You might also like
- Pharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceFrom EverandPharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceRating: 3 out of 5 stars3/5 (1)
- Anderson & Townsend Preventing High-Alert Medication Errors in Hospitalized PatientsDocument6 pagesAnderson & Townsend Preventing High-Alert Medication Errors in Hospitalized PatientsCG0% (1)
- Drug Errors: Consequences, Mechanisms, and Avoidance: Key PointsDocument7 pagesDrug Errors: Consequences, Mechanisms, and Avoidance: Key PointsRavikiran SuryanarayanamurthyNo ratings yet
- PharmacovigilanceDocument45 pagesPharmacovigilancepavani valluriNo ratings yet
- Adverse Drug ReactionDocument3 pagesAdverse Drug ReactionTin SagmonNo ratings yet
- Interview Questions-PVDocument9 pagesInterview Questions-PVtausif100% (1)
- Introduction To Pharmacovigilance & Its Current Perspectives in PunjabDocument35 pagesIntroduction To Pharmacovigilance & Its Current Perspectives in PunjabAshar NasirNo ratings yet
- Moore RDocument7 pagesMoore RElaine IllescasNo ratings yet
- National Patient Safety GoalsDocument7 pagesNational Patient Safety GoalsyaniNo ratings yet
- Incidence, Characteristics, and Predictive Factors For Medication Errors in Paediatric Anaesthesia: A Prospective Incident Monitoring StudyDocument8 pagesIncidence, Characteristics, and Predictive Factors For Medication Errors in Paediatric Anaesthesia: A Prospective Incident Monitoring StudyShaikh ZarinNo ratings yet
- Pharmacovigilance Ensuring The Safe Use of MedicinesDocument18 pagesPharmacovigilance Ensuring The Safe Use of MedicinespopadrianionutzNo ratings yet
- JCI-Sentinel Event AlertDocument3 pagesJCI-Sentinel Event AlertDewi Ratna SariNo ratings yet
- Art 09Document9 pagesArt 09Francisca DonosoNo ratings yet
- PHARMACOVIGILANCEDocument28 pagesPHARMACOVIGILANCENosheen JavedNo ratings yet
- Impact of Pharmacist Interventions On Clinical Outcome and Cost Avoidance in A University Teaching HospitalDocument8 pagesImpact of Pharmacist Interventions On Clinical Outcome and Cost Avoidance in A University Teaching HospitalErick De La RosaNo ratings yet
- PV DefinitionsDocument6 pagesPV DefinitionsJhansi ReddyNo ratings yet
- International Patient Safety GoalsDocument30 pagesInternational Patient Safety GoalsMuvenn Kannan50% (2)
- Drug Incompatibilities in Intravenous Therapy Evaluation and Proposition of Preventive Tools in Intensive Care and Hematology UnitsDocument9 pagesDrug Incompatibilities in Intravenous Therapy Evaluation and Proposition of Preventive Tools in Intensive Care and Hematology UnitsGlory Claudia KarundengNo ratings yet
- Consumer ReportingDocument36 pagesConsumer ReportingJai RamNo ratings yet
- Journa Generall AneshesiaDocument7 pagesJourna Generall AneshesiaNadya NovianiNo ratings yet
- Aims and Applications: Aims: The Three Aims of Pharmacoepidemiology AreDocument10 pagesAims and Applications: Aims: The Three Aims of Pharmacoepidemiology Aregowtham0% (1)
- Emergency Drug Therapy DoneDocument4 pagesEmergency Drug Therapy DonelsshgriffinNo ratings yet
- Adverse Drug Reaction Monitoring Reporting PDFDocument3 pagesAdverse Drug Reaction Monitoring Reporting PDFRossana Rizqita PutriNo ratings yet
- Medication Error PDFDocument61 pagesMedication Error PDFChelsea Ritz MendozaNo ratings yet
- Med Errors OldDocument1 pageMed Errors OldAnonymous XvwKtnSrMRNo ratings yet
- Brief Notes On PharmacovigilanceDocument78 pagesBrief Notes On Pharmacovigilancejay100% (1)
- Introduction To PharmacovigillanceDocument93 pagesIntroduction To PharmacovigillanceRanjan Kumar MajhiNo ratings yet
- Introduction To Pharmacovigilance UNIT - 1Document58 pagesIntroduction To Pharmacovigilance UNIT - 1meghana vasNo ratings yet
- Day Care Anaesthesia With Ketamine V S Fentanyl A Comparative Study in Short Surgical ProceduresDocument9 pagesDay Care Anaesthesia With Ketamine V S Fentanyl A Comparative Study in Short Surgical ProceduresFuchsia ZeinNo ratings yet
- Introduction To PharmacovigillanceDocument93 pagesIntroduction To Pharmacovigillancefunnymemesworld2023No ratings yet
- Abhijath Documents Those Who Are Preparing For Interview 1664876843Document36 pagesAbhijath Documents Those Who Are Preparing For Interview 1664876843naidujNo ratings yet
- 4 High Alert Medication FinalDocument4 pages4 High Alert Medication Finalrini setyawatiNo ratings yet
- 2000-WHO Drug Information Vol. 14 - No. 4 PDFDocument79 pages2000-WHO Drug Information Vol. 14 - No. 4 PDFAngela Castro RNo ratings yet
- Evidenced Based (Bernardo, BSN - 3C)Document8 pagesEvidenced Based (Bernardo, BSN - 3C)Jerico CunananNo ratings yet
- Pharmacovigilance - Dr. Ganesh UchitDocument58 pagesPharmacovigilance - Dr. Ganesh UchitSshan ChaturvediNo ratings yet
- SMB5401Document288 pagesSMB5401funnymemesworld2023No ratings yet
- I Hi Trigger Tool For Measuring Adverse Drug EventsDocument16 pagesI Hi Trigger Tool For Measuring Adverse Drug EventsGaby ValenzuelaNo ratings yet
- Ad Hoc Data SourcesDocument11 pagesAd Hoc Data SourcesVINAY KUMARNo ratings yet
- Notes To PharmacovigilanceDocument58 pagesNotes To Pharmacovigilancejay100% (1)
- Ipsg # 2017 PDFDocument30 pagesIpsg # 2017 PDFDARRYLARANHA100% (1)
- Week2 Submitter PaperDocument3 pagesWeek2 Submitter Paperapi-299189797No ratings yet
- Spontenious Reporting SystemDocument3 pagesSpontenious Reporting SystemAyanNo ratings yet
- Adverse Reactions SlideshowDocument40 pagesAdverse Reactions SlideshowGary MaoNo ratings yet
- Farmacovigilancia RevisionDocument16 pagesFarmacovigilancia RevisionOfelia RomeroNo ratings yet
- For Partial Fulfilment of The Requirement For TheDocument45 pagesFor Partial Fulfilment of The Requirement For ThesalmanNo ratings yet
- Write - Up - Adhoc Data SourcesDocument12 pagesWrite - Up - Adhoc Data SourcesRaju BaiNo ratings yet
- P109primary Care For Persons Who Inject DrugsDocument8 pagesP109primary Care For Persons Who Inject Drugshossein kasiriNo ratings yet
- Irrational Use of DrugDocument9 pagesIrrational Use of Drugsreedam100% (2)
- Ro-Ils 1Document3 pagesRo-Ils 1api-529438966No ratings yet
- HPCP Assignment 2Document8 pagesHPCP Assignment 2mokshmshah492001No ratings yet
- Radiation Oncology Incident Learning System (ROILS) Cast StudyDocument4 pagesRadiation Oncology Incident Learning System (ROILS) Cast Studyapi-481226212No ratings yet
- Medication Errors: What They Are, How They Happen, and How To Avoid ThemDocument9 pagesMedication Errors: What They Are, How They Happen, and How To Avoid ThemMoisesNo ratings yet
- Pharma CO VigilanceDocument33 pagesPharma CO VigilanceSravani ReddyNo ratings yet
- Medication Safety: Improving Public HealthDocument6 pagesMedication Safety: Improving Public HealthViee Nie SfarmNo ratings yet
- Practices: in Patient CareDocument5 pagesPractices: in Patient Careahmad nuril hidayatNo ratings yet
- Pharmacovigilance - An Overview: Dr. Sukanta Sen MD, DNB, DM (Clin Pharmacology)Document31 pagesPharmacovigilance - An Overview: Dr. Sukanta Sen MD, DNB, DM (Clin Pharmacology)FranchescaAmoréBrodithe100% (1)
- Immunization Safety SurveillanceDocument14 pagesImmunization Safety SurveillanceHIRA DASNo ratings yet
- The Prevention of Intrathecal Medictionl Errors Woods K Department of Health UK 2001 PDFDocument24 pagesThe Prevention of Intrathecal Medictionl Errors Woods K Department of Health UK 2001 PDFArturo RuizNo ratings yet
- Recs 071317 OpioidsDocument4 pagesRecs 071317 OpioidsKuzivakwasheNo ratings yet
- Search BMJ GroupDocument23 pagesSearch BMJ GroupCharles BrooksNo ratings yet
- Recommendation From Renee AbdellaDocument2 pagesRecommendation From Renee Abdellaapi-244230664No ratings yet
- PPPPC Meeting Minutes 071614Document5 pagesPPPPC Meeting Minutes 071614api-244230664No ratings yet
- Signed Final Evaluation 2014Document3 pagesSigned Final Evaluation 2014api-244230664No ratings yet
- Recommendation From Jamie NordhagenDocument1 pageRecommendation From Jamie Nordhagenapi-244230664No ratings yet
- Thank You Patient 1Document2 pagesThank You Patient 1api-244230664No ratings yet
- Kudos Email 8 25 13Document2 pagesKudos Email 8 25 13api-244230664No ratings yet
- Focuspdca 7 26 14Document2 pagesFocuspdca 7 26 14api-244230664No ratings yet
- Kudos Email 1 13 14Document1 pageKudos Email 1 13 14api-244230664No ratings yet
- Pain Severity Satisfaction With Pain ManagementDocument10 pagesPain Severity Satisfaction With Pain Managementapi-244230664No ratings yet
- Kudos Email 8 2 14Document1 pageKudos Email 8 2 14api-244230664No ratings yet
- Ce Record 2014 Aurora Davis v2Document1 pageCe Record 2014 Aurora Davis v2api-244230664No ratings yet
- Advisor Checklist CompletedDocument7 pagesAdvisor Checklist Completedapi-244230664No ratings yet
- Kudos Email 10 11 13Document1 pageKudos Email 10 11 13api-244230664No ratings yet
- Kudos Email 3 29 14Document1 pageKudos Email 3 29 14api-244230664No ratings yet
- Thank You New Grad 1Document2 pagesThank You New Grad 1api-244230664No ratings yet
- Preceptor Council AttendanceDocument2 pagesPreceptor Council Attendanceapi-244230664No ratings yet
- Lo6 FeedbackDocument2 pagesLo6 Feedbackapi-244230664No ratings yet
- January Staff Meeting MinutesDocument3 pagesJanuary Staff Meeting Minutesapi-244230664No ratings yet
- Preceptor Council AttendanceDocument2 pagesPreceptor Council Attendanceapi-244230664No ratings yet
- Cancer Patients Barriers To Pain ManagementDocument12 pagesCancer Patients Barriers To Pain Managementapi-244230664No ratings yet
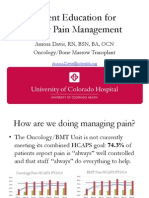
- Presentation of Pain Patient Education ToolDocument10 pagesPresentation of Pain Patient Education Toolapi-244230664No ratings yet
- PSC Meeting Agenda 4 2014Document1 pagePSC Meeting Agenda 4 2014api-244230664No ratings yet
- Do Patients Beliefs Act As BarriersDocument13 pagesDo Patients Beliefs Act As Barriersapi-244230664No ratings yet
- Pain Minutes 031914Document2 pagesPain Minutes 031914api-244230664No ratings yet
- Email From Mandy 7 14 14Document1 pageEmail From Mandy 7 14 14api-244230664No ratings yet
- A Pain Education ProgrammeDocument13 pagesA Pain Education Programmeapi-244230664No ratings yet
- Cancer Pain Part 2Document7 pagesCancer Pain Part 2api-244230664No ratings yet
- Hcahps Omg Data BeforeDocument1 pageHcahps Omg Data Beforeapi-244230664No ratings yet
- Hcahps BMT Data BeforeDocument1 pageHcahps BMT Data Beforeapi-244230664No ratings yet
- Daisy Nomination Bill ValentineDocument2 pagesDaisy Nomination Bill Valentineapi-244230664No ratings yet
- Cryptosporidiosis in ChickensDocument7 pagesCryptosporidiosis in ChickensŠhâh NawazNo ratings yet
- PDEA S Register 2-14 FormDocument12 pagesPDEA S Register 2-14 FormAngelito BALUYOT JRNo ratings yet
- Desi Elage: High Cholestrol Level in Blood (Khoon Main Cholesterol Ka Level Barh Jae)Document7 pagesDesi Elage: High Cholestrol Level in Blood (Khoon Main Cholesterol Ka Level Barh Jae)Irshad HussainNo ratings yet
- Health PromotionDocument10 pagesHealth PromotionReyta NoorNo ratings yet
- Basic Life Support (BLS)Document49 pagesBasic Life Support (BLS)Sukhbir KaurNo ratings yet
- Felix Widal TestDocument9 pagesFelix Widal TestGaluhAlvianaNo ratings yet
- CPG Management of Hypertension (4th Edition)Document98 pagesCPG Management of Hypertension (4th Edition)ssfdsNo ratings yet
- Radiotherapy NursingDocument35 pagesRadiotherapy NursingMarlon Rey AnacletoNo ratings yet
- MAPEH 7 Q4 Week 4Document9 pagesMAPEH 7 Q4 Week 4Maricris ArsibalNo ratings yet
- Chapter37 Assessment and Management of Patients With Allergic DisordersDocument40 pagesChapter37 Assessment and Management of Patients With Allergic Disordersjericho dinglasanNo ratings yet
- EC Certificate - Production Quality Assurance EC Certificate - Production Quality AssuranceDocument6 pagesEC Certificate - Production Quality Assurance EC Certificate - Production Quality AssuranceEngr Hamid AliNo ratings yet
- Post-Operative Fever EditDocument52 pagesPost-Operative Fever EditDebsNo ratings yet
- Chagrin Factor - Feinstein1985Document3 pagesChagrin Factor - Feinstein1985Rafael MartinsNo ratings yet
- Preoperative Physiology, Imaging, andDocument13 pagesPreoperative Physiology, Imaging, andSiLfia SahrinNo ratings yet
- Teaching Students With Autism Spectrum DisordersDocument155 pagesTeaching Students With Autism Spectrum DisordersAnonymous Pj6Odj0% (1)
- General HospitaDocument273 pagesGeneral HospitaAbcdNo ratings yet
- Active and Passive Euthanasia Thesis StatementDocument7 pagesActive and Passive Euthanasia Thesis StatementDoMyPaperForMeSingapore100% (2)
- Risk Factors For Venous and Arterial ThrombosisDocument19 pagesRisk Factors For Venous and Arterial ThrombosisM Buyung MusliminNo ratings yet
- Comparative Study of Episiotomy Repair Absorbable Synthetic Versus Chromic Catgut Suture MaterialDocument5 pagesComparative Study of Episiotomy Repair Absorbable Synthetic Versus Chromic Catgut Suture MaterialamilyapraditaNo ratings yet
- AllianzDocument27 pagesAllianzHariz SyahmiNo ratings yet
- PhysioEx9,1: Exercise 7 Activity 2: PEX-07-02Document8 pagesPhysioEx9,1: Exercise 7 Activity 2: PEX-07-02mishael_baig100% (11)
- DialysisDocument21 pagesDialysisReygie MarsadaNo ratings yet
- Discharge PlanDocument1 pageDischarge PlanGail GenturalezNo ratings yet
- A3 ReportDocument4 pagesA3 ReportmfernandNo ratings yet
- Evaluation of The R One Robotic System For Percutaneous Coronary Intervention THDocument11 pagesEvaluation of The R One Robotic System For Percutaneous Coronary Intervention THNeranga SamaratungeNo ratings yet
- Name of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesDocument2 pagesName of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesKarl Lourenz DeysolongNo ratings yet
- NUTRILITE Apple Jujube WheatPeptide enDocument27 pagesNUTRILITE Apple Jujube WheatPeptide enNoris Eka Raudzah IshakNo ratings yet
- Hospital Management System: By, C.Arun Kumar S.Dinesh V.Dinesh S.Gowtham S.HarijayanthDocument16 pagesHospital Management System: By, C.Arun Kumar S.Dinesh V.Dinesh S.Gowtham S.Harijayanthneeraj-singh-6543No ratings yet
- AnswersDocument47 pagesAnswersOriyomi OdekunleNo ratings yet
- Mortality Incidence Sociodemographic and Clinical Data in COVID19 PatientsDocument1,365 pagesMortality Incidence Sociodemographic and Clinical Data in COVID19 PatientsSoumodeep SenNo ratings yet
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- The Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItFrom EverandThe Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItRating: 4.5 out of 5 stars4.5/5 (107)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Redefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackFrom EverandRedefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackRating: 4.5 out of 5 stars4.5/5 (152)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)
- A Profession Without Reason: The Crisis of Contemporary Psychiatry—Untangled and Solved by Spinoza, Freethinking, and Radical EnlightenmentFrom EverandA Profession Without Reason: The Crisis of Contemporary Psychiatry—Untangled and Solved by Spinoza, Freethinking, and Radical EnlightenmentNo ratings yet
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeFrom EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeRating: 5 out of 5 stars5/5 (559)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (250)
- Anxious for Nothing: Finding Calm in a Chaotic WorldFrom EverandAnxious for Nothing: Finding Calm in a Chaotic WorldRating: 4.5 out of 5 stars4.5/5 (1245)
- Insecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItFrom EverandInsecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItRating: 4.5 out of 5 stars4.5/5 (84)
- How to Be Miserable: 40 Strategies You Already UseFrom EverandHow to Be Miserable: 40 Strategies You Already UseRating: 4.5 out of 5 stars4.5/5 (57)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouFrom EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNo ratings yet
- The Anatomy of Loneliness: How to Find Your Way Back to ConnectionFrom EverandThe Anatomy of Loneliness: How to Find Your Way Back to ConnectionRating: 4.5 out of 5 stars4.5/5 (162)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- 50 Ways to Rewire Your Anxious Brain: Simple Skills to Soothe Anxiety and Create New Neural Pathways to CalmFrom Everand50 Ways to Rewire Your Anxious Brain: Simple Skills to Soothe Anxiety and Create New Neural Pathways to CalmNo ratings yet