif icant p H
g radient . Th e t h resh old f or bicar-
bonat e reabsorp t ion in neonat es
is reduced, desp it e an ev ent ual
normal adult reabsorp t iv e cap ac-
it y. " 2 Th e t h resh old is increased
g radually during mat urat ion,
wh ich is ref lect ed in increasing
serum bicarbonat e concent ra-
t ions wit h ag e. I n t h e normal
adult , t h e p rox imal t ubular sys-
H' , HC O- , Na' ,
HPO- 2 K 1
p H 7 . 4
Acid
( H+ )
NH_ secret on
Na4 + HC O 4 - H+ Dist al
Na+ + p C 0 7 3 4 0 { Ht J X
t ubule
p H 7 . 4 B ase
reabsorp t Don
Prox imal
t ubule
p H 7 . 4
F ig ure 1 . Th e nep h ron in base reabsorp t ion, acid secret ion and g enerat ion of an acid urine. B lood
at p H 7 . 4 ent ers t h e g lomerular cap illaries, wh ere t h e ionic const it uent s sh own are f ilt ered and en-
t er t h e p rox imal t ubular lumen, st ill at p H 7 . 4 . Th ere is a net reabsorp t ion in t h e p rox imal t ubule
of Na+ and HC 0 3 - wit h no ch ang e in luminal p H. U rine p assing t h roug h t h e lumen ex it s t h e loop
of Henle st ill at p H 7 . 4 and ent ers t h e dist al t ubule. Ag ain, as described in t h e t ex t , t h e g enerat ion
of ammonia and t h e net secret ion of H+ occur in t h is seg ment , wit h conseq uent elaborat ion of an
acidic urine in a p H rang e of 4 . 5 t o 8 . 0 . Th e dist al t ubule is able t o secret e h ydrog en ag ainst a g ra-
dient as h ig h as 1 0 0 0 :1 using an act iv e t ransp ort syst em.
t em result s in recov ery of > 6 0 0 0
mEq of bicarbonat e/ day. F ilt ered
sodium is act iv ely t ransp ort ed
across t h e luminal membrane us-
ing a Na+ - H+ carrier molecule
( NHE- 3 ) driv en by t h e concent ra-
t ion g radient f or sodium g ener-
at ed by Na+ - K + ATPase locat ed at
t h e ant iluminal surf ace of t h e cell
( F ig ure 2 ) . Th e ex p elled H+
rap idly associat es wit h f ilt ered lu-
minal bicarbonat e t o f orm
H2 C O3
( membrane- bound carbonic anh y-
drase, C A
MV ) ,
wh ich j ust as rap idly
dissociat es and liberat es C O2 and
wat er. Th e C O2 dif f uses int o t h e
cell, wh ere it is enz ymat ically ( car-
bonic anh ydrase, C A I I ) reh ydrat ed
t o f orm carbonic acid, wh ich
ag ain dissociat es wit h t h e f orma-
t ion of H+ and
HC O3 - . C A I I , or cy-
t osolic carbonic anh ydrase, is t h e
p redominant ( 9 5 % ) renal
isoz yme and is f ound in larg e p ro-
5 3 4 C LI NI C ALPEDI ATRI C S
OC TOB ER
2 0 0 1
5 3 4 C LI NI C ALPEDI ATRI C S OC TOB ER 2 0 0 1
at MCMASTER UNIV LIBRARY on August 24, 2010 cpj.sagepub.com Downloaded from
Renal Tubular Acidosis
0 Na+ -
HC O3 C ot ransp ort er
F ig ure 2 . Th e p rocess of p rox imal t ubular base reabsorp t ion. Th ere are t h ree key f eat ures of t h e
p rox imal t ubular ep it h elial cell t h at enable t h e abilit y t o reabsorb base: 1 ) act iv e t ransp ort of lu-
minal sodium as p art of t h e Na+ - K + ATPase syst em; 2 ) luminal surf ace and int racellular carbonic
anh ydrase cap able of p roducing larg e q uant it ies of bicarbonat e; 3 ) a sodium- bicarbonat e ex -
ch ang er ( NB C - 1 ) at t h e inner basolat eral surf ace. I t sh ould be not ed t h at alt h oug h bicarbonat e ap -
p ears t o be synt h esiz ed in order f or it s reabsorp t ion t o occur, t h ere is no net cont ribut ion of bi-
carbonat e made t o t h e amount orig inally f ilt ered; t h us, t h ere is net reabsorp t ion. U sed wit h
p ermission f rom C oh n RM, Rot h K S . B ioch emist ry and Disease: B ridg ing B asic S cience and C lin-
ical Medicine. B alt imore: W illiams & W ilkins; 1 9 9 6 .
p ort ion in t h e p rox imal t ubules. 3
B icarbonat e ex it s across t h e ant i-
luminal membrane f or t wo rea-
sons: 1 ) mass act ion, because t h e
bicarbonat e concent rat ion is
lower in t h e int erst it ial sp ace t h an
in t h e cyt osol; and 2 ) carrier- me-
diat ed cot ransp ort ( NB C - 1 ) along
an elect roch emical g radient , g en-
erat ed by ex p ulsion of t h e p osi-
t iv ely- ch arg ed Na+ cat ion int o t h is
sp ace by t h e ion p ump . W h ile t h e
economy of t h e syst em is mar-
v elous, t h e net result is sodium
and bicarbonat e reabsorp t ion but
no net eliminat ion of H+ .
A t radit ional v iewof p rox imal
renal t ubular acidosis h olds t h at
t h e t ubular max imum ( Tm) f or bi-
carbonat e is reduced, t h us lower-
ing t h e p lasma concent rat ion and
p ermit t ing a g reat er p rop ort ion
t h an normal of t h e f ilt ered HC O3 -
t o escap e int o t h e urine. At f irst
g lance, t h is is an adeq uat e ex p la-
nat ion f or t h e clinical observ a-
t ions; a closer lookleav es us wit h
t h e dif f icult y of ex p laining h ow
t h e t ubular max imum ( Tm) is
p h ysically lowered and wh y p a-
t ient s wit h t yp e 2 RTA of t en can
p roduce an acid urine. Modern
molecular biolog y h as h elp ed us
t o address t h e cent ral issue of re-
duct ion in t h e Tm.
C ont rary t o t h e nat ural t en-
dency t o conceiv e a reduced Tm as
imp airment of t ransp ort across
t h e brush border surf ace, t h e real
def ect is almost cert ainly locat ed
in t h e carrier f or Na+ - HC O3 - co-
t ransp ort across t h e ant iluminal
or basolat eral surf ace. Th is mole-
cule, NB C - 1 ( Na+ - bicarbonat e co-
t ransp ort er) , is a p rot ein consist -
ing of ap p rox imat ely 1 0 0 0 amino
acid residues and underg oes f unc-
t ional ch ang es wit h v arying p H
condit ions. 4 Human g ene cloning
ex p eriment s h av e rev ealed t h e ex -
ist ence of t h ree molecular iso-
f orms in kidney ( NB C - 1 , NB C - 2 ,
and NB C - 3 ) ; it is unclear at p re-
sent wh at t h e p recise f unct ional
dist inct ions are bet ween each of
t h e t h ree isof orms. 5 I t is also not
yet ap p arent wh et h er t h e cause( s)
f or t h e v arying clinical sev erit y of
t yp e 2 RTA can be at t ribut ed t o
mix ed h et eroz yg osit y of mut a-
t ions in t h ese t h ree isof orms be-
cause of limit ed access t o t issue
f or st udy. Nonet h eless, it ap p ears
t h at t h e mech anism underlying
t h e reduced t ubular max imum
f or bicarbonat e is act ually re-
duced t ransp ort out of t h e p rox i-
mal t ubular cell wit h increased
backf low( ef f lux ) of cyt osolic bi-
carbonat e int o t h e t ubular lumen.
Th e inabilit y of t h e p rox imal
t ubule t o ach iev e net h ydrog en
ion eliminat ion renders t h e bicar-
bonat e buf f er syst em v ulnerable
t o an imp airment in t h e p rocess
of bicarbonat e reclamat ion. I n
such circumst ances, t h e result is a
non- anion g ap met abolic acido-
sis. Th is is because t h e body' s
met abolic p rocesses g enerat e
nonv olat ile, or f ix ed acids, wh ich
must be buf f ered by t h e blood
and eliminat ed t h roug h t h e kid-
neys. Th e laws of elect rical neu-
t ralit y also demand t h at each
mole of bicarbonat e t h at is lost be
accomp anied by a mole of cat ion,
usually p ot assium and, t o a lesser
ex t ent , sodium. Th e sodium loss
p rov okes a blood v olume cont rac-
t ion and a secondary release of al-
OC TOB ER 2 0 0 1
C LI NI C ALPEDI ATRI C S 5 3 5
LU MEN
PROXI MAL TU B U LE
C ELL B LOOD
Na*
* C arbonic Anh ydrase
OC TOB ER 2 0 0 1 C LI NI C ALPEDI ATRI C S 5 3 5
at MCMASTER UNIV LIBRARY on August 24, 2010 cpj.sagepub.com Downloaded from
Rot h , C h an
dost erone, wh ich ex acerbat es t h e
urinary p ot assium loss and cre-
at es a sig nif icant h yp okalemia, al-
t h oug h t h is is g enerally mild and
does not req uire t reat ment . Th ese
are t h e p h enomena underlying
t h e clinical ent it y t ermed p rox i-
mal or t yp e 2 RTA, def ined as a sys-
t emic acidosis deriv ing f rom a rel-
at iv e decrease in t h e abilit y of t h e
t ubule t o reclaim base.
F inally, wh ile bicarbonat uria
may be ex p ect ed t o p roduce alka-
line urine, t h is is not necessarily
t h e case in clinical p ract ice. Al-
t h oug h t h e abilit y of t h e p rox imal
t ubule t o reclaim base is imp aired
in p rox imal RTA, t h e abilit y of t h e
nep h ron t o eliminat e H+ remains
unaf f ect ed. Th us, p at ient s wit h
t yp e 2 RTA and syst emic acidosis
may p roduce urine wit h an acid
p H, rendering urine p H alone an
inaccurat e diag nost ic t est f or dis-
t inct ion bet ween t yp es I and I I
RTA. S ince t h e bicarbonat e
t h resh old increases wit h ag e, t h e
relat iv e reduct ion in bicarbonat e
Tm in t h e neonat e of t en con-
t ribut es t o a p ict ure of h yp er-
ch loremic met abolic acidosis and
acid urine p H, wh ich disap p ears
as t h e inf ant dev elop s. Not wit h -
st anding it s disap p earance, h ow-
ev er, t h is sit uat ion may req uire al-
kali t h erap y in early lif e t o av oid
anorex ia and p ermit normal
g rowt h .
Dist al Tubule
As not ed, base reabsorp t ion is
h andled p rimarily in t h e p rox i-
mal t ubule, wh ich is p h ysiolog i-
cally uneq uip p ed t o f orm a h y-
drog en ion g radient bet ween t h e
blood and t h e t ubular lumen wit h
wh ich t o reg ulat e blood p H. Th is
t ask f alls t o t h e dist al t ubule,
wh ere h ydrog en ion is secret ed
wit h t h e g enerat ion of a st eep H+
g radient . Th us, t h e role of t h e dis-
t al t ubule in acid- base h omeost a-
sis may be concep t ualiz ed as one
of acid secret ion, in cont rast t o
t h e p rox imal t ubule, wh ich serv es
as a
maj or
sit e f or reabsorp t ion of
base. I t is t h is dif f erence in roles
t h at also account s f or t h e dif f er-
ences in clinical sev erit y bet ween
dist urbances of p rox imal and dis-
t al t ubular f unct ions. Hence, al-
t h oug h increased loss of base
f rom t h e p rox imal t ubule causes
dev elop ment of a syst emic acido-
sis, t h e deg ree of t h e acidosis is
mit ig at ed considerably by t h e
abilit y of t h e dist al t ubule t o elim-
inat e h ydrog en ion. I n cont rast ,
h owev er, wh en t h e dist al t ubule is
not cap able of normal H+ elimi-
nat ion, t h ere is a maj or acid- base
diseq uilibrium result ing in sev ere
acidosis.
Th e key t o t h e abilit y of t h e
dist al t ubule t o cause net acid se-
cret ion is t h e cap acit y t o direct ly
secret e H+ int o t h e t ubular lumen
indep endent of sodium, using a
H+ - ATPase p ump . 6 Ot h er f eat ures
dist inct t o t h e dist al t ubule in-
clude t h e f ollowing : nonleaky
t ig h t j unct ions p ermit t ing g enera-
t ion of v ery st eep concent rat ion
g radient s, and t h e g enerat ion of
ammonia ( F ig ure 3 ) . I t is imp or-
t ant t o underst and t h at t h e h ydro-
g en ion t h at is ex p elled is g ener-
at ed by t h e act ion of carbonic
anh ydrase on wat er and C 0 2 , so
t h at t h e remaining HC 0 3 - can be
ex ch ang ed at t h e basal surf ace f or
a ch loride ion. Th e def icit lef t by
ex p ulsion of t h e h ydrog en ion is
addressed by dif f usion of a
sodium ion, wh ich ex it s wit h t h e
bicarbonat e in ex ch ang e f or a K + .
Th e simult aneous p roduct ion of
NH3 f rom g lut amine and it s dif f u-
sion int o t h e lumen cap t ures t h e
h ydrog en ion by f ormat ion of am-
monium radical and combinat ion
wit h f ilt ered p h osp h at e. I t is t h e
f ormat ion of t h ese acid salt s t h at
comp rises t it rat able acid and ren-
ders t h e abilit y of t h e dist al t ubule
t o p roduce an acid urine.
Remarkably, t h ere is a direct
similarit y bet ween t h e molecular
def ect s in p rox imal and dist al
RTA. As in t yp e 2 RTA, t h e def ect
in t yp e 1 RTA lies not in t h e
brush border H+ - ATPase, wh ich
mig h t be an int uit iv e assump t ion,
but rat h er in t h e C l- - HC 0 3 - ex -
ch ang er at t h e ant iluminal sur-
f ace7 ( see F ig ure 3 ) . Th is h as been
def init iv ely demonst rat ed in
t h ose indiv iduals sh owing an au-
t osomal dominant t ransmission
p at t ern, 8 but is less clear in t h ose
wit h t h e aut osomal recessiv e v ari-
et y, in wh ich some p at ient s are
t h oug h t t o h av e a def ect in t h e
brush border H+ - ATPase. 9 Th e
f ailure of ch loride- bicarbonat e
ex ch ang e leads t o accumulat ion
of int racellular carbonic acid t h at
imp edes f urt h er synt h esis as well
as dissociat ion int o h ydrog en ion
and bicarbonat e. S odium- p ot as-
sium ex ch ang e will be adv ersely
af f ect ed as well, since sodium nor-
mally ex it s int o t h e p ericap illary
sp ace along wit h bicarbonat e.
S ince less h ydrog en ion is f ormed
by dissociat ion, t h ere is less ex -
p elled int o t h e lumen t o f orm
acid salt s and t h e urine p H t ends
t oward t h e neut ral rang e.
As in p rox imal RTA, t h e di-
minish ed sodium reabsorp t ion
causes a v olume cont ract ion, re-
duced body sodium, and a sec-
ondary h yp eraldost eronism. Th e
result ing p ot assium loss leads t o
h yp okalemia, of t en of a rat h er se-
v ere deg ree. Howev er, t h ere is a
div erg ent resp onse of t h e h y-
p okalemia t o t h erap y bet ween t h e
t wo f orms of RTA; wit h v olume
and p H correct ion t h ere is a de-
crease in aldost erone and a cor-
rect ion of p ot assium wast ing in
dist al RTA. B y cont rast , in p rox i-
mal RTA t h e p ot assium wast ing
increases wit h v olume correct ion,
because t h ere is increased deliv -
ery of sodium bicarbonat e t o t h e
dist al t ubule, wh ich is ch arg ed
5 3 6 C LI NI C ALPEDI ATRI C S
OC TOB ER 2 0 0 1
5 3 6 C LI NI C ALPEDI ATRI C S OC TOB ER 2 0 0 1
at MCMASTER UNIV LIBRARY on August 24, 2010 cpj.sagepub.com Downloaded from
Renal Tubular Acidosis
DI S TAL TU B U LE
C ELL B LOOD
= C arbonic Anh ydrase ONa' - K + - ATPase
0 C h loride- B icarbonat e Ex ch ang er
F ig ure 3 . Th e p rocess of net H+ ex cret ion in t h e dist al t ubule. Th ere are f our key f eat ures of t h e
dist al t ubule t h at cont ribut e t o t h e acidif icat ion of t h e urine: 1 ) a brush border H+ ATPase; 2 ) int ra-
cellular carbonic anh ydrase; 3 ) a basolat eral C l- - HC O3 - ex ch ang er; 4 ) abilit y t o synt h esiz e NH3 .
Det ails are cont ained in t h e t ex t . Modif ied and used wit h p ermission f rom C oh n RM, Rot h K S . B io-
ch emist ry and Disease: B ridg ing B asic S cience and C linical Medicine. B alt imore: W illiams &
W ilkins, 1 9 9 6 .
wit h sodium- p ot assium ex ch ang e.
A rev iewof t h is discussion nowal-
lows ex p lanat ion f or t h e clinical
f inding s of p olyuria and const ip a-
t ion in af f ect ed p at ient s. Th e re-
duct ion in v olume causes up reg u-
lat ion of t h e renin- ang iot ensin
syst em; increased ang iot ensin I I
h as a direct ef f ect on t h e t h irst
cent er in t h e brain, 1 0 wh ile de-
creased int erst it ial p ot assium and
decreased ch loride ex ch ang e di-
minish es concent rat ing abilit y in
t h e renal loop of Henle wit h t h e
t wo p h enomena combining t o
cause p olyuria. Th e const ip at ion
is a direct conseq uence of h y-
p okalemia, wit h conseq uent de-
crease in g ut mot ilit y.
A f inal p at h og enic issue in
bot h f orms of RTA is t h at of cal-
cium- p h osp h orus met abolism
and secondary ef f ect s on t h e kid-
ney. C ommon t o bot h p rox imal
and dist al RTA is a st at e of ch ronic
met abolic acidosis, req uiring t h at
H+ be bot h buf f ered and ex cret ed
by alt ernat iv e means. Th e most di-
rect ef f ect of acidosis is t h e dis-
p lacement of p rot ein- bound cal-
cium by h ydrog en in t h e blood,
t h ereby increasing bot h t h e
amount of ioniz ed calciumll, "2
and it s f ilt rat ion by t h e g lomeru-
lus. Howev er, ch ronic acidosis
p rov okes div erg ent resp onses t o
t h is increased calcium load in t h e
p rox imal and dist al seg ment s, in-
creasing reabsorp t ion in t h e f or-
mer and inh ibit ing it in t h e lat t er.
Th e net ef f ect is t o cause h yp er-
calciuria, wh ich can reach st riking
p rop ort ions in t h e dist al RTA
f orm but usually remains of no
conseq uence in isolat ed t yp e 2
disease. Typ e 1 RTA is due t o f ail-
ure t o eliminat e h ydrog en ion,
wh ile t yp e 2 is a conseq uence of
diminish ed base reabsorp t ion;
t h us, t h e marked dif f erence in de-
g ree of syst emic acidosis may also
p lay a role.
Th e sev ere acidosis of t yp e 1
disease also inh ibit s p roduct ion
and release of mit och ondrial cit -
rat e, 1 3 wh ich is normally p resent
t o react wit h calcium and en-
h ance it s solubilit y.
1 4
I ncreased
f ilt ered load and inh ibit ed reab-
sorp t ion causes sev ere h yp er-
calciuria, wh ile t h e reduct ion in
solubilit y leads t o a marked t en-
dency t oward nep h rocalcinosis.
Moreov er, t h e need t o maint ain
serum calcium necessit at es in-
creased t urnov er of bone mat rix
and result s in ost eomalacia. I n
cont rast , bone disease in t yp e 2
RTA is relat iv ely mild, g enerally
result ing f rom p h osp h at e loss and
secondary h yp erp arat h yroidism.
Ph osp h at e, a maj or urinary
buf f er, is f ilt ered by t h e g lomeru-
lus and ent ers t h e p rox imal t ubu-
lar lumen wh ere it becomes av ail-
able t o buf f er h ydrog en ions.
Howev er, ammoniag enesis is sub-
max imal in ch ronic acidosis,
wh ich rest rict s t h e usef ulness of
NH3 as a urinary buf f er, esp ecially
in an alkaline urine such as t h at
p roduced in t yp e
1 RTA. I n addi-
t ion, t h is reduced synt h et ic rat e
limit s cat ions req uired f or f ix ed
acid ex cret ion and oblig at es
ot h er cat ions, such as C a+ + , t o act
in it s p lace.
Rat e- Dep endent Dist al RTA
C ondit ions t h at alt er t ransep -
it h elial v olt ag e in t h e dist al seg -
OC TOB ER 2 0 0 1
C LI NI C ALPEDI ATRI C S 5 3 7
LU MEN
C LI NI C ALPEDI ATRI C S 5 3 7
OC TOB ER 2 0 0 1
at MCMASTER UNIV LIBRARY on August 24, 2010 cpj.sagepub.com Downloaded from
Rot h , C h an
ment , such as imp aired sodium
up t ake, can also alt er t h e rat e at
wh ich H+ is secret ed int o t h e lu-
men, and are et iolog ically dist inct
f rom t h e g enet ically t ransmit t ed
disorder already discussed. S t rif e
and associat esl5 h av e demon-
st rat ed in ch ildren wit h dist al RTA
t h at dif f erent iat ion of t h e classical
disease f rom rat e- dep endent dis-
t al RTA on clinical g rounds will be
dif f icult . I n rat e- dep endent dist al
RTA t h e kidney can elaborat e
urine wit h a p H less t h an 4 . 5 , lead-
ing t o misdiag nosis of p rox imal
RTA. Det erminat ion of t h e dif f er-
ence bet ween urine and blood
p art ial p ressure of C O2 will aid in
dif f erent iat ion, since all p at ient s
wit h dist al RTA will h av e a dif f er-
ence of less t h an 2 0 mmHg , wh ile
normal subj ect s and ch ildren wit h
p rox imal RTA will h av e a dif f er-
ence g reat er t h an 2 0 mmHg . 1 5
Diag nost ic Ap p roach
I dent if icat ion and ap p rop ri-
at e cat eg oriz at ion of p at ient s wit h
RTA req uire considerat ion of an
ex t ensiv e list of dif f erent ial diag -
noses ( F ig ure 4 ) . Th e init ial t askis
t o det ermine t h e p resence of a h y-
p erch loremic met abolic acidosis
and absence of any sig nif icant
p lasma anion g ap ( [ sodium]
-
[ bicarbonat e] + [ ch loride] ) . Th e
dif f erent ial list of ent it ies f it t ing
t h is descrip t ion is p resent ed in
Table 1 .
Th e most common cause of
t h is sit uat ion in p ediat rics is acut e
diarrh eal disease. Pot assium
losses can be subst ant ial enoug h
in eit h er RTA or diarrh eal disease
t o cause h yp okalemia, making t h e
t wo dif f icult t o dist ing uish f rom
each ot h er wh en t h ey coex ist in
t h e inf ant . Th e most direct means
t o ap p roach a dif f erent ial in sus-
p ect ed RTA is by det erminat ion
of t h e urinary anion g ap , def ined
Met abolic Acidosis
Ev aluat e S erum Anion G ap
Elev at ed Normal ( 1 0 - 1 2 meq / 1 )
W orkup f or
h ig h anion
g ap acidosis
Ev aluat e U rinary Anion G ap
Normal ( small t o neg at iv e)
R/ OTyp e I I RTA
Ev aluat e
U rine p H
S erum K +
F ract ional Ex cret ion HC OJ
Elev at ed ( p osit iv e)
S erum K +
Low Hig h
R/ OTyp e I RTA R/ OTyp e I V RTA
Ev aluat e Ev aluat e
U rine p H U rine p H
U rine:
B lood
p C O2
U ine: B lood
PC O2
F ig ure 4 . Alg orit h m f or diag nosis of RTA. F rom Hanna J D, S ant os F , C h an J C M. Renal t ubular aci-
dosis. I n K h er K K , Makker S P ( eds) : Pediat ric Renal Disease: Diag nosis and Manag ement . New
York: McG raw- Hill, 1 9 9 2 , p p . 6 6 5 - 6 6 8 .
somewh at dif f erent ly f rom t h e
serum anion g ap , as t h e sum of
( urine [ Na+ ] + urine [ K + ] )
-
urine
[ C 1 - ] . Ammonium ex cret ion is
usually increased as acidosis de-
v elop s, most commonly in t h e
f orm of ch loride salt s, alt h oug h
urinary ammonium is considered
an unmeasured cat ion. Th us, in a
st at e of acidosis, t h e urinary an-
ion g ap sh ould decrease as t h e
ch loride ex cret ion increases in
concert wit h ammonium. Th e
ut ilit y of t h is calculat ion ref lect s
t h e f act t h at ammonium g enera-
t ion by t h e kidney occurs in t h e
dist al t ubule, so t h at in all f orms
of dist al RTA it would be ant ici-
p at ed t h at no decrease in urine
anion g ap would be seen. I n con-
t rast , a normal renal resp onse t o
g ast roint est inal bicarbonat e
losses, or in a kidney af f ect ed by
Typ e I I RTA, would be increased
ammonium p roduct ion, in-
creased ch loride ex cret ion, and
h ence, a decreased v alue of t h e
urinary anion g ap .
5 3 8 C LI NI C AL PEDI ATRI C S
2 0 0 1 ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
OC TOB ER 2 0 0 1 5 3 8 C LI NI C ALPEDI ATRI C S
at MCMASTER UNIV LIBRARY on August 24, 2010 cpj.sagepub.com Downloaded from
Renal Tubular Acidosis
Ex amp les
Normal Typ e I RTA Typ e I I RTA
C l > Na+ K + C lV > Na+ K + C lV > Na+ K +
1 0 0 + 5 - 1 5 0 - 4 5 1 0 0 + 5 - 1 5 0 - 4 5 1 0 0 + 5 - 2 0 0 - - 9 5
Th e use of t h is p aramet er in
ch ildren h as been discussed; 1 6 it is
adv isable t o use caut ion in int er-
p ret ing t h e uirine anion g ap in
ch ildren, and esp ecially in
neonat es since ammonium g ener-
at ion mat ures during p ost nat al
dev elop ment .
I n ch ildren wit h a relat iv ely
mild deg ree of syst emic acidosis
( a serum bicarbonat e concent ra-
t ion no lower t h an 1 7 mEq / L) , it
may be h elp f ul t o p erf orm an
acid- loading t est . Th e classical
met h od f or t h is h as been an oral
load of NH4 C l; recent ly, t h e int ra-
v enous arg inine h ydroch loride
inf usion t est ( 1 0 0 - 1 5 0 mEq
H+ / m2 body surf ace area) h as
been used. ' 7 Th e ov erall p urp ose
of t h ese t est s is t o creat e syst emic
condit ions t h at will max imiz e re-
nal h ydrog en ion ex cret ion, and
t o det ermine syst emic and urine
p H under t h ese circumst ances. I f
urine p H f alls below5 . 5 , t h e p a-
t ient can be assumed not t o h av e
dist al RTA. S ome p at ient s wit h
p rox imal RTA can ach iev e a nor-
mal urine p H resp onse under
t h ese circumst ances, so t h at t yp e
I I RTA cannot be ruled out by t h is
t ech niq ue.
Anot h er t est of t h e abilit y of
t h e dist al t ubule t o secret e H+ is t o
alkaliniz e t h e urine and measure
t h e secret ory cap acit y along a h y-
drog en ion g radient wh ere blood
p H sh ould be less t h an urine p H.
C lassically t h is was ach iev ed using
an oral sodium bicarbonat e dose,
but oral acet az olamide as a uri-
nary alkaliniz ing ag ent ( 1 7
mg / K g ) h as been f ound t o be
more ef f icient . 1 8 Dist ally secret ed
h ydrog en ions ent er t h e t ubular
lumen and combine wit h bicar-
bonat e anions t o f orm carbonic
acid, wh ich slowly deh ydrat es int o
wat er and C O2 because of t h e ab-
sence of luminal membrane car-
bonic anh ydrase in dist al t ubular
cells. Accumulat ion of luminal
C O2 because of delayed deh ydra-
t ion of carbonic acid is f urt h er en-
h anced by diminish ed dif f usion
due t o an unf av orable v olume t o
surf ace area relat ionsh ip in t h e
medullary collect ing duct . ' 7 As a
result of t h ese t wo f act ors, t h e
p C O2 of t h e urine increases and,
measured in suf f icient ly alkaline
urine, it can be used as a reliable
index of dist al h ydrog en ion se-
cret ion. U nder t h ese condit ions,
normal indiv iduals are cap able of
increasing urine p C O2 abov e 7 0
mmHg and ach iev ing a p C O2 dif -
f erence bet ween urine and blood
of 2 5 t o 3 0 mm Hg . G iv en t h e
same condit ions, a dif f erence of
less t h an 2 0 mmHg st rong ly sug -
g est s diminish ed H+ secret ory ca-
p acit y, wh ich is ch aract erist ic of
dist al RTA.
Normal indiv iduals g iv en
f urosemide ( 1 - 2 mg / kg ) g ener-
at e a markedly acid urine and a
sig nif icant increase in net acid ex -
cret ion wit h in 2 t o 3 h ours. Th is
ef f ect is based on f urosemide- in-
duced increased sodium deliv ery
t o and inh ibit ion of ch loride re-
absorp t ion in t h e dist al t ubule. As
a conseq uence, t h e increased
sodium load result s in g reat er ex -
ch ang e f or H+ and t h e g reat er
p resence of ch loride induces a
C LI NI C ALPEDI ATRI C S 5 3 9 OC TOB ER 2 0 0 1
at MCMASTER UNIV LIBRARY on August 24, 2010 cpj.sagepub.com Downloaded from
Rot h , C h an
h ig h er deg ree of luminal elec-
t roneg at iv it y. Th us, p at ient s wit h
RTA sh ould sh owconcordant re-
sp onses t o a f urosemide t est . I n
p at ient s susp ect ed of h av ing t yp e
4 RTA in wh om h yp erkalemia
could become h az ardous wit h
acid loading , f urosemide can p ro-
v ide a usef ul and saf e alt ernat iv e.
G rowt h F ailure in RTA
Dist urbances of g rowt h are
t yp ically associat ed wit h RTA of all
t yp es and wit h ch ronic met abolic
acidosis in g eneral. Th e ef f ect s of
acidosis ap p ear t o f all int o t wo
sep arat e cat eg ories: direct ( by
commit t ing calcium as a buf f er
f or H+ ) and indirect ( t h roug h t h e
g rowt h h ormone- I G F ax is) . I n t h e
classical v iew, t h e p at h op h ysio-
log ic resp onse t o ch ronic acidosis
leads t o increase in t h e ioniz ed
f ract ion in serum, a result ant in-
crease in g lomerular f ilt rat ion
and a conseq uent enh anced uri-
nary loss as calcium salt s. Th e net
result of t h is is ost eomalacia wit h
bowing of t h e long bones, p art ic-
ularly t h ose in t h e lower ex t remi-
t ies, and g rowt h f ailure. W e h av e
already ex amined t h e t ubular
p rocesses leading t o t h ese ef f ect s,
so t h at t h is mech anism f or t h e ad-
v erse imp act of acidosis up on
g rowt h sh ould be clear.
I n 1 9 8 1 , McS h erry and associ-
at es1 9 rep ort ed a blunt ed g rowt h
h ormone release in ch ildren wit h
RTA, alt h oug h no dat a were in-
cluded on f req uency, q uant it y, or
ot h er asp ect s of g rowt h h ormone
secret ion. To up dat e t h is rep ort ,
C h alla and co- workers2 0 recent ly
demonst rat ed t h at p ulse amp li-
t ude and area, as well as t ot al
g rowt h h ormone secret ion were
diminish ed in acidot ic rat s, com-
p ared t o cont rol and p air- f ed ani-
mals, wh ile t h e p ulse f req uency
remained unaf f ect ed in t h e aci-
dot ic animals. Ot h er f inding s in-
cluded sup p ressed serum I G F , h e-
p at ic I G F - 1 mRNA and h ep at ic
g rowt h h ormone recep t or
mRNA, as well as g ene ex p ression
of I G F at t h e g rowt h p lat e of t h e
long bones in t h ese animals. Th e
ch ang es in I G F - 1 mRNA and
g rowt h h ormone recep t ors seem
t o be sp ecif ic t o t h e cellular ef f ect s
of acidosis. Taken t og et h er, t h ese
f inding s are rep resent at iv e of an
addit ional mech anism f or t h e ad-
v erse imp act of ch ronic acidosis
up on g rowt h , alt h oug h t h ey will
need conf irmat ion in h umans.
G enet ics and
Molecular G enet ics
U nt il recent ly, elucidat ion of
t h e g enet ic asp ect s of t yp es 1 and
2 RTA was h amp ered by conf us-
ing clinical associat ions ( e. g . ,
deaf ness, F anconi syndrome) and
f amilial, inh erit ed, and sp oradic
p at t erns of occurrence f or each .
Howev er, wit h t h e adv ent of mole-
cular g enet ics, many of t h e p rev i-
ously p uz z ling asp ect s of t h ese dis-
orders are nowcoming int o
sh arp er f ocus. Th e t ransient ,
neonat al f orm of RTA may be
caused by relat iv e immat urit y of
t h e ap ical Na+ - H+ ex ch ang er mol-
ecule ( NHE- 3 ) , wh ich is known t o
underg o p ost nat al dev elop ment
in animals. 2 1 , 2 2 Th e g ene f or
NHE- 3 h as been map p ed t o
5 p l5 . 3 . 2 3 W it h resp ect t o g enet ic
t yp e 2 RTA, t h e molecular basis
f or an inh erit ed def ect is nowin
h and wit h t h e cloning of t h e t wo
h uman g enes f or t h e Na+ - HC O3 -
cot ransp ort er ( NB C ) p rot ein
molecules. Th e g ene f or NB C - 1
h as been map p ed t o 4 p 2 I . 2 4 How-
ev er, it may req uire dev elop ment
of diag nost ic t ech nolog y t o ascer-
t ain t h e p resence of an abnormal
NB C - 1 t ransp ort er g ene in non-
renal t issue f rom af f ect ed indiv id-
uals, since renal biop sy in t yp e 2
RTA is dif f icult t o rat ionaliz e. Th e
v ast maj orit y of cases of p rox imal
RTA are seen in associat ion wit h
ot h er g enet ic disorders, in wh ich
t h e acid- base dist urbance is sim-
p ly a p art of a g eneraliz ed p rox i-
mal t ubular dysf unct ion called
t h e renal F anconi syndrome. 2 5 , 2 6
I n t h ese indiv iduals, t h e g enet ics
of t h e RTA f ollows t h e p at t ern of
t h e underlying disorder, almost
always an aut osomal recessiv e
t rait . I t is wort h not ing t h at t yp e 2
RTA due t o a carbonic anh ydrase
( C A I I ) def iciency occurs in asso-
ciat ion wit h ost eop et rosis and
cerebral calcif icat ion as an aut o-
somal recessiv e t rait , as well. 2 7 C A
I I def iciency may also cause a
mix ed t yp e I - t yp e I I RTA, orig i-
nally desig nat ed t yp e I I I , a t erm
no long er in use. C A I I h as been
map p ed t o 8 q 2 2 ; use of a C A
1 I - def icient mouse model h as
p rov ided t h e basis f or successf ul,
but t emp orary g ene t h erap y. 2 8
I n cont rast , dist al RTA occurs
wit h t h e g reat est f req uency as an
isolat ed def ect , of t en t ransmit t ed
as an aut osomal dominant t rait
due t o a mut at ion at 1 7 q 2 1 - q 2 2 . 2 9
Th e molecular abnormalit y in
t h ese cases is an imp aired C l- -
HC 0 3 - ex ch ang er wit h in t h e cell
at t h e ant iluminal surf ace, as p re-
v iously discussed. Norman and as-
sociat es3 0 st udied t wo p edig rees
in wh ich clinically af f ect ed indi-
v iduals were sh own t o be h yp oci-
t rat uric; ot h er, asymp t omat ic
members of t h e p edig ree wit h in-
comp let e dist al RTA were f ound
t o be h yp ocit rat uric and were also
sh own t o h av e an abnormal re-
sp onse t o acid loading . Th ese ob-
serv at ions are ent irely consist ent
wit h an aut osomal dominant t rait .
I n addit ion, dist al RTA can be in-
h erit ed as an aut osomal recessiv e
t rait , wit h or wit h out associat ed
sensorineural h earing loss. Th ose
indiv iduals wit h out h earing de-
5 4 0 C LI NI C ALPEDI ATRI C S OC TOB ER 2 0 0 1
5 4 0 C LI NI C ALPEDI ATRI C S OC TOB ER 2 0 0 1
at MCMASTER UNIV LIBRARY on August 24, 2010 cpj.sagepub.com Downloaded from
Renal Tubular Acidosis
f ect s carry mut at ions at 7 q 3 3 -
q 3 4 . 9 Dist al RTA in associat ion
wit h h earing loss h as been sh own
t o inv olv e t h e g ene ( ATP6 B 1 )
coding f or t h e B - subunit of t h e
H+ - ATPase, 8 wh ich is normally re-
sp onsible f or t h e secret ion of h y-
drog en ion int o t h e lumen. S ig -
nif icant ly, neit h er of t h e t wo
recessiv e f orms of dist al RTA in-
v olv es a locus ev en remot ely con-
nect ed wit h t h at wh ich det er-
mines t h e ch loride- bicarbonat e
ex ch ang er def ect in t h e domi-
nant t rait . Th us, t h ere are clearly
at least t h ree dist inct abnormali-
t ies of t h e g enome wh ich can ad-
v ersely af f ect urinary acidif icat ion
in t h e dist al t ubule. W h ile a g ood
deal of workremains t o be done
on t h e molecular biolog y of RTA,
t h e dat a are already beg inning t o
h elp us t o underst and t h e clinical
g enet ics as well as t h e p at h op h ysi-
olog y t o a deg ree not p ossible 2 0
years ag o.
V ariat ion on t h e Th eme
I n p ast lit erat ure on t h e sub-
j ect , RTA nomenclat ure h ad
ev olv ed t o a deg ree of conf usion
v ast ly out of p rop ort ion t o it s un-
derlying p at h op h ysiolog ic com-
p lex it y. Th e more recent lit era-
t ure on t h e subj ect deals
essent ially wit h t h ree t yp es: 1 , 2 ,
and 4 . I t is nowclearly recog -
niz ed t h at t yp e 4 , also called h y-
p erkalemic dist al RTA t o dist in-
g uish it f rom classical t yp e 1 , is an
acq uired def ect g enerally due t o
eit h er aldost erone def iciency or
relat iv e aldost erone resist ance. 3 1
Th e f irst sit uat ion of t en p ert ains
in cases of cong enit al adreno-
g enit al syndrome, wh ile t h e sec-
ond may be seen wh enev er renal
mass is diminish ed ( e. g . , obst ruc-
t iv e urop at h y, diabet ic nep h rop a-
t h y) . Alt h oug h ch ronic renal f ail-
ure is a p rominent cause of t yp e
4 RTA in adult s, it is rarely seen
in ch ildren. Th e mech anism be-
h ind t h e h yp erkalemia is p lainly
an imp aired or inh ibit ed ex -
ch ang e of p ot assium f or sodium,
a p rocess reg ulat ed in t h e dist al
t ubule by aldost erone. Th e same
ap p lies t o t h e syst emic accumula-
t ion of H+ , since secret ion of h y-
drog en ion is linked t o t h e same
p rocess t h at is imp aired in t h e
absence of normal aldost erone
reg ulat ion.
I ncidence
Th e relat iv e incidence of t h e
t h ree t yp es of RTA was rep ort ed
by B rennen and associat es3 2
sh ort ly af t er t h e init ial descrip -
t ion of t yp e 4 RTA. Th ese work-
ers sug g est ed t h at t yp e 1 was
most common, f ollowed by t yp e
4 , wit h t yp e 2 t h e least common
of all. Th is order is, h owev er, un-
likely because g enet ic def ect s
rarely, if ev er, out number ac-
q uired ones. Th us, t h e number
of elderly males wit h p rost at ic h y-
p ert rop h y and p at ient s of all ag es
wit h obst ruct iv e urop at h y wh o
become relat iv ely resist ant t o al-
dost erone and in wh om t yp e 4
RTA dev elop s are clearly more
numerous t h an indiv iduals wit h
mut at ions f or a ch loride- bicar-
bonat e ex ch ang er ( t yp e 1 ) . Al-
t h oug h it is cert ain t h at ev ery in-
f ant is born wit h a lower
bicarbonat e t h resh old t h an it s
p arent s, most newborns do not
dev elop syst emic acidosis in rela-
t ion t o t h eir ag e coh ort s as a con-
seq uence. Nonet h eless, it is at
least arg uable t h at t yp e 2 , due t o
a p h ysiolog ic immat urit y, ap -
p ears in t h e g eneral p op ulat ion
more f req uent ly t h an g enet ically
det ermined t yp e 1 . Howev er, it is
cert ain t h at af t er inf ancy, iso-
lat ed t yp e 1 is seen f ar more com-
monly t h an isolat ed t yp e 2 .
Treat ment
Th e basis f or t reat ment of a
p at ient wit h any f orm of RTA is
t h e result ing met abolic acidosis,
wh ich all p at ient s ex p erience. I n
p rox imal RTA, wh ere t h e f unda-
ment al p h ysiolog ic abnormalit y,
as we h av e def ined it , is in base re-
absorp t ion, it st ands t o reason
t h at base rep lacement would be
t h erap eut ic. Th us, base rep lace-
ment as sodium bicarbonat e or
t h e more p alat able alt ernat iv e,
cit rat e or S h oh l' s solut ion ( 2 - 1 4
mEq / kg / day in div ided doses3 3 )
is ut iliz ed t o maint ain p lasma bi-
carbonat e h ig h er t h an t h e re-
duced Tm and of f set t h e increased
urinary losses. I n bot h f orms of
dist al RTA, not wit h st anding t h e
dif f erent underlying mech anism
comp ared t o t yp e 2 RTA, t h e clin-
ical p roblem remains a syst emic
met abolic acidosis. C it rat e re-
p lacement h as been used as an ef -
f ect iv e mainst ay of t reat ment in
t yp e 1 RTA. F inally, in t reat ment
of t yp e 4 RTA, it is essent ial t o de-
t ermine t h e underlying mech a-
nism, wh et h er h yp oaldost ero-
nism v s end- org an resist ance. F or
t h e f ormer st at e, mineralocort i-
coid rep lacement is ef f ect iv e, but
t h e p at ient sh ould be monit ored
f or sodium ret ent ion and v olume
ov erload. F or t h e lat t er, g enerally
result ing f rom ch ronic renal dis-
ease, administ rat ion of
f urosemide ( 2 mg / kg / day) is
h ig h ly ef f ect iv e and av oids t h e
p roblem of v olume ov erload by
p romot ing sodium ex cret ion.
C onclusions
W e p resent ed a concep t ion of
t h e t wo maj or t yp es of RTA based
on t h e ch aract erist ic f unct ional
def icit of each . I n t h e case of t yp e
2 ( p rox imal) RTA, t h e underlying
g enet ic def ect in sodium- bicar-
OC TOB ER 2 0 0 1
C LI NI C ALPEDI ATRI C S 5 4 1
OC TOB ER 2 0 0 1 C L1 7 V I C ALPEDI ATRI C S 5 4 1
at MCMASTER UNIV LIBRARY on August 24, 2010 cpj.sagepub.com Downloaded from
Rot h , C h an
bonat e cot ransp ort er molecule
( NB C - 1 ) result s in a def icit in
base reabsorp t ion. Th us, p rox i-
mal RTA result s in reduced
p lasma bicarbonat e and syst emic
met abolic acidosis on t h is basis.
B y cont rast , t yp e 1 ( dist al) RTA h as
been p resent ed as a f ailure t o elim-
inat e h ydrog en ion, a concep t am-
p ly sup p ort ed by t h e molecular
def init ion of a g enet ic def iciency
of t h e ch loride- bicarbonat e ex -
ch ang er molecule imp airing t h e
dist al t ubule' s abilit y t o secret e
H+ . Th e ut ilit y of t h is concep t ual-
iz at ion lies p rimarily in t h e f act
t h at it emp h asiz es bot h t h e nor-
mal and abnormal f unct ion of
each of t h e t wo inv olv ed seg -
ment s, wh ile also h elp ing t o ex -
p lain t h e p h ysiolog ic basis f or t h e
clinical p resent at ions.
Th e marked abnormalit ies of
linear g rowt h , p art icularly ev i-
dent in dist al RTA, are under-
st ood as t h e result of at least t wo
sep arat e set s of ev ent s: ost eoma-
lacia and bowing of t h e lower ex -
t remit ies due t o calcium loss;
and, t h e acidosis- induced
ch ang es in t h e g rowt h h ormone-
I G F ax is. Our knowledg e of t h e
lat t er inf luence is st ill in t h e most
rudiment ary st ag es, alt h oug h
t ech niq ues of molecular biolog y
p rov ide t h e p romise of rap id ad-
v ances in t h e near f ut ure. Th e
molecular g enet ics of RTA h as
p rog ressed dramat ically in t h e
p ast decade, p rov iding ev idence
of t h e act ual molecular def ect s in
t yp es 1 and 2 RTA and f urt h ering
our underst anding of t h e under-
lying cellular ev ent s. Th ese ob-
serv at ions h av e also h elp ed
g reat ly in our delineat ion of t h e
inh erit ance p at t erns of bot h
p rox imal and dist al RTA. Th us,
t h e p rog ress in t h e p ast t wo
decades h as been dramat ic and
h olds direct imp licat ions f or clin-
ical care of p at ient s af f ect ed by
RTA.
REF ERENC ES
1 . Edelmann C M, Rodrig uez - S oriano J ,
B ioch is H, et al. Renal bicarbonat e re-
absorp t ion and h ydrog en ion ex cre-
t ion in inf ant s. J C lin I nv est . 1 9 6 7 ;
4 6 :1 3 0 9 - 1 3 1 7 .
2 . S v enning sen NW . Renal acid- base
t it rat ion st udies in inf ant s wit h and
wit h out met abolic acidosis in t h e p ost -
neonat al p erod. Pediat r Res. 1 9 7 4 ;
8 :6 5 9 - 6 7 2 .
3 . Dobyan DC , B ulg er RE. Renal car-
bonic anh ydrase. AmJ Ph ysiol. 1 9 8 2 ;
2 4 3 :F 3 1 1 - F 3 2 4 .
4 . B oron W F , F ong P, Hedig er MA, et al.
Th e elect rog enic Na/ HC O3 cot rans-
p ort er. W ien K lin W och ensch r 1 9 9 7 ;
1 0 9 :4 4 5 - 4 5 6 .
5 . S oleimani M, B urnh am C E. Ph ysio-
log ic and molecular asp ect s of t h e
Na+ :HC O3 - cot ransp ort er in h ealt h
and disease p rocesses. K idney I nt .
2 0 0 0 ; 5 7 :3 7 1 - 3 8 4 .
6 . McK inney TD, B urg MB . B icarbonat e
absorp t ion by rabbit cort ical collect -
ing t ubules in v it ro. AmJ Ph ysiol. 1 9 7 6 ;
2 3 4 :F 1 4 1 - F 1 4 5 .
7 . F ish er J L, Hust ed RF , S t einmet z PR.
C h loride dep endence of t h e HC O3 -
ex it st ep in urinary acidif icat ion by
t h e t urt le bladder. AmJ Ph ysiol. 1 9 8 3 ;
2 4 5 :F 5 6 4 - F 5 6 8 .
8 . K aret F E, G ainz a F J , G yory AZ , et al.
Mut at ions in t h e ch loride- bicarbonat e
ex ch ang er g ene AE1 cause aut osomal
dominant but not aut osomal recessiv e
dist al renal t ubular acidosis. Proc Nat l
Acad S ci. 1 9 9 8 ; 9 5 :6 3 3 7 - 6 3 4 2 .
9 . K aret F E, F inberg K E, Nayir A, et al.
Localiz at ion of a g ene f or aut osomal
recessiv e dist al renal t ubular acidosis
wit h normal h earing ( rdRTA2 ) t o
7 q 3 3 - 3 4 . AmJ Hum G enet . 1 9 9 9 ;
6 5 :1 6 5 6 - 1 6 6 5 .
1 0 . Andersson B , Leksel LG , Rundg ren
M. Reg ulat ion of wat er int ake. Annu
Rev Nut r 1 9 8 2 ; 2 :7 3 - 8 9 .
1 1 . Moore EW . I oniz ed calcium in nor-
mal serum, ult raf ilt rat es and wh ole
blood det ermined by ion- ex ch ang e
elect rodes. J C lin I nv est . 1 9 7 0 ; 4 9 :3 1 8 - .
1 2 . Pedersen K O. B inding of calcium t o
serum albumin: I I . Ef f ect of p H v ia
comp et it iv e h ydrog en and calcium
ion binding t o t h e imidaz ole g roup s
of albumin. S cand J C lin Lab I nv est .
1 9 7 2 ; 2 9 :7 5 - .
1 3 . MelnickJ Z , S rere PA, Elsh ourbag y
NA, et al. Adenosine t rip h osp h at e cit -
rat e lyase mediat es h yp ocit rat uria in
rat s. J C lin I nv est . 1 9 9 6 ; 9 8 :2 3 8 1 - 2 3 8 7 .
1 4 . Dedmon RE, W rong 0 . Th e ex cret ion
of org anic anion in renal t ubular aci-
dosis wit h p art icular ref erence t o cit -
rat e. C lin S ci. 1 9 6 2 ; 2 2 :1 9 - 3 2 .
1 5 . S t rif e C F , C lardy C W , V arade W S , et al.
U rine- t o- blood carbon diox ide t en-
sion g radient and max imal dep res-
sion of urinary p H t o dist ing uish rat e-
dep endent f rom classic dist al renal
t ubular acidosis in ch ildren. J Pediat r
1 9 9 3 ; 1 2 2 :6 0 - 6 5 .
1 6 . Rodrig uez - S oriano J , V allo A. Renal
t ubular acidosis. Pediat rNep h rol. 1 9 9 0 ;
4 :2 6 8 - 2 7 5 .
1 7 . HannaJ D, S ch einmanJ I , C h an J C M.
Th e kidney in acid- base balance. Pedi-
at r C lin Nort h Am. 1 9 9 5 ; 4 2 :1 3 6 5 - 1 3 9 5 .
1 8 . Alon U , Hellerst ein S , W arady B A.
Oral acet az olamide in t h e assessment
of ( urine- blood) p C 0 2 - Pediat r
Nep h rol. 1 9 9 1 ; 5 :3 0 7 - 3 1 1 .
1 9 . McS h erry E. Renal t ubular acidosis in
ch ildh ood. K idney I nt . 1 9 8 1 ; 2 0 :7 9 9 -
8 0 9 .
2 0 . C h allaA, K rieg RJ J r, Th abet MA, et al.
Met abolic acidosis inh ibit s g rowt h
h ormone secret ion in rat s: mech a-
nism of g rowt h ret ardat ion. AmJ Ph ys-
iol. 1 9 9 3 ; 2 6 5 :E5 4 7 - E5 5 3 .
2 1 . G uillery EN, K arniski LP, Mat h ews
MS , RobillardJ E. Mat urat ion of p rox -
imal t ubule Na+ / H+ ant ip ort er act iv it y
in sh eep f rom f et us t o newborn. AmJ
Ph ysiol. 1 9 9 4 ; 2 6 7 :F 5 3 7 - F 5 4 5 .
2 2 . B aum M, Moe OW , G ent ry DL,
Alp ern RJ . Ef f ect of g lucocort icoids
on renal cort ical NHE- 3 and NHE- 1
mRNA. AmJ Ph ysiol. 1 9 9 4 ; 2 6 7 :F 4 3 7 -
F 4 4 2 .
2 3 . Rut h erf ord PA. Ex p ression of Na+ - H+
ex ch ang er isof orms in t h e kidney-
imp licat ions f or renal f unct ion and
disease. Nep h rol Dial Transp lant . 1 9 9 6 ;
1 1 :1 7 1 1 - 1 7 1 3 .
2 4 . Romero MF , B oron W F . Elect rog enic
Na+ / HC O3 - cot ransp ort ers: cloning
and p h ysiolog y. Annu Rev Ph ysiol.
1 9 9 9 ; 6 1 :6 9 9 - 7 2 3 .
2 5 . F oremanJ W , Rot h K S . Th e h uman re-
nal F anconi syndrome- t h en and
now. Nep h rolog y. 1 9 8 9 ; 5 1 :3 0 1 - 3 0 6 .
5 4 2 C LI NI C ALPEDI ATRI C S OC TOB ER 2 0 0 1
5 4 2 C LI NI C ALPEDI ATRI C S OC TOB ER 2 0 0 1
at MCMASTER UNIV LIBRARY on August 24, 2010 cpj.sagepub.com Downloaded from
Renal Tubular Acidosis
2 6 . Rodrig uez - S oriano J . Newinsig h t s
int o t h e p at h og enesis of renal t ubular
acidosis- f rom f unct ional t o molecu-
lar st udies. Pediat r Nep h rol. 2 0 0 0 ;
1 4 :1 1 2 1 - 1 1 3 6 .
2 7 . Rot h DE, V ent a PJ , Tash ian RE, S ly
W S . Molecular basis of h uman car-
bonic anh ydrase I I def iciency. Proc
Nat l Acad S ci U S A. 1 9 9 2 ; 8 9 :1 8 0 4 -
1 8 0 8 .
2 8 . Lai LW , C h an DM, Erickson RP, et al.
C orrect ion of renal t ubular acidosis in
carbonic anh ydrase 1 I - def icient mice
wit h g ene t h erap y. J C lin I nv est . 1 9 9 8 ;
1 0 1 :1 3 2 0 - 1 3 2 5 .
2 9 . J arolim P, S h ayakul C , Prabakaran D,
et al. Aut osomal dominant dist al renal
t ubular acidosis is associat ed in t h ree
f amilies wit h h et eroz yg osit y f or t h e
R5 8 9 H mut at ion in t h e AE1 ( band 3 )
C l- / HC O3 - ex ch ang er. J B iol C h em.
1 9 9 8 ; 2 7 3 :6 3 8 0 - 6 3 8 8 .
3 0 . Norman ME, F eldman NI , C oh n RM,
et al. U rinary cit rat e ex cret ion in t h e
diag nosis of dist al renal t ubular acido-
sis. J Pediat x 1 9 7 8 ; 9 2 :3 9 4 - 4 0 0 .
3 1 . Morris RC J r. Renal t ubular acidosis.
NEng lJ Med. 1 9 8 1 ; 3 0 4 :4 1 8 - 4 2 0 .
3 2 . B renner RJ , S p ring DB , S ebast ian A,
et al. I ncidence of radiolog ically ev i-
dent bone disease, nep h rocalcinosis,
and nep h rolit h iasis in v arious t yp es of
renal t ubular acidosis. NEng lJ Med.
1 9 8 2 :2 1 7 - 2 2 1 .
3 3 . S ant os F , C h an J C M. Renal t ubular
acidosis in ch ildren: diag nosis, t reat -
ment and p rog nosis. AmJ Nep h rol.
1 9 8 6 ; 6 :2 8 9 - 2 9 5 .
OC TOB ER 2 0 0 1
C LI NI C ALPEDI ATRI C S 5 4 3 ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
C LI NI C ALPEDI ATRI C S 5 4 3 OC TOB ER 2 0 0 1
at MCMASTER UNIV LIBRARY on August 24, 2010 cpj.sagepub.com Downloaded from
You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- SM-204-TechReport 01 2022 AnsichtDocument4 pagesSM-204-TechReport 01 2022 AnsichtDanny DoanNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- DPP 04 (Of Lec 06)Document3 pagesDPP 04 (Of Lec 06)Aabha BhartiNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- WRM Training ReportDocument42 pagesWRM Training Reportpremkumar165No ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Power Facility Coatings Brochure BROPWDocument5 pagesPower Facility Coatings Brochure BROPWprakashNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Acgih Manual 1998 (401-500)Document100 pagesAcgih Manual 1998 (401-500)HéctorNo ratings yet
- FinfetDocument25 pagesFinfetsathyanarainraoNo ratings yet
- Limit States Design in Structural Steel: G.L. Kulak and G.Y. Grondin 9 Edition, 1 Printing 2010Document19 pagesLimit States Design in Structural Steel: G.L. Kulak and G.Y. Grondin 9 Edition, 1 Printing 2010Rania Kanj KiwanNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Inorganic Chemistry Practice Booklet-1Document65 pagesInorganic Chemistry Practice Booklet-1godlanshul32No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Study of Material Non-Linearity During Deformation Using FEM SofwareDocument82 pagesA Study of Material Non-Linearity During Deformation Using FEM SofwareRicky GunawanNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Phase Equilibrium Study in The CaODocument5 pagesPhase Equilibrium Study in The CaOsattiricNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Retrofitting of RC Structure Using FRP Laminate: AbstractDocument10 pagesRetrofitting of RC Structure Using FRP Laminate: AbstractYo Yo AkNo ratings yet
- 2603988Document14 pages2603988Don RahulNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- [Synthetic Metals 1985-oct vol. 11 iss. 6] Boehm, H.P._ Setton, R._ Stumpp, E. - Nomenclature and terminology of graphite intercalation compounds. Report by a subgroup of the international committee for charac (198Document9 pages[Synthetic Metals 1985-oct vol. 11 iss. 6] Boehm, H.P._ Setton, R._ Stumpp, E. - Nomenclature and terminology of graphite intercalation compounds. Report by a subgroup of the international committee for charac (198Ricardinho1987No ratings yet
- Petrochemicals An Overview (STUDENT) (3of3)Document175 pagesPetrochemicals An Overview (STUDENT) (3of3)Chuah Chong Yang100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Technological Result of Decomposition Sodium Aluminate SolutionDocument10 pagesTechnological Result of Decomposition Sodium Aluminate SolutionDragana Dragojlović SmiljanicNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Soil Classification2 - USDA Soil Taxonomy Upgrade-Trinidad and TobagoDocument13 pagesSoil Classification2 - USDA Soil Taxonomy Upgrade-Trinidad and TobagoPlaiboiNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Concrete ClothDocument20 pagesConcrete ClothShrinivasNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- GB150 1-2011enDocument46 pagesGB150 1-2011enIrfan AhmedNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Yield Strength Yield Point Stress Yield Point Stress Elastic Limit Elastic LimitDocument1 pageYield Strength Yield Point Stress Yield Point Stress Elastic Limit Elastic LimitCarlito Jr JavilloNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Automotive Aluminium Catalogue 2022Document140 pagesAutomotive Aluminium Catalogue 2022badnet1980No ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Summary Guide in Earth ScienceDocument7 pagesSummary Guide in Earth ScienceMeriam WebsterNo ratings yet
- IjoiijDocument347 pagesIjoiijpi.314153.4No ratings yet
- A Brief Guide To Calculating Embodied CarbonDocument6 pagesA Brief Guide To Calculating Embodied Carbonmatt calvertNo ratings yet
- NDT Method SummaryDocument3 pagesNDT Method SummaryNguyen Anh TungNo ratings yet
- TimberDocument3 pagesTimberAllan SsemujjuNo ratings yet
- What Differentiates Coiled Pins?: Prior To InstallationDocument2 pagesWhat Differentiates Coiled Pins?: Prior To Installationarda akkayaNo ratings yet
- 200319-Final Exam - Machine DesignDocument2 pages200319-Final Exam - Machine DesignJoseph RefuerzoNo ratings yet
- Basic Physical Properties of PVOH ResinDocument40 pagesBasic Physical Properties of PVOH ResinJavier RealNo ratings yet
- Optical Brightener Uvitex OB Msds Baoxu ChemicalDocument11 pagesOptical Brightener Uvitex OB Msds Baoxu ChemicalBhaumik ParmarNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Coursebook Answers: Science in Context: Lord of The RingsDocument39 pagesCoursebook Answers: Science in Context: Lord of The RingsEshanNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
























![[Synthetic Metals 1985-oct vol. 11 iss. 6] Boehm, H.P._ Setton, R._ Stumpp, E. - Nomenclature and terminology of graphite intercalation compounds. Report by a subgroup of the international committee for charac (198](https://imgv2-2-f.scribdassets.com/img/document/613195716/149x198/cd1cc2775e/1710575975?v=1)