You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Final Guide To Cbt-1Document199 pagesFinal Guide To Cbt-1Anderson Alfred93% (28)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Luborsky, Lester - Principles of Psychoanalytic Psychotherapy PDFDocument295 pagesLuborsky, Lester - Principles of Psychoanalytic Psychotherapy PDFMario Hernández Jr.No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- B2-Poohs Little Book of Feng ShuiDocument100 pagesB2-Poohs Little Book of Feng Shuiapi-3732743100% (4)
- Puff The Magic Dragon ScoreDocument1 pagePuff The Magic Dragon ScoreJules100% (1)
- Ghid de Calatorie Pentru HemofiliciDocument211 pagesGhid de Calatorie Pentru HemofiliciRegarde Le Ciel Ici0% (1)
- Operational PlanDocument10 pagesOperational PlanIan Mizzel A. Dulfina100% (3)
- Borderline Personality Disorder OverviewDocument1 pageBorderline Personality Disorder OverviewTomNo ratings yet
- Alienware-14 Owner's Manual En-UsDocument109 pagesAlienware-14 Owner's Manual En-UsAditya PatilNo ratings yet
- Pollen Filter Clio 11 Dci 1.5Document3 pagesPollen Filter Clio 11 Dci 1.5welder2011x1No ratings yet
- Adult Education 2016Document24 pagesAdult Education 2016TomNo ratings yet
- Whats Wrong With ANPR-No CCTV ReportDocument12 pagesWhats Wrong With ANPR-No CCTV ReportTomNo ratings yet
- 01 The Translation Process LessonDocument12 pages01 The Translation Process Lessonnicole_laetNo ratings yet
- Zelda - Ocarina MedleyDocument6 pagesZelda - Ocarina MedleyTomNo ratings yet
- 2009 Diptrans Seminar ChineseDocument32 pages2009 Diptrans Seminar ChineseTomNo ratings yet
- DSM I PDFDocument145 pagesDSM I PDFOrlando Alfonso Vázquez75% (4)
- Ukcat AnswersDocument6 pagesUkcat AnswersShivam PatelNo ratings yet
- SOS - Your Starter Guide To Mental HealthDocument36 pagesSOS - Your Starter Guide To Mental HealthTomNo ratings yet
- Freedom of Information Request - RFI20110278Document4 pagesFreedom of Information Request - RFI20110278TomNo ratings yet
- Lobotomy - The Brain Cutters ReturnDocument3 pagesLobotomy - The Brain Cutters ReturnTomNo ratings yet
- Welfare Policy PaperDocument29 pagesWelfare Policy PaperPiotr WójcickiNo ratings yet
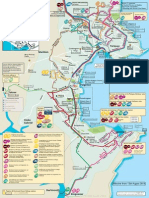
- Torbay Bus RoutesDocument1 pageTorbay Bus RoutesTomNo ratings yet
- Returning From Abroad InfoDocument26 pagesReturning From Abroad InfoTomNo ratings yet
- International Students and Part Time JobsDocument3 pagesInternational Students and Part Time Jobsharshan09No ratings yet
- FP3 TextbookDocument149 pagesFP3 TextbookJadeLovatic100% (2)
- 2013 Open Day ProgrammeDocument17 pages2013 Open Day ProgrammeTomNo ratings yet
- Aqa Mfp2 TextbookDocument156 pagesAqa Mfp2 TextbookWiktorJanusNo ratings yet
- GCE Mathematics (6360) Further Pure Unit 4 (MFP4)Document133 pagesGCE Mathematics (6360) Further Pure Unit 4 (MFP4)TomNo ratings yet
- Replacement of Missing Teeth With Fixed ProsthesesDocument5 pagesReplacement of Missing Teeth With Fixed ProsthesesTomNo ratings yet
- Implant Guidelines 20121009 - FINALDocument11 pagesImplant Guidelines 20121009 - FINALTomNo ratings yet
- Thatcher Ism, New Labour and The Walfare StateDocument40 pagesThatcher Ism, New Labour and The Walfare StateGroze BogdanNo ratings yet
- Claim Against Anup Joseph - HUB Legal Department US$19.00Document26 pagesClaim Against Anup Joseph - HUB Legal Department US$19.00Dr Romesh Arya ChakravartiNo ratings yet
- Manager: Spitalul Clinic Judeţean de Urgenţe "Sf. Spiridon" IaşiDocument1 pageManager: Spitalul Clinic Judeţean de Urgenţe "Sf. Spiridon" IaşiNelly-Georgiana MănăilăNo ratings yet
- Fims Case StudyDocument23 pagesFims Case StudyAKASH DAYAL100% (1)
- Prophylactic Cervical Cerclage (Modified Shirodkar Operation) For Twin and Triplet Pregnancies After Fertility TreatmentDocument8 pagesProphylactic Cervical Cerclage (Modified Shirodkar Operation) For Twin and Triplet Pregnancies After Fertility TreatmentAiraNo ratings yet
- Credentialing and Priviledging of Pharmacists: The UK PerspectiveDocument10 pagesCredentialing and Priviledging of Pharmacists: The UK PerspectiveFendy SipayungNo ratings yet
- Assessment NSG Diagnosis Goal Intervention Implementation EvaluationDocument2 pagesAssessment NSG Diagnosis Goal Intervention Implementation EvaluationMichelle ErikaNo ratings yet
- Medication Error TypesDocument19 pagesMedication Error TypesKamalakar KaramchetiNo ratings yet
- Class C - 1Document2 pagesClass C - 1Devi SetiawanNo ratings yet
- Medical Negligence RENEWEDDocument69 pagesMedical Negligence RENEWEDNAMRATA BHATIANo ratings yet
- 1 5 Middle Range TheoryDocument64 pages1 5 Middle Range TheoryMacey Malonzo0% (1)
- Alcohol Treatment Facility Business Plan FY-02Document7 pagesAlcohol Treatment Facility Business Plan FY-02Keith BeckerNo ratings yet
- Name: - Score: M - A - PE - H - Teacher: - DateDocument3 pagesName: - Score: M - A - PE - H - Teacher: - DateDarwin SolanoyNo ratings yet
- Omar ResumeDocument2 pagesOmar ResumeJbour OmarNo ratings yet
- A Proposed Grading System For Endovascular Treatment of Cerebral Arteriovenous Malformations - Buffalo Score PDFDocument9 pagesA Proposed Grading System For Endovascular Treatment of Cerebral Arteriovenous Malformations - Buffalo Score PDFRafael Mujica OreNo ratings yet
- 05thjan Assignment Abroad TimesDocument8 pages05thjan Assignment Abroad TimesSameer ShaikNo ratings yet
- Job Description - Deputy Nursing SuperintendentDocument5 pagesJob Description - Deputy Nursing SuperintendentSheen BelsylinNo ratings yet
- Contoh Application LetterDocument1 pageContoh Application LetterfennyNo ratings yet
- Theory of Comfort EnglishDocument15 pagesTheory of Comfort EnglishedoprimaNo ratings yet
- 12-Mother Teresa BiographtDocument65 pages12-Mother Teresa Biographtspark_123100% (2)
- Adamjee Panel Hospitals PDFDocument4 pagesAdamjee Panel Hospitals PDF00hanan100% (1)
- Latar Belakang PenelitianDocument22 pagesLatar Belakang PenelitiansyarifaNo ratings yet
- Shannon Troy: 362 Meadowbrook Ave Apt 1 Youngstown, OH 44512Document2 pagesShannon Troy: 362 Meadowbrook Ave Apt 1 Youngstown, OH 44512api-508597583No ratings yet
- APSIC BrochureDocument2 pagesAPSIC BrochurekindyNo ratings yet
- Overtime in NursingDocument5 pagesOvertime in NursingallisonNo ratings yet
- Uas Progsus (Oktober 2018) SoalDocument5 pagesUas Progsus (Oktober 2018) Soalyuliana perdiantiNo ratings yet
- Shadow and SolitudeDocument34 pagesShadow and SolitudeharrohhoraytNo ratings yet