You might also like
- Enteral Nutrition (Gastrojejunotomy)Document30 pagesEnteral Nutrition (Gastrojejunotomy)Hairul IzlanNo ratings yet
- Enteral and Parenteral RoutesDocument3 pagesEnteral and Parenteral RoutesKarla Karina Dela CruzNo ratings yet
- Enteral Nutriton TherapyDocument5 pagesEnteral Nutriton TherapyJAMES ROD MARINDUQUENo ratings yet
- Alf (NCP)Document3 pagesAlf (NCP)timmisarmientoNo ratings yet
- MIDTERMS MS SL NGT TPN FeedingDocument7 pagesMIDTERMS MS SL NGT TPN FeedingMarie Cris SorianoNo ratings yet
- Gastroretentive Microballoons: A Novel Approach For Drug DeliveryDocument9 pagesGastroretentive Microballoons: A Novel Approach For Drug DeliveryprinceamitNo ratings yet
- Docusate Sodium (Colace)Document2 pagesDocusate Sodium (Colace)E100% (1)
- Enteral and Parenteral Feeding: Mylin G. Abalus NUTN 204 LecturerDocument24 pagesEnteral and Parenteral Feeding: Mylin G. Abalus NUTN 204 Lecturerminhmap90_635122804No ratings yet
- Bisacodyl (Dulcolax)Document1 pageBisacodyl (Dulcolax)ENo ratings yet
- Medication Administration Through Enteral Feeding Tubes: PrimerDocument11 pagesMedication Administration Through Enteral Feeding Tubes: PrimerAnna Karla Do Nascimento SouzaNo ratings yet
- Magnesium Hydroxide (Milk of Magnesia)Document1 pageMagnesium Hydroxide (Milk of Magnesia)ENo ratings yet
- COURSE TASK 15 - Herrera, Geraldine Mae F.Document3 pagesCOURSE TASK 15 - Herrera, Geraldine Mae F.Geraldine MaeNo ratings yet
- Drug Cards Milk of MagnesiaDocument1 pageDrug Cards Milk of MagnesiaAdrianne Bazo100% (1)
- Nutrisi EnteralDocument51 pagesNutrisi EnteralIsma Awalia Habibah14No ratings yet
- Drug Study SorbitolDocument2 pagesDrug Study SorbitolみずNo ratings yet
- Gastroretentive-Drug-Delivery-System L-13 L-59 L-67 L-01 L-46Document9 pagesGastroretentive-Drug-Delivery-System L-13 L-59 L-67 L-01 L-46Bilal AsgharNo ratings yet
- Part 2 Gastro New NotesDocument12 pagesPart 2 Gastro New NotesanreilegardeNo ratings yet
- Drug Study #3Document8 pagesDrug Study #3James Emman ClementeNo ratings yet
- 13Nutritional-Support LatestDocument76 pages13Nutritional-Support LatestKryzza LeizellNo ratings yet
- Gerd Maam Weng MingoyDocument1 pageGerd Maam Weng MingoyMingoy, CarlosNo ratings yet
- NCM 105 Lec Final NotesDocument3 pagesNCM 105 Lec Final Notescherryle whiteNo ratings yet
- Methods of Nutrient DeliveryDocument3 pagesMethods of Nutrient DeliveryFarmisa MannanNo ratings yet
- Nutritional Management of Gastrointestinal Tract Diseases of Dogs and CatsDocument7 pagesNutritional Management of Gastrointestinal Tract Diseases of Dogs and CatsLuciana ArauzNo ratings yet
- Enteral FeedingDocument16 pagesEnteral FeedingShane KasabovNo ratings yet
- Mira LaxDocument1 pageMira LaxCassieNo ratings yet
- A Review On Gastroretentive Drug Delivery SystemDocument10 pagesA Review On Gastroretentive Drug Delivery Systemharshita SinghNo ratings yet
- Enteral Nutrition Gastro LecDocument14 pagesEnteral Nutrition Gastro LecanreilegardeNo ratings yet
- Drug BisacodylDocument1 pageDrug BisacodylSrkocherNo ratings yet
- FiberCon (Polycarbophil)Document1 pageFiberCon (Polycarbophil)ENo ratings yet
- Anti - Diarrheal DrugsDocument5 pagesAnti - Diarrheal DrugsFitri NurullahNo ratings yet
- Drug Delivery On Rectal Absorption: Suppositories: Review ArticleDocument7 pagesDrug Delivery On Rectal Absorption: Suppositories: Review ArticleNindah IkaNo ratings yet
- Enteral NutritionDocument11 pagesEnteral NutritionPablo CauichNo ratings yet
- Laxatives and PugatiivesDocument4 pagesLaxatives and PugatiivesSultan Abdul Hamid IINo ratings yet
- Pro To NixDocument2 pagesPro To NixKatie McPeekNo ratings yet
- Floating Drug Delivery SystemDocument27 pagesFloating Drug Delivery SystemGANESH KUMAR JELLA100% (1)
- GrddsDocument6 pagesGrddsSrihith RoyNo ratings yet
- Tube Feeding Handouts 102819Document4 pagesTube Feeding Handouts 102819MariaNo ratings yet
- 83-Article Text-86-1-10-20180222 - 2Document6 pages83-Article Text-86-1-10-20180222 - 2Haider SalahNo ratings yet
- Atrovent (Ipratropium)Document1 pageAtrovent (Ipratropium)E100% (2)
- 2 Forms &routes of Drug AdminDocument38 pages2 Forms &routes of Drug AdminNathaniel PulidoNo ratings yet
- 2-Tables 1,2,3 and 4Document4 pages2-Tables 1,2,3 and 4mohammed zourobNo ratings yet
- Enteral Nutrition: Sana Inam Lecturer College of Pharmacy, GCUFDocument18 pagesEnteral Nutrition: Sana Inam Lecturer College of Pharmacy, GCUFAnum AzamNo ratings yet
- L5 - Special Medical NeedDocument38 pagesL5 - Special Medical NeedHailey ChengNo ratings yet
- Complication of Enteral Nutrition PDFDocument3 pagesComplication of Enteral Nutrition PDFIndra WijayaNo ratings yet
- COMMON TERMS IN GI TREATMENT MODALITIES Part 1Document11 pagesCOMMON TERMS IN GI TREATMENT MODALITIES Part 1Mikee PaningbatanNo ratings yet
- Nutri Final 1Document4 pagesNutri Final 1cajeshannahabigaelNo ratings yet
- NCP Acabo Hypokalemia 1Document2 pagesNCP Acabo Hypokalemia 1Doneva Lyn MedinaNo ratings yet
- Gastroretentive Drug Delivery System-Areview: January 2013Document17 pagesGastroretentive Drug Delivery System-Areview: January 2013Kumar GalipellyNo ratings yet
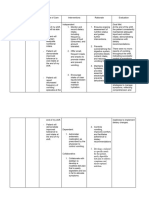
- Drug Doctor's Order Mechanism of Action Indications Contraindications Effects Nursing ConsiderationsDocument2 pagesDrug Doctor's Order Mechanism of Action Indications Contraindications Effects Nursing Considerationsnikki shein bullongNo ratings yet
- Smooth Muscle Spasm: Gastrointestinal TractDocument3 pagesSmooth Muscle Spasm: Gastrointestinal TractLei BrionesNo ratings yet
- NCP - Pott's DiseaseDocument23 pagesNCP - Pott's Diseasemhean azneitaNo ratings yet
- AirflowDocument1 pageAirflowRyan Marie CornellNo ratings yet
- NCP Materna2 NutriDocument2 pagesNCP Materna2 Nutrigoodemonz15No ratings yet
- Nutritional Management of Hospitalized Small AnimalsFrom EverandNutritional Management of Hospitalized Small AnimalsDaniel L. ChanNo ratings yet
- The Perfect Liquid Diet Cookbook:The Ultimate Nutrition Guide To Shedding Pounds, Powering Metabolism And Living Long With Delectable And Nourishing RecipesFrom EverandThe Perfect Liquid Diet Cookbook:The Ultimate Nutrition Guide To Shedding Pounds, Powering Metabolism And Living Long With Delectable And Nourishing RecipesNo ratings yet
- The 7 Important Intermittent Fasting Rules - Based On The Teachings Of Dr. Eric Berg: Unlocking The Power Of Intermittent FastingFrom EverandThe 7 Important Intermittent Fasting Rules - Based On The Teachings Of Dr. Eric Berg: Unlocking The Power Of Intermittent FastingNo ratings yet
- Jackylin Tan September 20Document1 pageJackylin Tan September 20api-3831131No ratings yet
- The Function of Elections in SingaporeDocument16 pagesThe Function of Elections in Singaporeapi-3831131No ratings yet
- Histor YDocument1 pageHistor Yapi-3831131No ratings yet
- FriendsterlayoutDocument2 pagesFriendsterlayoutapi-3831131No ratings yet
- Jackylin Tan1NU06May 15Document1 pageJackylin Tan1NU06May 15api-3831131No ratings yet
- Jackylin TanDocument1 pageJackylin Tanapi-3831131No ratings yet
- Ex Curs Us Nu 06Document5 pagesEx Curs Us Nu 06api-3831131100% (3)
- Histor YDocument1 pageHistor Yapi-3831131No ratings yet
- Final English!!!!Document24 pagesFinal English!!!!api-3831131No ratings yet
- Ex Curs Us Nu 06Document5 pagesEx Curs Us Nu 06api-3831131100% (3)
- Ani Me LayoutDocument3 pagesAni Me Layoutapi-3831131No ratings yet
- Xjacky LINXDocument2 pagesXjacky LINXapi-3831131No ratings yet
- What Is Historical MaterialismDocument22 pagesWhat Is Historical Materialismapi-3831131No ratings yet
- Nursing Review Bullet For Funda (-Credits To OWNER-)Document4 pagesNursing Review Bullet For Funda (-Credits To OWNER-)Camille Honeyleith Lanuza FernandoNo ratings yet
- ADN3-1 Digestive HP - 200 - Yang, Myung SookDocument37 pagesADN3-1 Digestive HP - 200 - Yang, Myung SookNorPhea - នភាNo ratings yet
- Checklist NGT - FinalDocument5 pagesChecklist NGT - FinalKim Tan100% (2)
- Petrus Nnolim CVDocument5 pagesPetrus Nnolim CVagni.nnolimNo ratings yet
- Gastric-Lavage-and-Gavage ReviewerDocument2 pagesGastric-Lavage-and-Gavage ReviewerPatricia AdiaoNo ratings yet
- Nasogastric (NG) Tube - Feeding Your ChildDocument3 pagesNasogastric (NG) Tube - Feeding Your ChildmaliniNo ratings yet
- Small Mammal, Exotic Animal and Wildlife Nursing PDFDocument28 pagesSmall Mammal, Exotic Animal and Wildlife Nursing PDFTheodora Novenna R CNo ratings yet
- Kozier's Peri Operative NSG ChecklistDocument15 pagesKozier's Peri Operative NSG ChecklistMichaelNo ratings yet
- Nasogastric TubeDocument11 pagesNasogastric TubeSoma Al-mutairiNo ratings yet
- Feeding PatientDocument10 pagesFeeding PatientHarish Kumar KumawatNo ratings yet
- Submission No. 5Document14 pagesSubmission No. 5Angela BronNo ratings yet
- CHN MCQ'''SSDocument19 pagesCHN MCQ'''SSrevathidadam55555No ratings yet
- NGT VillarealDocument5 pagesNGT VillarealDianne LabisNo ratings yet
- Feeding Helpless Patient Fundamental-1Document77 pagesFeeding Helpless Patient Fundamental-1Ibrahim Ahmed OsmanNo ratings yet
- ICU ReportDocument14 pagesICU Reportحسين علي سلطانNo ratings yet
- FREE NLE REVIEW Fundies and OthersDocument40 pagesFREE NLE REVIEW Fundies and OthersAngel Lopez100% (1)
- Nasogastric Tubes Insertion of NotesDocument4 pagesNasogastric Tubes Insertion of NotesJenny WongNo ratings yet
- Adult Nasogastric Tube Insertion Procedure & Management PolicyDocument0 pagesAdult Nasogastric Tube Insertion Procedure & Management PolicyRubelyn Joy LazarteNo ratings yet
- Renr Review Practice Test 3: Healthcare Services. What Is One of The Goals of Managed Care?Document9 pagesRenr Review Practice Test 3: Healthcare Services. What Is One of The Goals of Managed Care?Tk0% (1)
- Intake and Output MeasurementDocument6 pagesIntake and Output MeasurementWen RodsaNo ratings yet
- NGT Insertion 2022Document41 pagesNGT Insertion 2022Krishna Faith P. DelaraNo ratings yet
- Rectal FluidtherapyDocument7 pagesRectal FluidtherapyIan SabogalNo ratings yet
- IV InsertionDocument9 pagesIV InsertionSharmaine Grace FlorigNo ratings yet
- OSCE ProceduresDocument16 pagesOSCE ProceduresQueen ShNo ratings yet
- Medical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 40Document9 pagesMedical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 40sarasjunkNo ratings yet
- Nasogastric Tube (NGT)Document31 pagesNasogastric Tube (NGT)annyeong_123No ratings yet
- NGT LavageDocument16 pagesNGT LavageTina Alteran100% (1)
- N N T I R: Asogastric and Asoenteric Ube Nsertion and EmovalDocument8 pagesN N T I R: Asogastric and Asoenteric Ube Nsertion and EmovalFernanda AlfaroNo ratings yet
- IV To PO Conversion PolicyDocument4 pagesIV To PO Conversion PolicyIrham NiNo ratings yet
- Arizona Burncenter Guidelines PDFDocument20 pagesArizona Burncenter Guidelines PDFBuyungNo ratings yet