You might also like
- Dummy ReportDocument29 pagesDummy ReportnaquiahoNo ratings yet
- Lo3 Artifact - Micro-Counseling Skills Midterm ReflectionDocument6 pagesLo3 Artifact - Micro-Counseling Skills Midterm Reflectionapi-543749170No ratings yet
- Zaki & Williams (2013) - Interpersonal Emotion RegulationDocument9 pagesZaki & Williams (2013) - Interpersonal Emotion Regulationalessarpon7557No ratings yet
- Evaluation of A Social Skills Program Using Art Therapy PDFDocument10 pagesEvaluation of A Social Skills Program Using Art Therapy PDFLNo ratings yet
- Growth and Development: Infancy Early Childhood Middle Childhood AdolescentDocument42 pagesGrowth and Development: Infancy Early Childhood Middle Childhood AdolescentJohn Ervin AgenaNo ratings yet
- Autism Spectrum Disorder Fact Sheet-1Document2 pagesAutism Spectrum Disorder Fact Sheet-1api-354686297No ratings yet
- Interventions For Classroom DisruptionDocument54 pagesInterventions For Classroom DisruptionnosunarNo ratings yet
- Genograms and EcomapsDocument8 pagesGenograms and EcomapsDevan DaveNo ratings yet
- Mob BehaviourDocument8 pagesMob BehaviourPradipta Mukherjee100% (1)
- FM Mental Health BrochureDocument2 pagesFM Mental Health BrochureKaitlyn RichardsNo ratings yet
- Classification of Feeding and Eating DisordersDocument13 pagesClassification of Feeding and Eating DisordersMagito JayaNo ratings yet
- Chapter 20 - Culturally Adaptive InterviewingDocument94 pagesChapter 20 - Culturally Adaptive InterviewingNaomi LiangNo ratings yet
- The Supervisory Relationship Questionnaire (SRQ)Document3 pagesThe Supervisory Relationship Questionnaire (SRQ)kartuteNo ratings yet
- The Bodys Response To Processing Emotion PDFDocument22 pagesThe Bodys Response To Processing Emotion PDFMaría Regina Castro CataldiNo ratings yet
- Paper 2 Compassion FatigueDocument4 pagesPaper 2 Compassion Fatigueapi-401934380No ratings yet
- 2016 Resilience, Risk, Mental Health and Well-Being Associations and Conceptual DifferencesDocument9 pages2016 Resilience, Risk, Mental Health and Well-Being Associations and Conceptual DifferencesDorin CascavalNo ratings yet
- Sample Literature Review - PsychologyDocument9 pagesSample Literature Review - Psychologyapi-242012614No ratings yet
- Pedagogies of Strategic Empathy: Navigating Through The Emotional Complexities of Anti-Racism in Higher EducationDocument14 pagesPedagogies of Strategic Empathy: Navigating Through The Emotional Complexities of Anti-Racism in Higher Educationapi-247542954100% (1)
- Compassion FatigueDocument5 pagesCompassion Fatigueapi-384261910No ratings yet
- Parent Stress Index With Instructions - 11-28-11Document2 pagesParent Stress Index With Instructions - 11-28-11Sumit SinghNo ratings yet
- Group Therapy PDFDocument2 pagesGroup Therapy PDFma maNo ratings yet
- Eating Disorders:: Anorexia Nervosa (AN)Document5 pagesEating Disorders:: Anorexia Nervosa (AN)kgjtertij100% (1)
- Theory of Mind: An Observational ReportDocument3 pagesTheory of Mind: An Observational ReportMalavika MenonNo ratings yet
- Work Effectively in Trauma Informed CareDocument20 pagesWork Effectively in Trauma Informed CareCharlie HaddadNo ratings yet
- Group Counseling Informed Consent For ParentsDocument1 pageGroup Counseling Informed Consent For Parentsapi-239096806No ratings yet
- Emotional Regulation Training For Intensive and Critical Care NursesDocument9 pagesEmotional Regulation Training For Intensive and Critical Care NursesvipereejayNo ratings yet
- Dissociative Identity Disorder in ArtDocument5 pagesDissociative Identity Disorder in ArtsiancampbellNo ratings yet
- Sport, Disordered Eating & Eating DisordersDocument6 pagesSport, Disordered Eating & Eating DisordersChris ParkerNo ratings yet
- Children and GriefDocument3 pagesChildren and GriefRommel Villaroman EstevesNo ratings yet
- Autism Spectrum Disorder Friendly School Guidelines 2016Document11 pagesAutism Spectrum Disorder Friendly School Guidelines 2016Pudu MounikaNo ratings yet
- Addressing Absenteeism Through A Positive Reinforcement InterventionDocument51 pagesAddressing Absenteeism Through A Positive Reinforcement InterventionMARJUN BARTOLO100% (1)
- Supporting Students With Challenging BehaviorsDocument4 pagesSupporting Students With Challenging Behaviorsapi-357465278No ratings yet
- Emotional CPR - AustraliaDocument1 pageEmotional CPR - AustraliaSharon A Stocker0% (1)
- Early Regression in Social Communication in Autism Spectrum Disorders: A CPEA Study (Luyster Et Al 2005)Document26 pagesEarly Regression in Social Communication in Autism Spectrum Disorders: A CPEA Study (Luyster Et Al 2005)info-TEANo ratings yet
- Healing Through PlayDocument2 pagesHealing Through PlayEunice KhainzaNo ratings yet
- Personality Factors of Teachers of Autistic StudentsDocument59 pagesPersonality Factors of Teachers of Autistic Studentswork4you2No ratings yet
- CBT Paper Final BerryDocument18 pagesCBT Paper Final Berryapi-284381567No ratings yet
- Facilitating Social Inclusion of Children with AutismDocument16 pagesFacilitating Social Inclusion of Children with AutismZAHRUDIN ZAHIRUDDIN DAUD Moe100% (1)
- The Children's Eating Behavior InventoryDocument14 pagesThe Children's Eating Behavior Inventoryguilherme augusto paroNo ratings yet
- Anger Management InterventionsDocument10 pagesAnger Management InterventionsAsih Nor ZahidahNo ratings yet
- Final Paper AsdDocument24 pagesFinal Paper Asdapi-410097887No ratings yet
- Article Taming The Terrible MomentsDocument3 pagesArticle Taming The Terrible Momentsapi-232349586No ratings yet
- Development and validation of the General Activities of Daily Living ScaleDocument10 pagesDevelopment and validation of the General Activities of Daily Living ScaleCarlos Eduardo NorteNo ratings yet
- Coping strategies and factors in parents of children with autismDocument18 pagesCoping strategies and factors in parents of children with autismandrea lopezNo ratings yet
- 16PF GuideDocument17 pages16PF GuidesmacujaNo ratings yet
- The Effectiveness of Play Therapy On Reduction ofDocument6 pagesThe Effectiveness of Play Therapy On Reduction ofHira Khan100% (1)
- Brochure !Document2 pagesBrochure !api-291329856No ratings yet
- Ed Autisminc PDFDocument76 pagesEd Autisminc PDFAndres Rafael Rangel GonzalezNo ratings yet
- Modified Coventry Model - Including PDA ProfileDocument13 pagesModified Coventry Model - Including PDA ProfileAliens-and-antsNo ratings yet
- Youngmee Kim - Gender in Psycho-Oncology (2018, Oxford University Press, USA)Document263 pagesYoungmee Kim - Gender in Psycho-Oncology (2018, Oxford University Press, USA)Dian Oktaria SafitriNo ratings yet
- Children Appreciation Test (CAT) : HistoryDocument17 pagesChildren Appreciation Test (CAT) : Historysadia RashidNo ratings yet
- Emotional Development from Childhood to AdolescenceDocument27 pagesEmotional Development from Childhood to AdolescenceSherli PNo ratings yet
- Clinical GuidelineDocument86 pagesClinical GuidelineJae MedinaNo ratings yet
- CBTi vs. Sleeping PillsDocument1 pageCBTi vs. Sleeping PillssamzNo ratings yet
- Cognitive, Sensory, and Emotional Changes Associated With The Menstrual Cycle PDFDocument10 pagesCognitive, Sensory, and Emotional Changes Associated With The Menstrual Cycle PDFadrianNo ratings yet
- Youth Trauma Fact SheetDocument2 pagesYouth Trauma Fact Sheetapi-494901707No ratings yet
- Challenges Faced by Families of Autistic Children-153 PDFDocument5 pagesChallenges Faced by Families of Autistic Children-153 PDFRidhoyanti HNo ratings yet
- Destructive Myths in Family Therapy: How to Overcome Barriers to Communication by Seeing and Saying -- A Humanistic PerspectiveFrom EverandDestructive Myths in Family Therapy: How to Overcome Barriers to Communication by Seeing and Saying -- A Humanistic PerspectiveNo ratings yet
- Collaborative Problem Solving: An Evidence-Based Approach to Implementation and PracticeFrom EverandCollaborative Problem Solving: An Evidence-Based Approach to Implementation and PracticeAlisha R. PollastriNo ratings yet
- Harm to Others: The Assessment and Treatment of DangerousnessFrom EverandHarm to Others: The Assessment and Treatment of DangerousnessNo ratings yet
- Remmitance Padala Fee: Amount From Amount To Applicable Service FeeDocument1 pageRemmitance Padala Fee: Amount From Amount To Applicable Service Feealtarboy_mdNo ratings yet
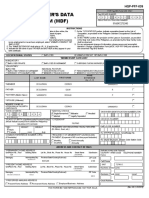
- Member'S Data Form (MDF) : HQP-PFF-039Document2 pagesMember'S Data Form (MDF) : HQP-PFF-039altarboy_mdNo ratings yet
- Logic Multiple Choice Q and As (FACILITATOR)Document5 pagesLogic Multiple Choice Q and As (FACILITATOR)Neha KalraNo ratings yet
- PsychoanalysisDocument14 pagesPsychoanalysisaltarboy_mdNo ratings yet
- Guilty PleasureDocument24 pagesGuilty Pleasurealtarboy_mdNo ratings yet
- 2016 0120 BridgetteDocument1 page2016 0120 Bridgettealtarboy_mdNo ratings yet
- ReadmeDocument1 pageReadmeChadel DbholezNo ratings yet
- SonaDocument14 pagesSonaaltarboy_mdNo ratings yet
- Awolusi Social Networking WoDocument6 pagesAwolusi Social Networking Woaltarboy_mdNo ratings yet
- Pink OilDocument1 pagePink Oilaltarboy_mdNo ratings yet
- The 200 Best Small Companies in America: 18. MSCIDocument1 pageThe 200 Best Small Companies in America: 18. MSCIaltarboy_mdNo ratings yet
- 7 Ways Ro Use Rewards To Fix EmployeesDocument2 pages7 Ways Ro Use Rewards To Fix Employeesaltarboy_md100% (2)
- Liquidation For Xmas PresentationDocument1 pageLiquidation For Xmas Presentationaltarboy_mdNo ratings yet
- Christmas Party 2013 LiquidationDocument1 pageChristmas Party 2013 Liquidationaltarboy_mdNo ratings yet
- ABP ChildrenDocument1 pageABP Childrenaltarboy_mdNo ratings yet
- Epic definition: A long narrative poemDocument3 pagesEpic definition: A long narrative poemaltarboy_mdNo ratings yet
- Integrative Counseling ApproachDocument6 pagesIntegrative Counseling Approachaltarboy_md100% (1)
- Questionnaire of Work Life BalanceDocument2 pagesQuestionnaire of Work Life BalancePratik Khimani100% (3)
- IdiomsDocument8 pagesIdiomsPearl PMNo ratings yet
- Work Life BalanceDocument32 pagesWork Life Balancealtarboy_mdNo ratings yet
- Sss Web Inquiry SystemDocument1 pageSss Web Inquiry Systemaltarboy_md0% (1)
- Criminology 1Document2 pagesCriminology 1altarboy_mdNo ratings yet
- Reaction Paper For HerculesDocument1 pageReaction Paper For Herculesaltarboy_md100% (3)
- Relapse Prevention PlanningDocument4 pagesRelapse Prevention PlanningYungston100% (3)
- 3 R Framework For Early Childhood Learningin The Pandemic Era and BeyondDocument21 pages3 R Framework For Early Childhood Learningin The Pandemic Era and BeyondIJAR JOURNALNo ratings yet
- Millions Suffering From Depression in PH - Doh, WhoDocument4 pagesMillions Suffering From Depression in PH - Doh, WhoAda Mikaela CañeteNo ratings yet
- Ap Psychology Group Project MotivationDocument1 pageAp Psychology Group Project Motivationapi-333631531No ratings yet
- Understanding-Ocd 2016 v2Document27 pagesUnderstanding-Ocd 2016 v2Samanjit Sen Gupta100% (1)
- Merdard BossDocument5 pagesMerdard BossjkmilNo ratings yet
- EMDR E-Manual - 103pagsDocument103 pagesEMDR E-Manual - 103pagsPaula Cruz100% (1)
- Child Centered Treatment Planning FormDocument5 pagesChild Centered Treatment Planning FormCurieNo ratings yet
- India's view of mental healthDocument20 pagesIndia's view of mental healthagni.No ratings yet
- Non Insti FinalDocument7 pagesNon Insti FinalJames BoundNo ratings yet
- Cognitive Therapy For PTSD: Mood Anxiety and Personality Clinical Academic Group (CAG)Document110 pagesCognitive Therapy For PTSD: Mood Anxiety and Personality Clinical Academic Group (CAG)Leon YangNo ratings yet
- ADHD: Clinical Practice Guideline For The Diagnosis, Evaluation, and TreatmentDocument18 pagesADHD: Clinical Practice Guideline For The Diagnosis, Evaluation, and TreatmentBen CulpepperNo ratings yet
- Rational EmotiveDocument12 pagesRational EmotiveAntigoni DarvNo ratings yet
- A Good Time To Dance A Mixed-Methods Approach of The Effects of Dance Movement Therapy For Breast Cancer Patients During and After RadiotherapyDocument10 pagesA Good Time To Dance A Mixed-Methods Approach of The Effects of Dance Movement Therapy For Breast Cancer Patients During and After RadiotherapysetautoNo ratings yet
- PsycheDocument3 pagesPsycheChlodette Eizl M. LaurenteNo ratings yet
- Baguio ordinance proposes mental health policyDocument8 pagesBaguio ordinance proposes mental health policyKenneth AcostaNo ratings yet
- Personal Transformation: From Addiction To FreedomDocument3 pagesPersonal Transformation: From Addiction To FreedomLeslie FiegerNo ratings yet
- The Physical Self SummaryDocument4 pagesThe Physical Self SummaryMarilynNo ratings yet
- Original PDF Social Work An Empowering Profession 9th EditionDocument61 pagesOriginal PDF Social Work An Empowering Profession 9th Editionfrank.woodard901100% (36)
- 5 Ways To Build Confidence in A Child With ADD/ADHDDocument3 pages5 Ways To Build Confidence in A Child With ADD/ADHDwildflowerNo ratings yet
- Family Satisfaction Scale (FSS) : David H. Olson, Ph.D. I. Overview of Family SatisfactionDocument9 pagesFamily Satisfaction Scale (FSS) : David H. Olson, Ph.D. I. Overview of Family SatisfactionElena BuduroiNo ratings yet
- What Is Psychology?: Behavioral NeuroscienceDocument3 pagesWhat Is Psychology?: Behavioral Neurosciencenylana marceNo ratings yet
- Monografia Mutismo SelectivoDocument12 pagesMonografia Mutismo SelectivoFabiana FerelekNo ratings yet
- Facts & Statistics - Anxiety and Depression Association of America, ADAADocument7 pagesFacts & Statistics - Anxiety and Depression Association of America, ADAAasdflkjNo ratings yet
- Somatoform Disorders: NUR 444 FALL 2015Document37 pagesSomatoform Disorders: NUR 444 FALL 2015Amit TamboliNo ratings yet
- Chestionar Eating Disorders FairburnDocument5 pagesChestionar Eating Disorders FairburnSergiu VescanNo ratings yet
- FIND THE RIGHT DISTRESS TOLERANCE SKILL FOR YOUR SITUATIONDocument1 pageFIND THE RIGHT DISTRESS TOLERANCE SKILL FOR YOUR SITUATIONSasha-Lee KrielNo ratings yet
- Music Therapy Techniques As Predictors of Change in Mental Health CareDocument9 pagesMusic Therapy Techniques As Predictors of Change in Mental Health CareIra TryNo ratings yet
- Borderline Symptom List BLS 23Document2 pagesBorderline Symptom List BLS 23Cé García100% (1)
- A Case of Anorexia Nervosa in A Preadolescent MaleDocument4 pagesA Case of Anorexia Nervosa in A Preadolescent MaleSUPRAKASH CHAUDHURYNo ratings yet