You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Runyankore-Rukiga Dictionary Launch: President Yoweri Museveni's SpeechDocument28 pagesRunyankore-Rukiga Dictionary Launch: President Yoweri Museveni's SpeechThe New Vision50% (2)
- Recipes From The Perfect Scoop by David LebovitzDocument10 pagesRecipes From The Perfect Scoop by David LebovitzThe Recipe Club100% (7)
- JRC JFE-680 Instruct ManualDocument86 pagesJRC JFE-680 Instruct ManualMark Dominic FedericoNo ratings yet
- Immigrant Italian Stone CarversDocument56 pagesImmigrant Italian Stone Carversglis7100% (2)
- Cross Talk Details and RoutingDocument29 pagesCross Talk Details and RoutingRohith RajNo ratings yet
- Submitted - Manuscript - Red FontDocument20 pagesSubmitted - Manuscript - Red FontKartik DeshmukhNo ratings yet
- Study of Cardiovascular Manifestations in TreatmenDocument9 pagesStudy of Cardiovascular Manifestations in TreatmenKartik DeshmukhNo ratings yet
- "COVID Vaccine" Is Not The Excuse To Delay Adaptation To The "New Normal"Document4 pages"COVID Vaccine" Is Not The Excuse To Delay Adaptation To The "New Normal"Kartik DeshmukhNo ratings yet
- The Effectiveness of Small-Bore Intercostal CathetDocument6 pagesThe Effectiveness of Small-Bore Intercostal CathetKartik DeshmukhNo ratings yet
- Seasonal Variation in The Internet Searches For CaDocument24 pagesSeasonal Variation in The Internet Searches For CaKartik DeshmukhNo ratings yet
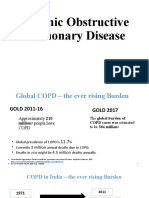
- Chronic Obstructive Pulmonary DiseaseDocument61 pagesChronic Obstructive Pulmonary DiseaseKartik DeshmukhNo ratings yet
- Role of Laparoscopy IN Acute Abdomen: Da Vinci GynecologyDocument5 pagesRole of Laparoscopy IN Acute Abdomen: Da Vinci GynecologyKartik DeshmukhNo ratings yet
- FRP Handrail Fittings CatalogDocument6 pagesFRP Handrail Fittings CatalogAl Adel MorenoNo ratings yet
- Shawal 1431 AH Prayer ScheduleDocument2 pagesShawal 1431 AH Prayer SchedulemasjidibrahimNo ratings yet
- Significance of GodboleDocument5 pagesSignificance of GodbolehickeyvNo ratings yet
- MarbiehistoryDocument6 pagesMarbiehistoryMarbie DalanginNo ratings yet
- Comparing Exponential NumbersDocument5 pagesComparing Exponential NumbersMaya RahayuNo ratings yet
- Gemh 108Document20 pagesGemh 108YuvrajNo ratings yet
- Assessment Questions: 1: Wash - Rinse and SanitizeDocument3 pagesAssessment Questions: 1: Wash - Rinse and SanitizeAna Margarita AycochoNo ratings yet
- Design and Development of Automatic Pneumatic Jack in Four Wheeler Ijariie5374Document5 pagesDesign and Development of Automatic Pneumatic Jack in Four Wheeler Ijariie5374Saravanan ViswakarmaNo ratings yet
- Curriculum Vitae - RadikaDocument3 pagesCurriculum Vitae - RadikaradikahendryNo ratings yet
- G.S 5Document2 pagesG.S 5Jamsher BalochNo ratings yet
- Schneider Pressure Switch XMLDocument2 pagesSchneider Pressure Switch XMLhaoNo ratings yet
- Why Are Solids Are Floating On My Secondary Clarifier - Biological Waste TreatmDocument6 pagesWhy Are Solids Are Floating On My Secondary Clarifier - Biological Waste TreatmIsaac FernándezNo ratings yet
- Assignment 2 Unit 20 Fully Completed - ReviewedDocument5 pagesAssignment 2 Unit 20 Fully Completed - Reviewedchris.orisawayiNo ratings yet
- Column, Slab, Footing and Wall Footing Foundations: Class A MixingDocument47 pagesColumn, Slab, Footing and Wall Footing Foundations: Class A MixingGioharry Nul PanambulanNo ratings yet
- Toshiba: ® A20SeriesDocument12 pagesToshiba: ® A20SeriesYangNo ratings yet
- Lec 4 - 4th WeekDocument40 pagesLec 4 - 4th Weekrajpoot aliNo ratings yet
- Mean Variance Portfolio TheoryDocument85 pagesMean Variance Portfolio TheoryEbenezerNo ratings yet
- TreesDocument69 pagesTreesADITYA GEHLAWATNo ratings yet
- Food Taste Panel Evaluation Form 2Document17 pagesFood Taste Panel Evaluation Form 2Akshat JainNo ratings yet
- Niir Integrated Organic Farming Handbook PDFDocument13 pagesNiir Integrated Organic Farming Handbook PDFNatalieNo ratings yet
- Seminar On Solar Mobile Charger: Submitted To: Submitted byDocument16 pagesSeminar On Solar Mobile Charger: Submitted To: Submitted byAkhila GottemukkulaNo ratings yet
- Fyp-Hydraulic Brakes CompleteDocument32 pagesFyp-Hydraulic Brakes CompleteRishabh JainNo ratings yet
- Oil Whirl and Whip Instabilities - Within Journal BearingsDocument27 pagesOil Whirl and Whip Instabilities - Within Journal BearingsTalha AamirNo ratings yet
- Goliath 90 v129 eDocument129 pagesGoliath 90 v129 eerkanNo ratings yet
- SPL Lab Report3Document49 pagesSPL Lab Report3nadif hasan purnoNo ratings yet