You might also like
- Generic Name T Rade Name Classification Minitran Anti Angina NitroglycerinDocument1 pageGeneric Name T Rade Name Classification Minitran Anti Angina NitroglycerinChristopher LeeNo ratings yet
- IV PO Conversion CAPDocument3 pagesIV PO Conversion CAPdamondouglasNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- Daptomycin (Cubicin)Document1 pageDaptomycin (Cubicin)Adrianne BazoNo ratings yet
- Stimulates Peripheral Glucose Uptake, Inhibits Hepatic Glucose Production, Inhibits Lipolysis and Proteolysis, Regulating Glucose MetabolismDocument4 pagesStimulates Peripheral Glucose Uptake, Inhibits Hepatic Glucose Production, Inhibits Lipolysis and Proteolysis, Regulating Glucose MetabolismKey CelestinoNo ratings yet
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingFrom EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováNo ratings yet
- Preload and AfterloadDocument28 pagesPreload and Afterloadapi-19916399100% (1)
- InsulinDocument1 pageInsulinamaliea234No ratings yet
- Antibiotics 9Document11 pagesAntibiotics 9Beth Morales100% (1)
- Assessing Abdominal Distensión After GastrectomyDocument1 pageAssessing Abdominal Distensión After GastrectomyEunice CortésNo ratings yet
- Module4 Resp-InhaledAnticholinergics-IpratropiumDocument1 pageModule4 Resp-InhaledAnticholinergics-IpratropiumnoeyeshaveseenNo ratings yet
- PharmacokineticsDocument7 pagesPharmacokineticsJan KarnowskiNo ratings yet
- Therapeutic Drug Monitoring in The ElderlyDocument3 pagesTherapeutic Drug Monitoring in The ElderlyKristine BaringNo ratings yet
- Drug DigoxinDocument1 pageDrug DigoxinSrkocherNo ratings yet
- Mu 002Document10 pagesMu 002chandanNo ratings yet
- LevaquinDocument1 pageLevaquinKatie McPeek100% (1)
- With Dr. Susan Lipsett: Community Acquired PneumoniaDocument1 pageWith Dr. Susan Lipsett: Community Acquired PneumoniaJayantiNo ratings yet
- Aerovent, Apovent Atronase, Ipraxa, Ipvent Rhinovent, Rinatecrinovagos, Atrovent, Atrovent HfaDocument4 pagesAerovent, Apovent Atronase, Ipraxa, Ipvent Rhinovent, Rinatecrinovagos, Atrovent, Atrovent HfaGwyn RosalesNo ratings yet
- Common Drug Stems Cheat Sheet: Drug Stem Drug Class And/or Stem Explanation ExamplesDocument2 pagesCommon Drug Stems Cheat Sheet: Drug Stem Drug Class And/or Stem Explanation ExamplesjthsNo ratings yet
- Drug AtivanDocument1 pageDrug AtivanSrkocherNo ratings yet
- Opioid Analgesics: Just in Time Training September 2006Document16 pagesOpioid Analgesics: Just in Time Training September 2006Yel CMNo ratings yet
- AnxietyDocument5 pagesAnxietyJohn HolmesNo ratings yet
- Critical Care Drugs 2Document23 pagesCritical Care Drugs 2Asri Ernadi100% (1)
- Generic Name FurosemideDocument1 pageGeneric Name FurosemideChristopher LeeNo ratings yet
- Drugs To Watch With WARFARINDocument3 pagesDrugs To Watch With WARFARINRajendra RaiNo ratings yet
- Know Common Disease ManagementDocument14 pagesKnow Common Disease Managementcdx25No ratings yet
- Drug AdvilDocument1 pageDrug AdvilDiana Laura LeiNo ratings yet
- DrugsDocument155 pagesDrugsAkankshaNo ratings yet
- Zocor Drug CardDocument1 pageZocor Drug CardSheri490No ratings yet
- Ciprofloxacin CiproDocument1 pageCiprofloxacin CiproKristi WrayNo ratings yet
- Grapefruit Juice and Drug Interactions - 0717Document2 pagesGrapefruit Juice and Drug Interactions - 0717Asri YaniNo ratings yet
- Docusate Sodium (Colace)Document1 pageDocusate Sodium (Colace)Adrianne BazoNo ratings yet
- Drug DilantinDocument1 pageDrug DilantinSrkocherNo ratings yet
- Warfarin Mechanism of ActionDocument7 pagesWarfarin Mechanism of ActionIna GrigorasNo ratings yet
- Pharmacology of Cardiac Diseases MINEDocument3 pagesPharmacology of Cardiac Diseases MINEMitu Miressa تNo ratings yet
- Antibiotic GuideDocument6 pagesAntibiotic GuideAnnTran100% (1)
- Midazolam FinalDocument2 pagesMidazolam FinalAhmad AbqariNo ratings yet
- Remembering Medication ClassificationsDocument2 pagesRemembering Medication ClassificationsGVHHNo ratings yet
- Mechanism of Action For Each Class of AntiDocument146 pagesMechanism of Action For Each Class of AntiReynaldo RiveraNo ratings yet
- Pharmocology Drug Cards: InnovarDocument33 pagesPharmocology Drug Cards: InnovarfaizaNo ratings yet
- Drug KenalogDocument1 pageDrug KenalogSrkocherNo ratings yet
- DigoxinDocument18 pagesDigoxinApril Mergelle LapuzNo ratings yet
- Pharmacology FirecrackerDocument37 pagesPharmacology FirecrackerRehan Usman100% (1)
- 07 Dosage RegimenDocument44 pages07 Dosage Regimenzetttttttttt100% (3)
- Prescribing Medicine in Pregnancy, by Australian Drug Evaluation CommitteeDocument90 pagesPrescribing Medicine in Pregnancy, by Australian Drug Evaluation Committee徐承恩100% (1)
- Template Drug Card1Document1 pageTemplate Drug Card1Kay TaylorNo ratings yet
- Drug OmeprazoleDocument1 pageDrug OmeprazoleSrkocherNo ratings yet
- MupirocinDocument13 pagesMupirocinkurutalaNo ratings yet
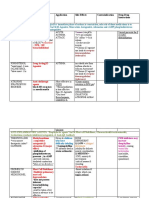
- Drug Name Mechanism Application Side Effects Contraindication Drug-Drug InteractionsDocument3 pagesDrug Name Mechanism Application Side Effects Contraindication Drug-Drug Interactionsazhar hussinNo ratings yet
- Half LifeDocument43 pagesHalf LifeMinal Nadeem100% (1)
- DiflucanDocument1 pageDiflucanSheri490No ratings yet
- CarafateDocument1 pageCarafateAdrianne BazoNo ratings yet
- Drug CardDocument2 pagesDrug CardHannahNo ratings yet
- Cardiovascular System Drugs - Active Stack® Pharmacology Flash Cards - Study Materials - My ATIDocument1 pageCardiovascular System Drugs - Active Stack® Pharmacology Flash Cards - Study Materials - My ATIAntonette Joy SolinapNo ratings yet
- Emergency Drugs Used in O.S. Common Drug Interactions in O.S. Practice Oral SurgeryDocument52 pagesEmergency Drugs Used in O.S. Common Drug Interactions in O.S. Practice Oral SurgeryFourthMolar.comNo ratings yet
- Huma Log Drug CardDocument1 pageHuma Log Drug CardJanet SheldonNo ratings yet
- PF Law Free Paul JBL 134 2015 637 501Document14 pagesPF Law Free Paul JBL 134 2015 637 501l1o2stNo ratings yet
- Hum Notebook Nov2005Document142 pagesHum Notebook Nov2005l1o2stNo ratings yet
- A Critique of Gentry and Wellum'S, Kingdom Through Covenant: A Hermeneutical-Theological ResponseDocument17 pagesA Critique of Gentry and Wellum'S, Kingdom Through Covenant: A Hermeneutical-Theological Responsel1o2stNo ratings yet
- 43 308 1 PB PDFDocument10 pages43 308 1 PB PDFl1o2stNo ratings yet
- Acls Study Guide September 2011Document18 pagesAcls Study Guide September 2011Zarah Jane Rull NateNo ratings yet
- Pscf9 11meyer RebuttalDocument12 pagesPscf9 11meyer Rebuttall1o2stNo ratings yet
- Reading ListDocument1 pageReading Listl1o2stNo ratings yet
- Who Will Be Left Behind Rethinking Matt 24 WTJDocument12 pagesWho Will Be Left Behind Rethinking Matt 24 WTJl1o2stNo ratings yet
- GGC BookDocument96 pagesGGC Bookl1o2st100% (1)
- Distinguishing TRALI and TACODocument6 pagesDistinguishing TRALI and TACOl1o2stNo ratings yet
- Cleveland Journal - Update On COPDDocument11 pagesCleveland Journal - Update On COPDl1o2stNo ratings yet
- Management PoisoningDocument6 pagesManagement PoisoningatifdocNo ratings yet
- Acute Liver Failure Update 2011Document26 pagesAcute Liver Failure Update 2011Andreea Alina TanaseNo ratings yet
- EcgDocument7 pagesEcgdeenadayalusNo ratings yet
- Penal Substitution in Church HistoryDocument16 pagesPenal Substitution in Church HistoryDavid Salazar100% (1)
- Clinical Presentation of MyoclonusDocument6 pagesClinical Presentation of Myoclonusl1o2stNo ratings yet
- Clinical Presentation of MyoclonusDocument6 pagesClinical Presentation of Myoclonusl1o2stNo ratings yet
- VentilatorDocument90 pagesVentilatorthenaloveNo ratings yet
- 06 WilsonDocument22 pages06 Wilsonl1o2stNo ratings yet
- VOL06Document341 pagesVOL06l1o2stNo ratings yet
- Understanding The TrinityDocument13 pagesUnderstanding The Trinityl1o2stNo ratings yet
- Edubriefs in CCTC: Svo (Mixed Venous Oxygen Saturation) or Scvo Central Venous Oxygen Saturation)Document3 pagesEdubriefs in CCTC: Svo (Mixed Venous Oxygen Saturation) or Scvo Central Venous Oxygen Saturation)l1o2stNo ratings yet
- Teper, Segal, & Inzlicht - Inside The Mindful Mind (In Press)Document6 pagesTeper, Segal, & Inzlicht - Inside The Mindful Mind (In Press)l1o2st100% (1)
- 10429Document2 pages10429l1o2stNo ratings yet
- 2 Corinthians 12 - Triumphalism, Suffering and Spiritual MaturityDocument26 pages2 Corinthians 12 - Triumphalism, Suffering and Spiritual Maturityl1o2st100% (1)
- Syllabus Ma Islamic StudiesDocument13 pagesSyllabus Ma Islamic StudiesshoebIASNo ratings yet
- Review Dunn PaulDocument10 pagesReview Dunn PaulJosé C.0% (1)
- Colossians-Personal Notes: 1. Paul's Messengers (4:7-9)Document5 pagesColossians-Personal Notes: 1. Paul's Messengers (4:7-9)l1o2stNo ratings yet
- ReviewDocument4 pagesReviewl1o2stNo ratings yet
- Consent in Gaming FillableDocument1 pageConsent in Gaming FillableChuck Barnard100% (1)
- Comprehensive Barangay Youth Development Plan (Cbydp)Document7 pagesComprehensive Barangay Youth Development Plan (Cbydp)Drena DertoNo ratings yet
- Dialectical Behavior Therapy Compared With General Psychiatric Management For Borderline Personality Disorder Clinical Outcomes and Functioning Over A 2-Year Follow-UpDocument12 pagesDialectical Behavior Therapy Compared With General Psychiatric Management For Borderline Personality Disorder Clinical Outcomes and Functioning Over A 2-Year Follow-UpPechopalomo 90No ratings yet
- Admin,+8Document9 pagesAdmin,+8Dewi RatnasariNo ratings yet
- PDF DocumentDocument1 pagePDF DocumentEuna DawkinsNo ratings yet
- Proximal Humerus Fracture: Fracture Care Team: Shared Care PlanDocument7 pagesProximal Humerus Fracture: Fracture Care Team: Shared Care PlanIlie OnuNo ratings yet
- Understanding and Completing The Reversion (25pp)Document25 pagesUnderstanding and Completing The Reversion (25pp)Tony Lambert100% (3)
- Causal Inference For Data Science (MEAP) - de VillaDocument163 pagesCausal Inference For Data Science (MEAP) - de VillaJuan RodriguezNo ratings yet
- Illegal Gold Mines in The PhilippinesDocument2 pagesIllegal Gold Mines in The PhilippinesMaricar RamirezNo ratings yet
- DERMOID CYST FINAL NaDocument56 pagesDERMOID CYST FINAL NaRhobic ManansalaNo ratings yet
- Es Compleat Coolant Eg Premix - MSDS - Lt16587aDocument6 pagesEs Compleat Coolant Eg Premix - MSDS - Lt16587aCesar G.No ratings yet
- Tanezumab For The Treatment of PainDocument15 pagesTanezumab For The Treatment of PainTony HartantoNo ratings yet
- Template For Co Ntingency Planning DivisionDocument21 pagesTemplate For Co Ntingency Planning Divisionelizer encarnacionNo ratings yet
- Civil Hospital Visit Report: TH NDDocument5 pagesCivil Hospital Visit Report: TH NDPranita DisaleNo ratings yet
- File Test 7 Grammar, Vocabulary, and Pronunciation A: Grammar 1 Underline The Correct Word(s)Document7 pagesFile Test 7 Grammar, Vocabulary, and Pronunciation A: Grammar 1 Underline The Correct Word(s)Darin Sopanha100% (2)
- Working in A Group EssayDocument4 pagesWorking in A Group Essayjvscmacaf100% (2)
- Medical Nutrition Therapy A Case Study Approach 5th Edition Nelms Solutions ManualDocument36 pagesMedical Nutrition Therapy A Case Study Approach 5th Edition Nelms Solutions Manualwinifredmilcah4oo1100% (15)
- Top 10 Nutrient DeficienciesDocument37 pagesTop 10 Nutrient DeficienciesAlessaNo ratings yet
- A Systematic Review of The Effects of Residency Training On Patients OutcomesDocument11 pagesA Systematic Review of The Effects of Residency Training On Patients OutcomesMaik MouraNo ratings yet
- Cardio-Respiratory ArrestDocument3 pagesCardio-Respiratory ArrestluizaNo ratings yet
- PospapDocument3 pagesPospapGregorius Rahardyan HarveyogaNo ratings yet
- Treatment Center PDFDocument120 pagesTreatment Center PDFShellyNo ratings yet
- Mosquito Borne DiseasesDocument24 pagesMosquito Borne DiseasesSidney BowenNo ratings yet
- Professional Development Plan - EportfolioDocument4 pagesProfessional Development Plan - Eportfolioapi-429873538No ratings yet
- Noria Modelo 3020B TC 6Document64 pagesNoria Modelo 3020B TC 6Fernando Manuel MichligNo ratings yet
- Week 4 Ortho TestsDocument15 pagesWeek 4 Ortho Testsapi-468597987No ratings yet
- Activity 2 - Quiñones Mary Angela Felicia T - CPE 1 - Nov 3 - Prof Andy GutierrezDocument7 pagesActivity 2 - Quiñones Mary Angela Felicia T - CPE 1 - Nov 3 - Prof Andy GutierrezMary Angela Felicia QuiñonesNo ratings yet
- 13 KayachikitsaDocument2 pages13 KayachikitsaShreeNo ratings yet
- Plummer 2021Document6 pagesPlummer 2021Cristina CostaNo ratings yet
- ch02 (Lecture) - Workforce Safety and WellnessDocument63 pagesch02 (Lecture) - Workforce Safety and WellnessJomar TeofiloNo ratings yet
- Essential Guide to Workplace Investigations, The: A Step-By-Step Guide to Handling Employee Complaints & ProblemsFrom EverandEssential Guide to Workplace Investigations, The: A Step-By-Step Guide to Handling Employee Complaints & ProblemsRating: 3 out of 5 stars3/5 (2)
- Legal Writing in Plain English: A Text with ExercisesFrom EverandLegal Writing in Plain English: A Text with ExercisesRating: 3 out of 5 stars3/5 (2)
- Nolo's Encyclopedia of Everyday Law: Answers to Your Most Frequently Asked Legal QuestionsFrom EverandNolo's Encyclopedia of Everyday Law: Answers to Your Most Frequently Asked Legal QuestionsRating: 4 out of 5 stars4/5 (18)
- A Student's Guide to Law School: What Counts, What Helps, and What MattersFrom EverandA Student's Guide to Law School: What Counts, What Helps, and What MattersRating: 5 out of 5 stars5/5 (4)
- Torts: QuickStudy Laminated Reference GuideFrom EverandTorts: QuickStudy Laminated Reference GuideRating: 5 out of 5 stars5/5 (1)
- The Power of Our Supreme Court: How Supreme Court Cases Shape DemocracyFrom EverandThe Power of Our Supreme Court: How Supreme Court Cases Shape DemocracyRating: 5 out of 5 stars5/5 (2)
- Employment Law: a Quickstudy Digital Law ReferenceFrom EverandEmployment Law: a Quickstudy Digital Law ReferenceRating: 1 out of 5 stars1/5 (1)
- How to Make Patent Drawings: Save Thousands of Dollars and Do It With a Camera and Computer!From EverandHow to Make Patent Drawings: Save Thousands of Dollars and Do It With a Camera and Computer!Rating: 5 out of 5 stars5/5 (1)
- Flora and Vegetation of Bali Indonesia: An Illustrated Field GuideFrom EverandFlora and Vegetation of Bali Indonesia: An Illustrated Field GuideRating: 5 out of 5 stars5/5 (2)
- Dictionary of Legal Terms: Definitions and Explanations for Non-LawyersFrom EverandDictionary of Legal Terms: Definitions and Explanations for Non-LawyersRating: 5 out of 5 stars5/5 (2)
- Legal Forms for Starting & Running a Small Business: 65 Essential Agreements, Contracts, Leases & LettersFrom EverandLegal Forms for Starting & Running a Small Business: 65 Essential Agreements, Contracts, Leases & LettersNo ratings yet
- Admissibility of Expert Witness TestimonyFrom EverandAdmissibility of Expert Witness TestimonyRating: 5 out of 5 stars5/5 (1)
- So You Want to be a Lawyer: The Ultimate Guide to Getting into and Succeeding in Law SchoolFrom EverandSo You Want to be a Lawyer: The Ultimate Guide to Getting into and Succeeding in Law SchoolNo ratings yet
- LLC or Corporation?: Choose the Right Form for Your BusinessFrom EverandLLC or Corporation?: Choose the Right Form for Your BusinessRating: 3.5 out of 5 stars3.5/5 (4)
- Legal Writing in Plain English, Third Edition: A Text with ExercisesFrom EverandLegal Writing in Plain English, Third Edition: A Text with ExercisesNo ratings yet
- Legal Guide for Starting & Running a Small BusinessFrom EverandLegal Guide for Starting & Running a Small BusinessRating: 4.5 out of 5 stars4.5/5 (9)