Professional Documents
Culture Documents
Physical and Language
Uploaded by
abcd205Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Physical and Language
Uploaded by
abcd205Copyright:
Available Formats
Physical
and
Languag
e
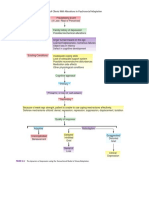
Emotional Social
Birth
to
1
month
Feedings: 5-8 per
daySleep: 20 hrs
per daySensory
Capacities: makes
basic distinctions in
vision, hearing,
smelling, tasting,
touch, temperature,
and perception of
pain
Generalized
Tension
Helpless
Asocial
Fed by mother
2
months
to
3
months
Sensory
Capacities: color
perception, visual
exploration, oral
exploration.Sounds
: cries, coos,
gruntsMotor Ability:
control of eye
muscles, lifts head
when on stomach.
Delight
Distress Smiles at a Face
Visually fixates at a
face, smiles at a face,
may be soothed by
rocking.
4
months
to
6
months
Sensory
Capacities:
localizes
soundsSounds:
babbling, makes
most vowels and
about half of the
consonantsFeeding
s: 3-5 per day
Motor Ability:
control of head and
Enjoys being
cuddled
Recognizes his
mother. Distinguishes
between familiar
persons and
strangers, no longer
smiles
indiscriminately.Expe
cts feeding, dressing,
and bathing.
arm movements,
purposive grasping,
rolls over.
7
months
to
9
months
Motor Ability:
control of trunk and
hands, sits without
support, crawls
about.
Specific emotional
attachment to
mother.
Protests separation
from mother. Enjoys
peek-a-boo
10
months
to
12
months
Motor Ability:
control of legs and
feet, stands,
creeps, apposition
of thumb and fore-
finger.Language:
says one or two
words, imitates
sounds, responds
to simple
commands.Feedin
gs: 3 meals, 2
snacksSleep: 12
hours, 2 naps
Anger
AffectionFear of
strangersCuriosity,
exploration
Responsive to own
name.Wave bye-
bye.Plays pat-a-cake,
understands no-
no!Gives and takes
objects.
1 years
to
1
years
Motor Ability:
creeps up stairs,
walks (10-20 min),
makes lines on
paper with crayon.
Dependent
Behavior
Very upset when
separated
from motherFear of
Bath
Obeys limited
commands.Repeats a
few words.Interested
in his mirror
image.Feeds himself.
1
years
to
2 years
Motor Ability: runs,
kicks a ball, builds
6 cube tower (2yrs)
Capable of bowel
and bladder
control.Language:
vocabulary of more
Temper tantrums
(1-3yrs)
Resentment of new
baby Does opposite
of what he is told (18
months).
than 200
wordsSleep: 12
hours at night, 1-2
hr nap
2 years
to
3 years
Motor Ability: jumps
off a step, rides a
tricycle, uses
crayons, builds a 9-
10 cube
tower.Language:
starts to use short
sentences controls
and explores world
with language,
stuttering may
appear briefly. Fear
of separation
Negativistic (2
yrs)Violent
emotions,
angerDifferentiates
facial expressions of
anger, sorrow, and
joy.Sense of humor
(Plays tricks)
Talks, uses I me
youCopies parents
actions.Dependent,
clinging, possessive
about toys, enjoys
playing alongside
another
child.Negativism (2
yrs).Resists parental
demands.Gives
orders.
Rigid insistence on
sameness of routine.
Inability to make
decisions.
3 years
to
4 years
Motor Ability:
Stands on one leg,
jumps up and
down, draws a
circle and a cross
(4 yrs)
Self-sufficient in
many routines of
home life.
Affectionate toward
parents.Pleasure in
genital
manipulationRoman
tic attachment to
parent of opposite
sex
(3 to 5 yrs)Jealousy
of same-sex
parent.Imaginary
fears of dark, injury,
etc. (3 to 5 years)
Likes to share, uses
weCooperative play
with other children,
nursery school.
Imitates
parents.Beginning of
identification with
same-sex parent,
practices sex-role
activities. Intense
curiosity & interest in
other childrens
bodies.Imaginary
friend.
4 years
to
Motor ability:
mature motor
Responsibility and
guiltFeels pride in
Prefers to play with
other children,
5 years control, skips,
broad jumps,
dresses himself,
copies a square
and a
triangle.Language:
talks clearly, uses
adult speech
sounds, has
mastered basic
grammar, relates a
story, knows over
2,000 words
(5 yrs)
accomplishment becomes competitive
prefers sex-
appropriate activities
Child development
From Wikipedia, the free encyclopedia
Jump to: navigation, search
For other uses, see Child development (disambiguation).
This article needs more medical
references for verification or relies too heavily on primary
sources. Please review the contents of the article and add
the appropriate references if you can. Unsourced or poorly
sourced material may be removed. (August 2012)
Exploring
Child development refers to the biological, psychological and emotional changes
that occur in human beings between birth and the end of adolescence, as the
individual progresses from dependency to increasingautonomy. It is a continuous
process with a predictable sequence yet having a unique course for every child. It
does not progress at the same rate and each stage is affected by the preceding types
of development. Because these developmental changes may be strongly influenced
by genetic factors and events during prenatal life, genetics and prenatal
development are usually included as part of the study of child development.
Related terms include developmental psychology, referring to development
throughout the lifespan, and pediatrics, the branch of medicine relating to the care
of children. Developmental change may occur as a result of genetically-controlled
processes known as maturation,
[1]
or as a result of environmental factors and
learning, but most commonly involves an interaction between the two. It may also
occur as a result of human nature and our ability to learn from our environment.
There are various definitions of periods in a child's development, since each period
is a continuum with individual differences regarding start and ending.
Some age-related development periods and examples of defined intervals
are: newborn (ages 04 weeks); infant (ages 4 weeks 1 year); toddler (ages 13
years); preschooler (ages 46 years); school-aged child (ages 613
years); adolescent (ages 1319).
[2]
However, organizations like Zero to Three and
the World Association for Infant Mental Health use the term infant as a broad
category, including children from birth to age 3.
Promoting child development through parental training, among other factors,
promotes excellent rates of child development, parental training as the Parental
Empowerment Program for Infant-PEPDI-
[3]
. The optimal development of
children is considered vital to society and so it is important to understand the
social, cognitive, emotional, and educational development of children. Increased
research and interest in this field has resulted in new theories and strategies, with
specific regard to practice that promotes development within the school system. In
addition there are also some theories that seek to describe a sequence of states that
compose child development.
Approximate outline of development periods in child development.
Contents
[hide]
1 Theories
o 1.1 Ecological systems theory
o 1.2 Piaget
1.2.1 Piaget stages
o 1.3 Vygotsky
o 1.4 Attachment theory
o 1.5 Erik Erikson
o 1.6 Behavioral theories
o 1.7 Other theories
2 Continuity and discontinuity in development
o 2.1 Mechanisms of development
3 Research issues and methods
4 Developmental milestones
5 Aspects of child development
o 5.1 Physical growth
5.1.1 Speed and pattern of development
5.1.2 Mechanisms of developmental change
5.1.3 Individual variation versus disease
o 5.2 Motor development
5.2.1 Definition
5.2.2 Speed and pattern of development
5.2.3 Mechanisms of motor development
5.2.4 Individual differences
5.2.5 Children with disabilities
5.2.6 Population differences
o 5.3 Cognitive/intellectual development
5.3.1 What develops?
5.3.2 Mechanisms of cognitive development
5.3.3 Individual differences
5.3.4 Population differences
o 5.4 Social-emotional development
5.4.1 What develops?
5.4.2 Speed and pattern of development
5.4.3 Mechanisms of social and emotional development
5.4.4 Individual differences
5.4.5 Population differences
o 5.5 Language
5.5.1 What develops?
5.5.2 Speed and pattern of development
5.5.3 Mechanisms of language development
o 5.6 Individual differences
5.6.1 Environmental causes
5.6.2 Neurological causes
6 Risk factors for poor child development
o 6.1 Postnatal depression
o 6.2 Maternal cocaine abuse
o 6.3 Malnutrition
6.3.1 Nutrients
o 6.4 Socioeconomic status
o 6.5 Parasites
o 6.6 Poisoning
o 6.7 Other factors
7 See also
8 References
9 Further reading
10 External links
Theories[edit]
Ecological systems theory[edit]
Main article: Ecological systems theory
Also called "development in context" or "human ecology" theory, ecological
systems theory, originally formulated by Urie Bronfenbrenner specifies four types
of nested environmental systems, with bi-directional influences within and
between the systems. The four systems are microsystem, mesosystem, exosystem,
and macrosystem. Each system contains roles, norms and rules that can powerfully
shape development. Since its publication in 1979, Bronfenbrenner's major
statement of this theory, The Ecology of Human Development
[4]
has had
widespread influence on the way psychologists and others approach the study of
human beings and their environments. As a result of this influential
conceptualization of development, these environments from the family to
economic and political structures have come to be viewed as part of the life
course from childhood through adulthood.
[5]
Piaget[edit]
Main articles: Jean Piaget and Piaget's theory of cognitive development
Jean Piaget was a Swiss scholar who began his studies in intellectual development
in the 1920s. Piagets first interests were those that dealt with the ways in which
animals adapt to their environments and his first scientific article about this subject
was published when he was 10 years old. This eventually led him to pursue a Ph.D.
in Zoology, which then led him to his second interest in
epistemology.]
[6]
Epistemology branches off from philosophy and deals with the
origin of knowledge. Piaget believed the origin of knowledge came from
Psychology, so he traveled to Paris and began working on the first standardized
intelligence test at Alfred Binet laboratories, this influenced his career greatly. As
he carried out this intelligence testing he began developing a profound interest in
the way childrens intellectualism works. As a result, he developed his own
laboratory and spent years recording childrens intellectual growth and attempted
to find out how children develop through various stages of thinking. This led to
Piaget develop four important stages of cognitive development: sensorimotor stage
(birth to age 2), preoperational stage (age 2 to 7), concrete-operational stage (ages
7 to 12), and formal-operational stage (ages 11 to 12, and thereafter).
[6]
Piaget stages[edit]
Sensorimotor: (birth to about age 2)
According to Piaget, when an infant reaches about 79 months of age they begin to
develop what he called object permanence, this means the child now has the ability
to understand that objects keep existing even when they cannot be seen. An
example of this would be hiding the childs favorite toy under a blanket, although
the child cannot physically see it they still know to look under the blanket.
Preoperational: (begins about the time the child starts to talk to about age 7)
During this stage of development, young children begin analyzing their
environment using mental symbols. These symbols often include words and
images and the child will begin to apply these various symbols in their everyday
lives as they come across different objects, events, and situations.
[6]
However,
Piagets main focus on this stage and the reason why he named it preoperational
is because children at this point are not able to apply specific cognitive operations,
such as mental math. In addition to symbolism, children now begin engaging in
pretend play where they begin pretending to be people they are not (teachers,
superheros), and they may use different props to make this pretend play more
real.
[6]
Some deficiencies in this stage of development are that children who are
about 34 years old often display what is called egocentrism, which means the
child is not able to see someone elses point of view, they feel as if every other
person is experiencing the same events and feelings that they are experiencing.
However, at about at 7 thought processes of children are no longer egocentric and
are more intuitive, meaning they now think about the way something looks instead
of rational thinking.
[6]
Concrete: (about first grade to early adolescence)
During this stage, children begin developing cognitive operations and begin
applying this new thinking to different events they may encounter.
[6]
Unlike the
preoperational stage, children can now change and rearrange mental images and
symbols to form a logical thought, an example of this is reversibility in which the
child now has the ability to reverse an action just by doing the opposite.
[6]
Formal operations:
The final stage of Piagets cognitive development defines a child as now having
the ability to think more rationally and systematically about abstract concepts and
hypothetical events.
[6]
Some positive aspects during this time is that child or
adolescent begins forming their identity and begin understanding why people
behave the way they behave. However, there are also some negative aspects which
include the child or adolescent developing some egocentric thoughts which include
the imaginary audience and the personal fable.
[6]
An imaginary audience is when
an adolescent feels that the world is just as concerned and judgmental of anything
the adolescent does as they are, an adolescent may feel as is they are on stage
and everyone is a critique and they are the ones being critiqued.
[6]
A personal fable
is when the adolescent feels that he or she is unique person and everything they do
is unique. They feel as if they are the only ones that have ever experienced what
they are experiencing and that they are invincible and nothing bad will happen to
them it will only happen to others.
[6]
Vygotsky[edit]
Main articles: Lev Vygotsky and Cultural-historical psychology
Vygotsky was a Russian theorist, who proposed the sociocultural theory. During
the 1920s1930s while Piaget was developing his own theory, Vygotsky was an
active scholar and at that time his theory was said to be recent because it was
translated out of Russian language and began influencing Western thinking.
[6]
He
posited that children learn through hands-on experience, as Piaget suggested.
However, unlike Piaget, he claimed that timely and sensitive intervention by adults
when a child is on the edge of learning a new task (called the zone of proximal
development) could help children learn new tasks. This technique is called
"scaffolding," because it builds upon knowledge children already have with new
knowledge that adults can help the child learn.
[7]
An example of this might be
when a parent "helps" an infant clap or roll her hands to the pat-a-cake rhyme, until
she can clap and roll her hands herself.
[8][9]
Vygotsky was strongly focused on the role of culture in determining the child's
pattern of development.
[7]
He argued that "Every function in the child's cultural
development appears twice: first, on the social level, and later, on the individual
level; first, between people (interpsychological) and then inside the child
(intrapsychological). This applies equally to voluntary attention, to logical
memory, and to the formation of concepts. All the higher functions originate as
actual relationships between individuals."
[7]
Vygotsky felt that development was a process and saw periods of crisis in child
development during which there was a qualitative transformation in the child's
mental functioning.
[10]
Attachment theory[edit]
Main article: Attachment theory
Attachment theory, originating in the work of John Bowlby and developed
by Mary Ainsworth, is a psychological, evolutionary and ethological theory that
provides a descriptive and explanatory framework for understanding interpersonal
relationships between human beings. Bowlbys observations of close attachments
led him to believe that close emotional bonds or attachments between an infant
and their primary caregiver is an important requirement that is necessary to form
normal social and emotional development.
[6]
Erik Erikson[edit]
Main articles: Erik Erikson and Psychosocial development
Erikson, a follower of Freud's, synthesized both Freud's and his own theories to
create what is known as the "psychosocial" stages of human development, which
span from birth to death, and focuses on "tasks" at each stage that must be
accomplished to successfully navigate life's challenges.
[11]
Erikson's eight stages consist of the following:
Trust vs. mistrust (infant)
Autonomy vs. shame (toddlerhood)
Initiative vs. guilt (preschooler)
Industry vs. inferiority (young adolescent)
Identity vs. role confusion (adolescent)
Intimacy vs. isolation (young adulthood)
Generativity vs. stagnation (middle adulthood)
Ego integrity vs. despair (old age)
[12]
Behavioral theories[edit]
Main article: Behavior analysis of child development
John B. Watsons behaviorism theory forms the foundation of the behavioral
model of development 1925.
[13]
He wrote extensively on child development and
conducted research (see Little Albert experiment). Watson was instrumental in the
modification of William James stream of consciousness approach to construct a
stream of behavior theory.
[citation needed]
Watson also helped bring a natural science
perspective to child psychology by introducing objective research methods based
on observable and measurable behavior.
[citation needed]
Following Watsons lead, B.F.
Skinner further extended this model to cover operant conditioning and verbal
behavior
[citation needed]
. Skinner used the operant chamber, or Skinner box, to observe
the behavior of small organisms in a controlled situation and proved that
organisms' behaviors are impacted on the environment. Furthermore, he used
reinforcement and punishment to shape in desired behavior.
Other theories[edit]
In accordance with his view that the sexual drive is a basic human
motivation,
[citation needed]
Sigmund Freud developed a psychosexual theory of human
development from infancy onward, divided into five stages.
[citation needed]
Each stage
centered around the gratification of the libido within a particular area, or erogenous
zone, of the body.
[citation needed]
He also argued that as humans develop, they become
fixated on different and specific objects through their stages of development.
[citation
needed]
Each stage contains conflict which requires resolution to enable the child to
develop.
[14]
The use of dynamical systems theory as a framework for the consideration of
development began in the early 1990s and has continued into the present
century.
[15]
Dynamic systems theory stresses nonlinear connections (e.g., between
earlier and later social assertiveness) and the capacity of a system to reorganize as
a phase shift that is stage-like in nature. Another useful concept for
developmentalists is the attractor state, a condition (such as teething or stranger
anxiety) that helps to determine apparently unrelated behaviors as well as related
ones.
[citation needed]
Dynamic systems theory has been applied extensively to the study
of motor development; the theory also has strong associations with some of
Bowlby's views about attachment systems. Dynamic systems theory also relates to
the concept of the transactional process,
[16]
a mutually interactive process in which
children and parents simultaneously influence each other, producing
developmental change in both over time.
[citation needed]
The "core knowledge perspective" is an evolutionary theory in child development
that proposes "infants begin life with innate, special-purpose knowledge systems
referred to as core domains of thought"
[17]
There are five core domains of thought,
each of which is crucial for survival, which simultaneously prepare us to develop
key aspects of early cognition; they are: physical, numerical, linguistic,
psychological, and biological.
[citation needed]
Continuity and discontinuity in development[edit]
Although the identification of developmental milestones is of interest to
researchers and to children's caregivers, many aspects of developmental change are
continuous and do not display noticeable milestones of change.
[18]
Continuous
developmental changes, like growth in stature, involve fairly gradual and
predictable progress toward adult characteristics. When developmental change is
discontinuous, however, researchers may identify not only milestones of
development, but related age periods often called stages. A stage is a period of
time, often associated with a known chronological age range, during which a
behavior or physical characteristic is qualitatively different from what it is at other
ages. When an age period is referred to as a stage, the term implies not only this
qualitative difference, but also a predictable sequence of developmental events,
such that each stage is both preceded and followed by specific other periods
associated with characteristic behavioral or physical qualities.
[19]
Stages of development may overlap or be associated with specific other aspects of
development, such as speech or movement. Even within a particular developmental
area, transition into a stage may not mean that the previous stage is completely
finished. For example, in Erikson's discussion of stages of personality, this theorist
suggests that a lifetime is spent in reworking issues that were originally
characteristic of a childhood stage.
[20]
Similarly, the theorist of cognitive
development, Piaget, described situations in which children could solve one type of
problem using mature thinking skills, but could not accomplish this for less
familiar problems, a phenomenon he called horizontal decalage.
[21]
Mechanisms of development[edit]
Girl playing in a play ground
See also: Nature versus nurture
Although developmental change runs parallel with chronological age,
[22]
age itself
cannot cause development.
[22]
The basic mechanisms or causes of developmental
change are genetic factors and environmental factors.
[23]
Genetic factors are
responsible for cellular changes like overall growth, changes in proportion of body
and brain parts,
[24]
and the maturation of aspects of function such as vision and
dietary needs.
[22]
Because genes can be "turned off" and "turned on",
[22]
the
individual's initial genotype may change in function over time, giving rise to
further developmental change. Environmental factors affecting development may
include both diet and disease exposure, as well as social, emotional, and cognitive
experiences.
[22]
However, examination of environmental factors also shows that
young human beings can survive within a fairly broad range of environmental
experiences.
[21]
Rather than acting as independent mechanisms, genetic and environmental factors
often interact to cause developmental change.
[22]
Some aspects of child
development are notable for their plasticity, or the extent to which the direction of
development is guided by environmental factors as well as initiated by genetic
factors.
[22]
When an aspect of development is strongly affected by early experience,
it is said to show a high degree of plasticity; when the genetic make-up is the
primary cause of development, plasticity is said to be low.
[25]
Plasticity may
involve guidance by endogenous factors like hormones as well as by exogenous
factors like infection.
[22]
Child playing with bubbles
One kind of environmental guidance of development has been described as
experience-dependent plasticity, in which behavior is altered as a result of learning
from the environment. Plasticity of this type can occur throughout the lifespan and
may involve many kinds of behavior, including some emotional reactions.
[22]
A
second type of plasticity, experience-expectant plasticity, involves the strong effect
of specific experiences during limited sensitive periods of development.
[22]
For
example, the coordinated use of the two eyes, and the experience of a single three-
dimensional image rather than the two-dimensional images created by light in each
eye, depend on experiences with vision during the second half of the first year of
life.
[22]
Experience-expectant plasticity works to fine-tune aspects of development
that cannot proceed to optimum outcomes as a result of genetic factors working
alone.
[26][27]
In addition to the existence of plasticity in some aspects of development, genetic-
environmental correlations may function in several ways to determine the mature
characteristics of the individual. Genetic-environmental correlations are
circumstances in which genetic factors make certain experiences more likely to
occur.
[22]
For example, in passive genetic-environmental correlation, a child is
likely to experience a particular environment because his or her parents' genetic
make-up makes them likely to choose or create such an environment.
[22]
In
evocative genetic-environmental correlation, the child's genetically-caused
characteristics cause other people to respond in certain ways, providing a different
environment than might occur for a genetically-different child;
[22]
for instance, a
child with Down syndrome may be treated more protectively and less
challengingly than a non-Down child.
[22]
Finally, an active genetic-environmental
correlation is one in which the child chooses experiences that in turn have their
effect;
[22]
for instance, a muscular, active child may choose after-school sports
experiences that create increased athletic skills, but perhaps preclude music
lessons. In all of these cases, it becomes difficult to know whether child
characteristics were shaped by genetic factors, by experiences, or by a combination
of the two.
[28]
Research issues and methods[edit]
1. What develops? What relevant aspects of the individual change over a
period of time?
2. What are the rate and speed of development?
3. What are the mechanisms of development what aspects of experience
and heredity cause developmental change?
4. Are there typical individual differences in the relevant developmental
changes?
5. Are there population differences in this aspect of development (for
example, differences in the development of boys and of girls)?
Empirical research that attempts to answer these questions may follow a number of
patterns. Initially, observational research in naturalistic conditions may be needed
to develop a narrative describing and defining an aspect of developmental change,
such as changes in reflex reactions in the first year.
[citation needed]
This type of work
may be followed by correlational studies, collecting information about
chronological age and some type of development such as vocabulary growth;
correlational statistics can be used to state change. Such studies examine the
characteristics of children at different ages.
[citation needed]
These methods may involve
longitudinal studies, in which a group of children are re-examined on a number of
occasions as they get older,or cross-sectional studies, in which groups of children
of different ages are tested once and compared with each other, or there may be a
combination of these approaches. Some child development studies examine the
effects of experience or heredity by comparing characteristics of different groups
of children in a necessarily non-randomized design.
[citation needed]
Other studies can
use randomized designs to compare outcomes for groups of children who receive
different interventions or educational treatments.
[21]
Developmental milestones[edit]
Main article: Child development stages
Milestones are changes in specific physical and mental abilities (such as walking
and understanding language) that mark the end of one developmental period and
the beginning of another.
[citation needed]
For stage theories, milestones indicate a stage
transition. Studies of the accomplishment of many developmental tasks have
established typical chronological ages associated with developmental milestones.
However, there is considerable variation in the achievement of milestones, even
between children with developmental trajectories within the typical range. Some
milestones are more variable than others; for example, receptive speech indicators
do not show much variation among children with typical hearing, but expressive
speech milestones can be quite variable.
[citation needed]
A common concern in child development is developmental delay involving a delay
in an age-specific ability for important developmental milestones. Prevention of
and early intervention in developmental delay are significant topics in the study of
child development.
[citation needed]
Developmental delays should be diagnosed by
comparison with characteristic variability of a milestone, not with respect to
average age at achievement. An example of a milestone would be eye-hand
coordination, which includes a child's increasing ability to manipulate objects in a
coordinated manner. Increased knowledge of age-specific milestones allows
parents and others to keep track of appropriate development.
[citation needed]
Aspects of child development[edit]
Child development is not a matter of a single topic, but progresses somewhat
differently for different aspects of the individual. Here are descriptions of the
development of a number of physical and mental characteristics.
[citation needed]
Physical growth[edit]
Physical growth in stature and weight occurs over the 1520 years following birth,
as the individual changes from the average weight of 3.5 kg and length of 50 cm
at full term birth to full adult size. As stature and weight increase, the
individual's proportions also change, from the relatively large head and
small torso and limbs of the neonate, to the adult's relatively small head and long
torso and limbs.
[29]
The childs pattern of growth is in a head-to-toe direction, or
cephalocaudal, and in an inward to outward pattern (center of the body to the
peripheral) called proximodistal.
Speed and pattern of development[edit]
The speed of physical growth is rapid in the months after birth, then slows, so birth
weight is doubled in the first four months, tripled by age 12 months, but not
quadrupled until 24 months.
[citation needed]
Growth then proceeds at a slow rate until
shortly before puberty (between about 9 and 15 years of age), when a period of
rapid growth occurs.
[citation needed]
Growth is not uniform in rate and timing across all
body parts. At birth, head size is already relatively near to that of an adult, but the
lower parts of the body are much smaller than adult size. In the course of
development, then, the head grows relatively little, and torso and limbs undergo a
great deal of growth.
[29]
Mechanisms of developmental change[edit]
Genetic factors play a major role in determining the growth rate, and particularly
the changes in proportion characteristic of early human development. However,
genetic factors can produce the maximum growth only if environmental conditions
are adequate. Poor nutrition and frequent injury and disease can reduce the
individual's adult stature, but the best environment cannot cause growth to a greater
stature than is determined by heredity.
[29]
Individual variation versus disease[edit]
Individual differences in height and weight during childhood are considerable.
Some of these differences are due to family genetic factors, others to
environmental factors, but at some points in development they may be strongly
influenced by individual differences in reproductive maturation.
[29]
The American Association of Clinical Endocrinologists defines short stature as
height more than 2 standard deviations below the mean for age and gender, which
corresponds to the shortest 2.3% of individuals.
[30]
In contrast, failure to thrive is
usually defined in terms of weight, and can be evaluated either by a low weight for
the child's age, or by a low rate of increase in the weight.
[31]
A similar term, stunted
growth, generally refers to reduced growth rate as a manifestation
of malnutrition in early childhood.
Motor development[edit]
A child while learning to walk
Abilities for physical movement change through childhood from the largely
reflexive (unlearned, involuntary) movement patterns of the young infant to the
highly skilled voluntary movements characteristic of later childhood and
adolescence.
Definition[edit]
"Motor learning refers to the increasing spatial and temporal accuracy of
movements with practice".
[32]
Motor skills can be divided into two categories: first
as basic skills necessary for everyday life and secondly, as recreational skills such
as skills for employment or certain specialties based on interest.
Speed and pattern of development[edit]
The speed of motor development is rapid in early life, as many of the reflexes of
the newborn alter or disappear within the first year, and slows later. Like physical
growth, motor development shows predictable patterns of cephalocaudal (head to
foot) and proximodistal (torso to extremities) development, with movements at the
head and in the more central areas coming under control before those of the lower
part of the body or the hands and feet. Types of movement develop in stage-like
sequences;
[citation needed]
for example, locomotion at 68 months involves creeping on
all fours, then proceeds to pulling to stand, "cruising" while holding on to an
object, walking while holding an adult's hand, and finally walking
independently.
[citation needed]
Older children continue the sequence by walking
sideways or backward, galloping, hopping, skipping with one foot and walking
with the other, and finally skipping.
[citation needed]
By middle childhood and
adolescence, new motor skills are acquired by instruction or observation rather
than in a predictable sequence.
[18]
There are Executive Functions of the brain
(working memory, timing measure of inhibition and switching) which are
important to motor skills.critiques the order of Executive Functioning leads to
Motor Skills, suggesting Motor Skills can support Executive Functioning in the
brain.
Mechanisms of motor development[edit]
The mechanisms involved in motor development involve some genetic components
that determine the physical size of body parts at a given age, as well as aspects of
muscle and bone strength.
[citation needed]
The main areas of the brain involved in
motor skills are the frontal cortex, parietal cortex and basal ganglia.
The dorsolateral frontal cortex is responsible for strategic processing. The parietal
cortex is important in controlling perceptual-motor integration and the basal
ganglia and supplementary motor cortex are responsible for motor sequences.
Nutrition and exercise also determine strength and therefore the ease and accuracy
with which a body part can be moved.
[18]
Flexibility is also impacted by nutrition
and exercise as well.
[33]
It has also been shown that the frontal lobe develops
posterio-anteriorally (from back to front). This is significant in motor development
because the hind portion of the frontal lobe is known to control motor functions.
This form of development is known as "Portional Development" and explains why
motor functions develop relatively quickly during typical childhood development,
while logic, which is controlled by the middle and front portions of the frontal
lobe, usually will not develop until late childhood and early
adolescence.
[34]
Opportunities to carry out movements help establish the abilities to
flex (move toward the trunk) and extend body parts, both capacities are necessary
for good motor ability. Skilled voluntary movements such as passing objects from
hand to hand develop as a result of practice and learning.
[18]
Mastery Climate is a
suggested successful learning environment for children to promote motor skills by
their own motivation. This promotes participation and active learning in children,
which according to Piaget's theory of cognitive development is extremely
important in early childhood rule.
Individual differences[edit]
Typical individual differences in motor ability are common and depend in part on
the child's weight and build. However, after the infant period, typical individual
differences are strongly affected by opportunities to practice, observe, and be
instructed on specific movements. Atypical motor development such as
persistent primitive reflexes beyond 46 months or delayed walking may be an
indication of developmental delays or problems such as autism, cerebral palsy,
or down syndrome .
[18]
Lower motor coordination results in difficulties with speed
accuracy and trade-off in complex tasks.
Children with disabilities[edit]
Children with Down syndrome or Developmental coordination disorder are late to
reach major motor skills milestones. A few examples of these milestones are
sucking, grasping, rolling, sitting up and walking, talking. Children with Down
syndrome sometimes have heart problems, frequent ear infections, hypotonia, or
undeveloped muscle mass. This syndrome is caused by
atypical chromosomal development.
Population differences[edit]
Regardless of the culture a baby is born into, they are born with a few core
domains of knowledge. These principals allow him or her to make sense of their
environment and learn upon previous experience by using motor skills such as
grasping or crawling. There are some population differences in motor
development, with girls showing some advantages in small muscle usage,
including articulation of sounds with lips and tongue.
[citation needed]
Ethnic differences
in reflex movements of newborn infants have been reported, suggesting that some
biological factor is at work.
[citation needed]
Cultural differences may encourage
learning of motor skills like using the left hand only for sanitary purposes and the
right hand for all other uses, producing a population difference.
[citation needed]
Cultural
factors are also seen at work in practiced voluntary movements such as the use of
the foot to dribble a soccer ball or the hand to dribble a basketball.
[18]
Cognitive/intellectual development[edit]
This section
requires expansion.(June
2008)
Cognitive Development is primarily concerned with ways in which infants and
children acquire, develop, and use internal mental capabilities such as problem
solving, memory and language.
What develops?[edit]
The capacity to learn, remember, and symbolise information, and to
solve problems, exists at a simple level in young infants, who can perform
cognitive tasks such as discriminating animate and inanimate beings or recognizing
small numbers of objects.
[citation needed]
During childhood, learning and information-
processing increase in speed, memory becomes increasingly longer, and symbol
use and the capacity for abstraction develop until a near-adult level is reached
by adolescence.
[18]
Mechanisms of cognitive development[edit]
Cognitive development has genetic and other biological mechanisms, as is seen in
the many genetic causes of intellectual disability.
[citation needed]
Environmental factors
including food and nutrition, responsiveness of parents, daily experiences, physical
activity and love can influence early brain development of children.
[35]
However,
although it is assumed that brain functions cause cognitive events, it has not been
possible to measure specific brain changes and show that they cause cognitive
change.
[citation needed]
Developmental advances in cognition are also related to
experience and learning, and this is particularly the case for higher-level abilities
like abstraction, which depend to a considerable extent on formal education.
[18]
Individual differences[edit]
There are typical individual differences in the ages at which specific cognitive
abilities are achieved,
[citation needed]
but schooling for children in industrialized
countries is based on the assumption that these differences are not large.
[citation
needed]
Atypical delays in cognitive development are problematic for children in
cultures that demand advanced cognitive skills for work and for independent
living.
[18]
Population differences[edit]
There are few population differences in cognitive development.
[citation needed]
Boys
and girls show some differences in their skills and preferences, but there is a great
deal of overlap between the groups.
[citation needed]
Differences in cognitive
achievement of different ethnic groups appears to result from cultural or other
environmental factors.
[18]
Social-emotional development[edit]
What develops?[edit]
Newborn infants do not seem to experience fear or have preferences for contact
with any specific people. In the first few months they only experience happiness,
sadness, and anger
[citation needed]
. A babys first smile usually occurs between 6 and
10 weeks. It is called a social smile because it usually occurs during social
interactions.
[citation needed]
By about 812 months, they go through a fairly rapid
change and become fearful ofperceived threats; they also begin to prefer familiar
people and show anxiety and distress when separated from them or approached by
strangers.
[citation needed]
Separation anxiety is a typical stage of development to an extent. Kicking,
screaming, and throwing temper tantrums are perfectly typical symptoms
for separation anxiety. Depending on the level of intensity, one may determine
whether or not a child has separation anxiety disorder. This is when a child
constantly refuses to separate from the parent, but in an intense manner. This can
be given special treatment but the parent usually cannot do anything about the
situation.
[36]
The capacity for empathy and the understanding of social rules begin in the
preschool period and continue to develop into adulthood.
[citation needed]
Middle
childhood is characterized by friendships with age-mates, and adolescence by
emotions connected with sexuality and the beginnings of romantic love.
[citation
needed]
Anger seems most intense during the toddler and early preschool period and
during adolescence.
[18]
Speed and pattern of development[edit]
Some aspects of social-emotional development,
[citation needed]
like empathy,
[citation
needed]
develop gradually, but others, like fearfulness,
[citation needed]
seem to involve a
rather sudden reorganization of the child's experience of emotion.
[citation
needed]
Sexual and romantic emotions develop in connection with physical
maturation.
[18]
The ability to learn temporal patterns in sequenced actions was investigated in
elementary-school age children. Temporal learning depends upon a process of
integrating timing patterns with action sequences. Children ages 613 and young
adults performed a serial response time task in which a response and a timing
sequence were presented repeatedly in a phase-matched manner, allowing
for integrative learning. The degree of integrative learning was measured as the
slowing in performance that resulted when phase-shifting the sequences. Learning
was similar for the children and adults on average but increased with age for the
children. Executive function measured by Wisconsin Card Sorting Test
(WCST) performance as well as a measure of response speed also improved with
age. Finally, WCST performance and response speed predicted temporal learning.
Taken together, the results indicate that temporal learning continues to develop in
pre-adolescents and that maturing executive function or processing speed may play
an important role in acquiring temporal patterns in sequenced actions and the
development of this ability.
[37]
Mechanisms of social and emotional development[edit]
Genetic factors appear to regulate some social-emotional developments that occur
at predictable ages, such as fearfulness, and attachment to familiar people.
Experience plays a role in determining which people are familiar, which social
rules are obeyed, and how anger is expressed.
[18]
Parenting practices have been shown to predict children's emotional intelligence.
The objective is to study the time mothers and children spent together in joint
activity, the types of activities that they develop when they are together, and the
relation that those activities have with the children's trait emotional intelligence.
Data was collected for both mothers and children (N = 159) using self-report
questionnaires. Correlations between time variables and trait emotional intelligence
dimensions were computed using Pearson's Product-Moment Correlation
Coefficient. Partial correlations between the same variables controlling for
responsive parenting were also computed. The amount of time mothers spent with
their children and the quality of their interactions are important in terms of
children's trait emotional intelligence, not only because those times of joint activity
reflect a more positive parenting, but because they are likely to promote modeling,
reinforcement, shared attention, and social cooperation.
[38]
Individual differences[edit]
Typical individual differences in motor ability are common and depend in part on
the child's weight and build. However, after the infant period, typical individual
differences are strongly affected by opportunities to practice, observe, and be
instructed on specific movements. Atypical motor development may be an
indication of developmental delays or problems such as autism or cerebral palsy.
[18]
Population differences[edit]
Population differences may occur in older children, if, for example they have
learned that it is appropriate for boys to express emotion or behave differently than
girls,
[citation needed]
or if customs learned by children of one ethnic group are different
from those learned in another.
[citation needed]
Social and emotional differences between
boys and girls of a given age may also be associated with differences in the timing
of puberty characteristic of the two sexes.
[18]
Language[edit]
Main article: Language development
What develops?[edit]
In addition to acquiring speech and a large spoken vocabulary, there are four main
areas in which the child must attain competence, regardless of
the language or dialect spoken. These are referred to as phonology or
sounds, semantics or the encoded meanings, syntax or the way in which words are
combined and pragmatics or knowledge of how language is used in different
contexts.
[39]
Speed and pattern of development[edit]
Receptive language, the understanding of others' speech, has a gradual
development beginning at about 6 months. However, expressive language, the
production of words, moves rapidly after its beginning at about a year of age, with
a "vocabulary explosion" of rapid word acquisition occurring in the middle of the
second year. This vocabulary expansion is closely linked to the ability to repeat
spoken words and enables the rapid acquisition of skill in their pronunciation.
Grammatical rules and word combinations appear at about age two. Mastery of
vocabulary and grammar continue gradually through the preschool and school
years. Adolescents still have smaller vocabularies than adults and experience more
difficulty with constructions like the passive voice.
Babies from one month old can produce "ooh" sounds which appear to grow out of
pleasurable interactions with caregivers in a mutual "dialogue". According to
Stern, this process is communication of affect between adult and infant in a mutual,
rhythmic interaction. The atonement and "gaze-coupling" in which infant and adult
take different roles is thought to anticipate the give-and-take of later dialogue.
From about 6 to 9 months babies produce more vowels,
some consonants and echolalia, or the frequent repetition of sounds like
"dadadada" which appear to have some phonetic characteristics of later speech. It
is thought that a crucial part of the development of speech is the time caregivers
spend "guessing" what their infants are trying to communicate thus integrating the
child into their social world. When infants are trying to learn words from others
they tend to create protowords, which is a "unique string of phonemes that serve
word-like functions. The attribution of intentionality to the infant's utterances has
been called "shared memory" and forms a complex series of actions, intentions and
actions in response in an improvised way.
It has been argued that children's phonological systems develop in ways that are
parallel to adult languages, even if they are using unrecognizable "words".
[40]
First
words have the function of naming or labeling but also condense meaning as in
"milk" meaning "I want milk".
[40]
Vocabulary typically grows from about 20 words
at 18 months to around 200 words at 21 months.
[40]
From around 18 months the
child starts to combine words into two word sentences.[citation needed] Typically
the adult expands it to clarify meaning. By 2427 months the child is producing
three or four word sentences using a logical, if not strictly correct, syntax.
[40]
The
theory is that children apply a basic set of rules such as adding 's' for plurals or
inventing simpler words out of words too complicated to repeat like "choskit" for
chocolate biscuit.
[40]
Following this there is a rapid appearance of grammatical
rules and ordering of sentences.
[40]
There is often an interest in rhyme, and
imaginative play frequently includes conversations.
[40]
Children's recorded
monologues give insight into the development of the process of organizing
information into meaningful units.
[40]
By three years the child is beginning to use complex sentences, including relative
clauses, although still perfecting various linguistic systems.
[40]
By five years of age
the child's use of language is very similar to that of an adult. From the age of about
three children can indicate fantasy or make-believe linguistically, produce coherent
personal stories and fictional narrative with beginnings and endings. It is argued
that children devise narrative as a way of understanding their own experience and
as a medium for communicating their meaning to others.
[40]
The ability to engage
in extended discourse emerges over time from regular conversation with adults and
peers.
[40]
For this the child needs to learn to combine his perspective with that of
others and with outside events and learn to use linguistic indicators to show he is
doing this. They also learn to adjust their language depending on to whom they are
speaking.
[40]
Typically by the age of about 9 a child can recount other narratives in
addition to their own experiences, from the perspectives of the author, the
characters in the story and their own views.
[40]
Mechanisms of language development[edit]
Although the role of adult discourse is important in facilitating the child's learning,
there is considerable disagreement amongst theorists about the extent to which
children's early meanings and expressive words arises directly from adult input as
opposed to intrinsic factors relating to the child's cognitive functions. Findings
about the initial mapping of new words, the ability to decontextualise words and
refine meaning are diverse.
[5]
One hypothesis is known as the
syntactic bootstrapping hypothesis, referring to the child's ability to infer meaning
from cues, using grammatical information from the structure of
sentences.
[41]
Another is the multi-route model in which it is argued that context-
bound words and referential words follow different routes; the first being mapped
onto event representations and the latter onto mental representations. In this model,
although parental input has a critical role, children rely on cognitive processing to
establish subsequent use of words.
[42]
However, naturalistic research on language
development has indicated that preschoolers' vocabularies are strongly associated
with the number of words addressed to them by adults.
[43]
There is as yet no single accepted theory of language acquisition. Current
explanations vary in emphasis from learning theory, with its emphasis on
reinforcement and imitation (Skinner), to biological, nativist theories, with innate
underlying mechanisms (Chomsky and Pinker), to a more interactive approach
within a social context (Piaget and Tomasello).
[5]
Behaviorists argue that given the
universal presence of a physical environment and, usually, a social environment,
any theory of language must account for the effects of the contingent relations of
these on an individuals development of language behaviour.
[44][45][46]
Pinker argues
that complex language is universal and has an innate basis. Pinker's argument is
partly based on the development of creole languages from pidgins. The children of
parents who communicate, without grammatical structures, in pidgin, develop a
creole language of their own accord, complete with standardised word orders,
markers for present, future and past tenses and subordinate clauses.
[47]
There is
some support for this from the development of sign language amongst deaf
children thrown together at a young age in special schools in Nicaragua who
spontaneously developed a pidgin which was then developed into a creole by a
younger generation of children coming into the schools, (ISN).
[48][49]
Individual differences[edit]
Delays in language is the most frequent type of developmental delay. According to
demographics 1 out of 5 children will learn to talk or use words later than other
children their age. Speech/language delay is three to four times more common in
boys than in girls. Some children will also display behavioral problems due to their
frustration of not being able to express what they want or need.
Simple speech delays are usually temporary. Most cases are solved on their own or
with a little extra attribution from the family. Its the parents duty to encourage
their baby to talk to them with gestures or sounds and for them to spend a great
amount of time playing with, reading to, and communicating with their baby. In
certain circumstances, parents will have to seek professional help, such as a speech
therapist.
It is important to take into considerations that sometimes delays can be a warning
sign of more serious conditions that could include auditory processing
disorders, hearing loss, developmental verbal dyspraxia, developmental delay in
other areas, or even an autism spectrum disorder (ASD).
Environmental causes[edit]
There are many environmental causes that are linked to language delays and they
include situations such as, the child is having their full attention on other skills,
such as walking perfectly, rather than on language. The child may have a twin or a
sibling in which their age are relatively close, and may not be receiving the
parents full attention. Another circumstance could be a child that is in a daycare
that provides few adults to be able to administer individual attention. Perhaps the
most obvious component would be a child that suffers from psychosocial
deprivation such as poverty, malnutrition, poor housing, neglect, inadequate
linguistic stimulation, or emotional stress.
Neurological causes[edit]
Language delay can be caused by a substantial amount of underlying disorders,
such as intellectual disability. Intellectual disability takes part for more than 50
percent of language delays. Language delay is usually more rigorous than other
developmental delays in intellectually disabled children, and it is usually the first
obvious symptom of intellectual disability. Intellectual disability accounts to global
language delay, including delayed auditory comprehension and use of gestures.
Impaired hearing is one of the most common causes of language delay. A child
who can not hear or process speech in a clear and consistent manner will have
a language delay. Even the most minimum hearing impairment orauditory
processing deficit can considerably affect language development. Essentially, the
more the severe the impairment, the more serious the language delay.
Nevertheless, deaf children that are born to families who usesign language develop
infant babble and use a fully expressive sign language at the same pace as hearing
children.
Developmental Dyslexia is a developmental reading disorder that occurs when the
brain does not properly recognize and process the graphic symbols chosen by
society to represent the sounds of speech. Children with dyslexia may encounter
problems in rhyming and separating sounds that compose words. These abilities
are essential in learning to read. Early reading skills rely heavily on word
recognition. When using an alphabet writing system this involves in having the
ability to separate out the sounds in words and be able to match them with letter
and groups of letters. Because they have trouble in connecting sounds of language
to the letter of words, this may result difficulty in understanding sentences. They
have confusion in mistaking letters such as "b" and "d". For the most part,
symptoms of dyslexia may include, difficulty in determining the meaning of a
simple sentence, learning to recognize written words, and difficulty in rhyming.
Autism and speech delay are usually correlated. Problems with verbal language are
the most common signs seen in autism. Early diagnosis and treatment of autism
can significantly help the child improve their speech skills. Autism is recognized as
one of the five pervasive developmental disorders, distinguished by problems with
language, speech, communication and social skills that present in early childhood.
Some common autistic syndromes are the following, being limited to no verbal
speech, echolalia or repeating words out of context, problems responding to verbal
instruction and may ignore others who speak directly.
Risk factors for poor child development[edit]
Child development can be negatively influenced by a number of risk factors, many
of which have been studied in developing countries.
[50]
They can be broadly
grouped under two headings.
Hereditary
Environmental factors
1. Pre-natal environment
Factors related to mothers during pregnancy
Nutritional deficiencies
Diabetic mother
Exposure to radiation
Infection with German measles
Smoking
Use of drugs
Factors related to fetus
Mal-position in uterus
Faulty placental implantation
2. Post-Natal Environment
External environment
Socio-economic status of the family
Childs nutrition
Climate and season
Childs ordinal position in the family
Number of siblings in the family
Family structure (single parent or extended family etc.)
Internal environment
Childs intelligence
Hormonal influences
Emotions
Malnutrition, maternal depression and maternal substance abuse are three of these
factors which have received particular attention by researchers, however, many
more factors have been considered.
[51][52][53]
Postnatal depression[edit]
Main article: Postpartum depression
Although there are a large number of studies contemplating the effect of maternal
depression and postnatal depression of various areas of infant development, they
are yet to come to consensus regarding the true effects. There are numerous studies
indicating a negative impact on development, and equally there are many
proclaiming no effect of depression on development. A study of 18 month olds
whose mothers suffered depressive symptoms while they were 6 weeks and/or 6
months old indicated that maternal depression had no effect on the childs
cognitive development at 18 months.
[54]
Furthermore, the study indicates that
maternal depression combined with a poor home environment is more likely to
have an effect on cognitive development. However, the authors conclude that it
may be that short term depression has no effect, where as long term depression
could cause more serious problems. A further longitudinal study spanning 7 years
again indicate no effect of maternal depression on cognitive development as a
whole, however it found a gender difference in that boys are more susceptible to
cognitive developmental issues when their mothers suffer depression.
[52]
This
thread is continued in a study of children up to 2 years old.
[55]
The study reveals a
significant difference on cognitive development between genders, with girls having
a higher score, however this pattern is found regardless of the childs mothers
history of depression. Infants with chronically depressed mothers showed
significantly lower scores on the motor and mental scales within the Bayley Scales
of Infant Development,
[55]
contrasting with many older studies.
[52][54]
A similar
effect has been found at 11 years: male children of depressed mothers score an
average of 19.4 points lower on an Intelligence Quotient IQ test than those with
healthy mothers, although this difference is much lower in girls.
[56]
3 month olds
with depressed mothers show significantly lower scores on the Griffiths Mental
Development Scale, which covers a range of developmental areas including
cognitive, motor and social development.
[57]
It has been suggested that interactions
between depressed mothers and their children may have an impact on social and
cognitive abilities in later life.
[58]
Maternal depression has been shown to influence
the mothers interaction with her child.
[59]
When communicating with their child,
depressed mothers fail to make changes to their vocal behaviour, and tend use
unstructured vocal behaviours.
[60]
Furthermore, when infants interact with
depressed mothers they show signs of stress, such as increased pulse and raised
cortisol levels, and make more use of avoidance behaviours, for example looking
away, compared to those interacting with healthy mothers.
[58]
The impact of
mother-infant interaction at 2 months has been shown to affect the childs
cognitive performance at 5 years.
[61]
Maternal cocaine abuse[edit]
Main article: Prenatal cocaine exposure
Research has provided conflicting evidence regarding the impact of maternal
substance abuse during and after pregnancy on childrens
development.
[53]
Children exposed to cocaine weigh less than those not exposed at
numerous ages ranging from 6 to 30 months.
[62]
Furthermore studies indicate that
the head circumference of children exposed to cocaine is lower than those
unexposed.
[62][63]
On the other hand, two more recent studies found no significant
differences between those exposed to cocaine and those who were not in either
measure.
[64][65]
Maternal cocaine use may also affect the childs cognitive
development, with exposed children achieving lower scores on measures of
psychomotor and mental development.
[66][67]
However, again there is conflicting
evidence, and a number of studies indicate no effect of maternal cocaine use on
their childs cognitive development.
[68][69]
Motor development can be negatively
impacted by maternal cocaine abuse.
[70][71]
As is the case for cognitive and physical
development, there are also studies showing no effect of cocaine use on motor
development.
[62][65]
Malnutrition[edit]
Malnutrition is a large problem in developing nations, and has an important impact
on young childrens weight and height. Children suffering malnutrition in
Columbia weighed less than those living in upper class conditions at the age of 36
months (11.88 kg compared to 14 kg), similarly, malnourished children were
shorter than well-nourished children, again at 36 months (85.3 cm in malnourished
children; 94 cm in well-nourished children
[51]
Malnutrition has been indicated as a
negative influence on childhood Intelligence Quotient IQ.
[72][73]
Although it is now
suggested that this effect is nullified when parental IQ is considered, implying that
this difference is genetic.
[74]
Nutrients[edit]
The impact of low iron levels on cognitive development and IQ is a subject still to
reach consensus.
[75]
Some evidence suggests that well-nourished children with
lower levels of iron and folate (although not at such a level to be considered
deficient) have a lower IQ than those with higher levels of iron and
folate.
[76]
Furthermore, anaemic children perform worse on cognitive measures
than non-anaemic children.
[77]
These nutrients have been strongly implicated in
brain development, along with iodine and zinc.
[78]
Iodine is required for the
generation of thyroid hormones necessary for brain development.
[79]
Iodine
deficiency may reduce IQ by an average of 13.5 points compared to healthy
individual.
[80]
Zinc deficiency has also been shown to have a negative impact on
childhood growth and development.
[81][82]
Socioeconomic status[edit]
Socioeconomic status is measured primarily based on the factors of income,
educational attainment and occupation.
[83]
Current investigations into the role of
socioeconomic factors on child development repeatedly show that continual
poverty is more harmful on Intelligence Quotient IQ,
[84]
and cognitive
abilities
[85]
than short-lived poverty. Children in families who experience persistent
financial hardships and poverty have significantly impaired cognitive abilities
compared to those in families who do not face this issue.
[85]
Low income poverty
can cause a number of further issues shown to effect child development, such as
malnutrition and lead poisoning due to lead paint found on the walls of some
houses.
[86]
Child blood levels of lead increase as income decreases.
[87]
Income
poverty is associated with a 613 point reduction in IQ for those earning half of the
poverty threshold compared to those earning twice the poverty threshold.
[84]
That
being said, children coming from households featuring continual or temporary
poverty still perform lower than children in middle-class families.
[85]
Parental educational attainment is the most significant socioeconomic factor in
predicting the childs cognitive abilities,
[88]
those with a mother with high IQ are
likely to have higher IQs themselves.
[74][89]
Similarly, maternal occupation is
associated with better cognitive achievement. Those whose mothers job entails
problem-solving are more likely to be given stimulating tasks and games, and are
likely to achieve more advanced verbal competency.
[90]
Poverty-stricken children are subjected to fewer stimulating recreational activities,
often missing out on trips to libraries or museums, and are unable to access a tutor
to help with problematic academic areas.
[91]
A further factor in a childs educational attainment involves the school
environment, more specifically teacher expectations and attitudes.
[92]
It has been
argued that teachers perceive low-SES children as being less academically able and
as such provide them with less attention and reinforcement.
[92]
Parasites[edit]
Diarrhea caused by the parasitic disease Giardiasis is associated with lower
IQ.
[93]
Parasitic worms (helminths) are associated with nutritional deficiencies that
are known to be a risk to child development.
[94]
In particular, intestinal parasitism
being one of the most neglected tropical diseases in the developed world.
Harboring of this parasite could adverse several health implications in children
affecting childhood development and morbidity. Reducing the prevalence of the
parasite can be a benefit in child growth, development and educational outcome.
[95]
Poisoning[edit]
High levels of lead in the blood is associated with attention
deficits,
[96]
while arsenic poisoning has a negative effect on verbal and
full Intelligence Quotient IQ.
[96]
Manganese poisoning due to levels in drinking
water is also associated with a reduced IQ of 6.2 points between the highest and
lowest level of poisoning.
[97]
Prenatal exposure to various pesticides including
organophosphates,
[98]
and chlorpyrifos
[99]
has also been linked to reduced IQ
score. Organophosphates have been specifically linked to poorer working memory,
verbal comprehension, perceptual reasoning and processing speed.
[98]
Other factors[edit]
Cognitive development is related to childhood exposure to violence and trauma,
including spousal abuse between the parents and sexual abuse.
[100]
Intrauterine
growth retardation is associated with learning deficits in childhood, and as such, is
related to lower IQ.
[101]
See also[edit]
Attachment theory
Autism
Behavioral cusp
Birth order
Child development stages, for
development specifications by each
month and year
Child life specialist
Child prodigy
Clinical social work
Critical period
Developmental psychology
Developmental psychobiology
Early childhood education
Emergent literacies
Evolutionary developmental
psychology
Healthy narcissism
Jointness (psychodynamics)
Neurodevelopmental
disorder
Overpopulation
Pedagogy
Peter Pan syndrome
Play (activity)
Thematic coherence
Early Childhood Longitudinal
Developmental psychopathology Program
References[edit]
1. Jump up^ Toga, AW.; Thompson, PM.; Sowell, ER. (2006). "Mapping brain
maturation". Trends Neuroscience 29(3): 148
59. doi:10.1016/j.tins.2006.01.007. PMC 3113697. PMID 16472876.
2. Jump up^ Kail, Robert V (2011). Children and Their Development (6th
Edition) (Mydevelopmentlab Series). Englewood Cliffs, N.J: Prentice
Hall. ISBN 0-205-03494-2. OCLC 727047867.
3. Jump up^ Vilaa, S. (2012). Desenvolvimento infantil e capacitao materna
como resultado da aplicao do Programa de Empowerment Parental para
o desenvolvimento infantil (PEPDI). (doctoral), University of Minho.
Retrieved from http://hdl.handle.net/1822/24370
4. Jump up^ Bronfenbrenner, Urie (1979). The ecology of human
development: experiments by nature and design. Cambridge: Harvard
University Press. ISBN 0-674-22456-6. OCLC 4515541.
5. ^ Jump up to:
a
b
c
Blades, Mark; Smith, Peter K.; Cowie, Helen
(2011). Understanding Children's Development. Wiley-Blackwell. ISBN 1-
4051-7601-6. OCLC 620124946.
6. ^ Jump up to:
a
b
c
d
e
f
g
h
i
j
k
l
m
Shaffer, David R. (2009). Social and
personality development (6th ed.). Australia: Wadsworth. ISBN 978-0-495-
60038-1.
7. ^ Jump up to:
a
b
c
Cole, Michael; Vygotski, L. S. (1978 (Published originally
in Russian in 1930)). Mind in society: the development of higher
psychological processes. Cambridge: Harvard University Press. ISBN 0-674-
57628-4.OCLC 3517053.
8. Jump up^ Kozulin, Alex; Lev Semenovich Vygotsky (2012). Thought and
Language. Cambridge, Mass: The MIT Press. ISBN 0-262-51771-
X. OCLC 768728899.
9. Jump up^ Wertsch, James V. (1985). Culture, communication, and
cognition: Vygotskian perspectives. Cambridge, UK: Cambridge University
Press. ISBN 0-521-33830-1. OCLC 715955821.
10. Jump up^ Carton, Aaron S.; Vygotski, L. S.; Rieber, R. W. (1987). The
collected works of L. S. Vygotsky. 5, Child psychology. New York: Plenum
Press. ISBN 0-306-45707-5. OCLC 312913751.
11. Jump up^ Denise Boyd; Wood, Samuel H.; Wood, Ellen Meiksins
(2010). Mastering the World of Psychology, Books a la Carte Edition (4th
Edition). Englewood Cliffs, N.J: Prentice Hall. ISBN 0-205-00505-
5.OCLC 660087952.
12. Jump up^ Manning, M.Lee (September 1988). "Erikson's Psychosocial
Theories Help Explain Early Adolescence".NASSP Bulletin 72 (509): 95
100. doi:10.1177/019263658807250914.
13. Jump up^ "WHAT THE NURSERY: HAS TO SAY ABOUT INSTINCTS by JOHN B.
WATSON". Psychologies of 1925: Powell Lectures in Psychological Theory by
Madison Bentley, Knight Dunlap, Walter S. Hunter, Kurt Koffka, Wolfgang
Khler, William McDougall, Morton Prince, John B. Watson, Robert S.
Woodworth, Carl Murchison.
14. Jump up^ Lemma, Alessandra (2002). "Psychodynamic Therapy: The
Freudian Approach". In W. Dryden. Handbook of individual therapy.
Thousand Oaks, Calif: Sage. ISBN 0-7619-6943-8. OCLC 50279223.
15. Jump up^ Aslin, Richard N. (1993). "Commentary : the strange
attractiveness of dynamic systems to development". In Thelen, Esther;
Smith, Linda C. A Dynamic systems approach to development applications.
Cambridge, Mass: MIT Press. ISBN 0-585-03867-8. OCLC 42854628.
16. Jump up^ Sameroff, A. (1983). Factors in predicting successful parenting.. In
Hoekelman, Robert A.; Sasserath, Valerie. "Minimizing high-risk parenting:
a review of what is known and consideration of appropriate preventive
intervention". Johnson & Johnson Baby Products Company pediatric round
table series (Radnor, Pa: Skillman, N.J. :The Company). ISBN 0-931562-07-
4. OCLC 8689673.
17. Jump up^ Berk, Laura E. (2009). Child development. Boston: Pearson
Education/Allyn & Bacon. ISBN 0-205-61559-7. OCLC 232605723.
18. ^ Jump up to:
a
b
c
d
e
f
g
h
i
j
k
l
m
n
o
Patterson, Charlotte (2008). Child
development. Boston: McGraw-Hill Higher Education. ISBN 0-07-234795-
3. OCLC 179102376.
19. Jump up^ Gross, J. (1987). Introducing Erik Erikson. Landham, MD:
University Press of America, ISBN 0819157880.
20. Jump up^ Erikson, Erik H. (1968). Identity: youth, and crisis. New York:
W.W. Norton. ISBN 0-393-31144-9.OCLC 750885788.
21. ^ Jump up to:
a
b
c
Mercer J (1998). Infant Development: A Multidisciplinary
Introduction. Pacific Grove, CA: Brooks/Cole. ISBN 0534339778.
22. ^ Jump up to:
a
b
c
d
e
f
g
h
i
j
k
l
m
n
o
p
Feldman, R. S. (2011). Development
across the life span. 6th ed., Upper Saddle River, NJ: Prentice Hall, ISBN
0205805914.
23. Jump up^ Plomin, Robert and Asbury, Kathryn (2005). "Nature and Nurture:
Genetic and Environmental Influences on Behavior". Annals of the
American Academy of Political and Social Science 600: 86
98.doi:10.1177/0002716205277184. JSTOR 25046112.
24. Jump up^ Tau GZ, Peterson BS (January 2010). "Normal development of
brain circuits". Neuropsychopharmacology35 (1): 147
68. doi:10.1038/npp.2009.115. PMC 3055433. PMID 19794405.
25. Jump up^ Buchwald J (1987). "A comparison of plasticity in sensory and
cognitive processing systems". In Gunzenhauser N. Infant Stimulation.
Skillman NJ: Johnson & Johnson. ISBN 0931562155.
26. Jump up^ Greenough WT, Black JE, Wallace CS (June 1987). "Experience
and brain development". Child Dev 58(3): 539
59. doi:10.2307/1130197. PMID 3038480.
27. Jump up^ Greenough W, Black J and Wallace C (1993). "Experience and
brain development". In Johnson M. Brain Development and Cognition.
Oxford: Blackwell. pp. 319322. ISBN 0-631-18222-5. OCLC 25874371.
28. Jump up^ Berk L (2005). Infants, Children, and Adolescents. Boston: Allyn &
Bacons. ISBN 0205511384.
29. ^ Jump up to:
a
b
c
d
Tanner JM (1990). Fetus into Man. Cambridge MA:
Harvard University Press. ISBN 0674306929.
30. Jump up^ "FDA Approves Humatrope for Short Stature". U.S. Food and
Drug Administration. 2003-07-25. Retrieved 2009-01-13.
31. Jump up^ "Failure to Thrive: Miscellaneous Disorders in Infants and
Children: Merck Manual Professional". Retrieved 2010-03-23.
32. Jump up^ Willingham, D. B. (1999). "The Neural Basis of Motor-Skill
Learning". Current Directions in Psychological Science 8 (6): 178
182. doi:10.1111/1467-8721.00042.
33. Jump up^ Bell, S. (2011-06-14). Flexibility diets. livestrong.com
34. Jump up^ Soska, K. C.; Adolph, K. E.; Johnson, S. P. (2010). "Systems in
development: Motor skill acquisition facilitates three-dimensional object
completion". Developmental Psychology 46 (1): 129
138.doi:10.1037/a0014618. PMC 2805173. PMID 20053012.
35. Jump up^ Brotherson, S. (April 2005) "Understanding Brain Development in
Young Children",
36. Jump up^ Lawrence Robinson (2012). Separation Anxiety in Children.
helpguide.org
37. Jump up^ Shin, J. C. (2011). "The development of temporal coordination in
children". Brain and Cognition 76 (1): 106
114. doi:10.1016/j.bandc.2011.02.011. PMID 21463915.
38. Jump up^ Alegre, A. (2012). "The Relation Between the Time Mothers and
Children Spent Together and the Children's Trait Emotional
Intelligence". Child & Youth Care Forum 41 (5): 493
508. doi:10.1007/s10566-012-9180-z. edit
39. Jump up^ "The Four Language Systems". The Learning House, Inc.
Retrieved 5 March 2013.
40. ^ Jump up to:
a
b
c
d
e
f
g
h
i
j
k
l
m
Child Health Nursing. India: Gennext
Publication. 2010. p. 90. ISBN 978-81-908675-0-4.
41. Jump up^ Gleitman LR (1990). "The structural sources of verb
meaning". Language Acquisition 1 (1): 3
55.doi:10.1207/s15327817la0101_2.
42. Jump up^ Barrett MD, Harris M and Chasan J (1991). "Early lexical
development and maternal speech: a comparison of children's initial and
subsequent uses of words". Journal of Child Language 18 (1): 21
40.doi:10.1017/S0305000900013271. PMID 2010501.
43. Jump up^ Hart B and Risley T (1995). Meaningful differences in the
everyday experience of young American children. Baltimore: P.H. Brookes.
44. Jump up^ Moerk E (1996). "Input and learning processes in first language
acquisition". Advances in Child Development and Behavior. Advances in
Child Development and Behavior 26: 181229. doi:10.1016/S0065-
2407(08)60509-1. ISBN 9780120097265.
45. Jump up^ Moerk EL (1986). "Environmental factors in early language
acquisition". In Whitehurst GJ. Annals of child development 3. Greenwich:
CTJAI press.
46. Jump up^ Moerk EL (1989). "The LAD was a lady and the tasks were ill
defined". Developmental Review 9 (1): 2157. doi:10.1016/0273-
2297(89)90022-1.
47. Jump up^ Pinker S (1994). The Language Instinct. London: Allen
Lane. ISBN 0688121411.
48. Jump up^ Kegl J, Senghas A and Coppola M (1999). "Creation through
construct: Sign language emergence and sign language change in
Nicaragua". In DeGrafs M. Language Creation and Language Change:
Creolization, Diachrony and Development. Cambridge, MA: MIT
Press. ISBN 0262541262.
49. Jump up^ Morford JP and Kegl J (2000). "Gestural precursors to linguistic
constructs: how input shapes the form of language". In McNeill
D. Language and Gesture. Cambridge: Cambridge University
Press.ISBN 0521777615.
50. Jump up^ Walker, S. P.; Wachs, T. D.; Meeks Gardner, J.; Lozoff, B.;
Wasserman, G. A.; Pollitt, E.; Carter, J. A.; International Child Development
Steering Group (2007). "Child development: Risk factors for adverse
outcomes in developing countries". The Lancet 369 (9556): 145
157. doi:10.1016/S0140-6736(07)60076-2.PMID 17223478.
51. ^ Jump up to:
a
b
Mora, J. O.; Herrera, M. G.; Suescun, J.; De Navarro, L.;
Wagner, M. (1981). "The effects of nutritional supplementation on physical
growth of children at risk of malnutrition". The American journal of clinical
nutrition 34 (9): 18851892. PMID 7282613. edit
52. ^ Jump up to:
a
b
c
Kurstjens S., Wolke D. (2001). "Effects of maternal
depression on cognitive development of children over the first 7 years of
life". Journal of Child Psychology and Psychiatry 42 (5): 623
636.doi:10.1111/1469-7610.00758. PMID 11464967.
53. ^ Jump up to:
a
b
Frank, D. A.; Augustyn, M.; Knight, W. G.; Pell, T.;
Zuckerman, B. (2001). "Growth, Development, and Behavior in Early
Childhood Following Prenatal Cocaine Exposure: A Systematic
Review". JAMA: the Journal of the American Medical Association 285 (12):
1613
1625. doi:10.1001/jama.285.12.1613.PMC 2504866. PMID 11268270. edit
54. ^ Jump up to:
a
b
Piteo, A. M.; Yelland, L. N.; Makrides, M. (2012). "Does
maternal depression predict developmental outcome in 18month old
infants?". Early Human Development 88 (8): 651
655.doi:10.1016/j.earlhumdev.2012.01.013. PMID 22361258.
55. ^ Jump up to:
a
b
Cornish, A. M.; McMahon, C. A.; Ungerer, J. A.; Barnett, B.;
Kowalenko, N.; Tennant, C. (2005). "Postnatal depression and infant
cognitive and motor development in the second postnatal year: The impact
of depression chronicity and infant gender". Infant Behavior and
Development 28 (4): 407.doi:10.1016/j.infbeh.2005.03.004.
56. Jump up^ Hay D.F., Pawlby S., Sharp D., Asten P., Mills A., Kumar R. (2001).
"Intellectual problems shown by 11-year-old children whose mothers had
postnatal depression". Journal of Child Psychology and Psychiatry 42(7):
871889. doi:10.1111/1469-7610.00784. PMID 11693583.
57. Jump up^ Galler J.R., Harrison R.H., Ramsey F., Forde V., Butler S.C. (2000).
"Maternal depressive symptoms affect infant cognitive development in
Barbados". Journal of Child Psychology and Psychiatry 41 (6): 747
757. doi:10.1111/1469-7610.00662. PMID 11039687.
58. ^ Jump up to:
a
b
Field T., Healy B., Goldstein S., Guthertz M. (1990).
"Behaviour-state matching and synchrony in mother-infant interactions of
nondepressed versus depressed dyads". Developmental Psychology 26 (1):
714. doi:10.1037/0012-1649.26.1.7.
59. Jump up^ Reck, C.; Hunt, A.; Fuchs, T.; Weiss, R.; Noon, A.; Moehler, E.;
Downing, G.; Tronick, E. Z.; Mundt, C. (2004). "Interactive Regulation of
Affect in Postpartum Depressed Mothers and Their Infants: An
Overview". Psychopathology 37 (6): 272
280. doi:10.1159/000081983. PMID 15539778.
60. Jump up^ Bettes B.A. (1988). "Maternal depression and motherese:
Temporal and intonational features". Child Development 59 (4): 1089
1096. doi:10.2307/1130275. PMID 3168616.
61. Jump up^ Murray L., Kempton C., Woolgar M., Hooper R. (1993).
"Depressed mothers' speech to their infants and its relation to infant
gender and cognitive development". Journal of Child Psychology and
Psychiatry 34 (7): 10811101. doi:10.1111/j.1469-7610.1993.tb01775.x.
62. ^ Jump up to:
a
b
c
Hurt, H.; Brodsky, N. L.; Betancourt, L.; Braitman, L. E.;
Malmud, E.; Giannetta, J. (1995). "Cocaine-exposed Children". Journal of
Developmental & Behavioral Pediatrics 16: 2935. doi:10.1097/00004703-
199502000-00005. edit
63. Jump up^ Azuma S., Chasnoff I. (1993). "Outcome of children prenatally
exposed to cocaine and other drugs: A path analysis of three-year
data". Pediatrics 92 (3): 396402. PMID 7689727.
64. Jump up^ Richardson, G. A.; Conroy, M. L.; Day, N. L. (1996). "Prenatal
cocaine exposure: Effects on the development of school-age
children". Neurotoxicology and teratology 18 (6): 627
634. doi:10.1016/S0892-0362(96)00121-3. PMID 8947939. edit
65. ^ Jump up to:
a
b
Kilbride, H.; Castor, C.; Hoffman, E.; Fuger, K. L. (2000).
"Thirty-six-month outcome of prenatal cocaine exposure for term or near-
term infants: Impact of early case management". Journal of developmental
and behavioral pediatrics : JDBP 21 (1): 1926. doi:10.1097/00004703-
200002000-00004.PMID 10706345. edit
66. Jump up^ Singer, L. T.; Yamashita, T. S.; Hawkins, S.; Cairns, D.; Baley, J.;
Kliegman, R. (1994). "Increased incidence of intraventricular hemorrhage
and developmental delay in cocaine-exposed, very low birth weight
infants". The Journal of pediatrics 124 (5 Pt 1): 765
771. doi:10.1016/S0022-3476(05)81372-1.PMID 7513757. edit
67. Jump up^ Chasnoff I.J., Griffith D.R., Freier C., Murray J. (1992).
"Cocaine/polydrug use in pregnancy: Two-year follow-up". Pediatrics 89 (2):
284289. PMID 1370867.
68. Jump up^ Coles, C. D.; Bard, K. A.; Platzman, K. A.; Lynch, M. E. (1999).
"Attentional response at eight weeks in prenatally drug-exposed and
preterm infants". Neurotoxicology and teratology 21 (5): 527
537.doi:10.1016/S0892-0362(99)00023-9. PMID 10492387. edit
69. Jump up^ Graham, K.; Feigenbaum, A.; Pastuszak, A.; Nulman, I.; Weksberg,
R.; Einarson, T.; Goldberg, S.; Ashby, S.; Koren, G. (1992). "Pregnancy
outcome and infant development following gestational cocaine use by
social cocaine users in Toronto, Canada". Clinical and investigative
medicine. Medecine clinique et experimentale 15 (4): 384
394. PMID 1516296. edit
70. Jump up^ Fetters L., Tronick E.Z. (1996). "Neuromotor development of
cocaine-exposed and control infants from birth through 15 months: Poor
and poorer performance". Pediatrics 98 (5): 938943. PMID 8909489.
71. Jump up^ Swanson, M. W.; Streissguth, A. P.; Sampson, P. D.; Olson, H. C.
(1999). "Prenatal cocaine and neuromotor outcome at four months: Effect
of duration of exposure". Journal of developmental and behavioral
pediatrics : JDBP 20 (5): 325334. doi:10.1097/00004703-199910000-
00007.PMID 10533991. edit
72. Jump up^ Ivanovic D.M., Leiva B.P., Perez H.T., Olivares M.G., Diaz N.S.,
Urrutia M.S., Almagia A.F., Toro T.D., Miller P.T. et al. (2004). "Head size
and intelligence, learning, nutritional status and brain development: Head,
IQ, learning, nutrition and brain". Neuropsychologia 42 (8): 1118
1131.doi:10.1016/j.neuropsychologia.2003.11.022. PMID 15093150.
73. Jump up^ Liu, J. (2003). "Malnutrition at Age 3 Years and Lower Cognitive
Ability at Age 11 Years<subtitle>Independence from Psychosocial
Adversity</subtitle>". Archives of Pediatrics & Adolescent Medicine 157 (6):
593. doi:10.1001/archpedi.157.6.593. edit
74. ^ Jump up to:
a
b
Webb K.E., Horton N.J., Katz D.L. (2005). "Parental IQ and
cognitive development of malnourished Indonesian children". European
Journal of Clinical Nutrition 59 (4): 618
620. doi:10.1038/sj.ejcn.1602103.PMID 15688080.
75. Jump up^ Grantham-Mcgregor, S.; Ani, C. (2001). "A review of studies on
the effect of iron deficiency on cognitive development in children". The
Journal of nutrition 131 (2S2): 649S666S; discussion 666S
668S.PMID 11160596. edit
76. Jump up^ Arija V., Espar G., Fernndez-Ballart J., Murphy M.M., Biarns E.,
Canals J. (2006). "Nutritional status and performance in test of verbal and
non-verbal intelligence in 6 year old children". Intelligence 34 (2): 141
149. doi:10.1016/j.intell.2005.09.001.
77. Jump up^ Halterman J.S., Kaczorowski J.M., Aligne C.A., Auinger P., Szilagyi
P.G. (2001). "Iron deficiency and cognitive achievement among school-aged
children and adolescents in the United States". Pediatrics 107 (6): 1381
1386. doi:10.1542/peds.107.6.1381. PMID 11389261.
78. Jump up^ Bryan J., Osendarp S., Hughes D., Calvaresi E., Baghurst K.,
Klinken J.W. (2004). "Nutrients for Cognitive Development in Schoolaged
Children". Nutrition Reviews 62 (8): 295306. doi:10.1111/j.1753-
4887.2004.tb00055.x. PMID 15478684.
79. Jump up^ Reavley N. (1998). Vitamins, etc. Melbourne: Bookman Media Pty
Ltd
80. Jump up^ Bleichrodt, N. and Born, M.P. (1994). A meta-analysis of research
on iodine and its relationship to cognitive development. The damaged brain
of iodine deficiency. New York: Cognizant Communication, pp. 195200.
81. Jump up^ Brown K. H., Peerson J. M., Rivera J., Allen L.H. (2002). "Effect of
supplemental zinc on the growth and serum zinc concentrations of
prepubertal children: a meta-analysis of randomized controlled trials". The
American Journal of Clinical Nutrition 75 (6): 10621071. PMID 12036814.
82. Jump up^ Bhutta Z.A., Black R.E., Brown K.H., Gardner J.M., Gore S.,
Hidayat A. et al. (1999). "Prevention of diarrhea and pneumonia by zinc
supplementation in children in developing countries: pooled analysis of
randomized controlled trials". The Journal of Pediatrics 135 (6): 689
697. doi:10.1016/S0022-3476(99)70086-7. PMID 10586170.
83. Jump up^ Socioeconomic Status. American Psychological Association.
84. ^ Jump up to:
a
b
Smith, J.R., Brooks-Gunn, J., and Klebanov, P. (1997). "The
consequences of living in poverty for young childrens cognitive and verbal
ability and early school achievement". In Consequences of growing up poor.
G.J. Duncan and J. Brooks-Gunn (eds.) New York: Russell Sage
Foundation, ISBN 0871541432.
85. ^ Jump up to:
a
b
c
Schoon, I.; Jones, E.; Cheng, H.; Maughan, B. (2011).
"Family hardship, family instability, and cognitive development". Journal of
Epidemiology & Community Health 66 (8): 716
722.doi:10.1136/jech.2010.121228. PMID 21507894.
86. Jump up^ Brooks-Gunn, J.; Duncan, G. J. (1997). "The effects of poverty on
children". The Future of children / Center for the Future of Children, the
David and Lucile Packard Foundation 7 (2): 55
71.doi:10.2307/1602387. PMID 9299837.
87. Jump up^ Brody D.J., Pirkle J.L., Kramer R.A., Flegal K.M., Matte T.D.,
Gunter E.W., Paschal D.C. (1994). "Blood lead levels in the US
population". The Journal of the American Medical Association 272 (4): 277
283.doi:10.1001/jama.272.4.277.
88. Jump up^ DeGarmo D.S., Forgatch M.S., Martinez Jr C.R. (2003). "Parenting
of divorced mothers as a link between social status and boys' academic
outcomes: Unpacking the effects of socioeconomic status". Child
Development 70 (5): 12311245. doi:10.1111/1467-
8624.00089. PMID 10546342.
89. Jump up^ Honzik, M. P. (1957). "Developmental studies of parent-child
resemblance in intelligence". Child development 28 (2): 215
228. PMID 13427072. edit
90. Jump up^ Parcel, T.L. and Menaghan, E.G. (1990). "Maternal working
conditions and children's verbal facility: Studying the intergenerational
transmission of inequality from mothers to young children". Social
Psychology Quarterly 53 (2): 132
147. doi:10.2307/2786675. JSTOR 2786675.
91. Jump up^ Bradley, R.H., Corwyn, R.F., McAdoo, H.P. and Garca Coll, C.
(2003). "The home environments of children in the United States Part I:
Variations by age, ethnicity, and poverty status". Child Development72 (6):
18441867. doi:10.1111/1467-8624.t01-1-00382. PMID 11768149.
92. ^ Jump up to:
a
b
McLoyd, Vonnie C.; Taylor, Ronald D.; Wang, Margaret C.
(Eds.) (1997). The impact of poverty and low socioeconomic status on the
socioemotional functioning of African-American children and adolescents:
mediating effects. abstract, pp. 734. Mahwah, NJ, US: Lawrence Erlbaum
Associates Publishers
93. Jump up^ Ajjampur, S. S. R.; Koshy, B.; Venkataramani, M.; Sarkar, R.;
Joseph, A. A.; Jacob, K. S.; Ward, H.; Kang, G. (2011). "Effect of
cryptosporidial and giardial diarrhoea on social maturity, intelligence and
physical growth in children in a semi-urban slum in south India". Annals of
Tropical Paediatrics: International Child Health 31 (3): 205
212. doi:10.1179/1465328111Y.0000000003. PMID 21781414. edit
94. Jump up^ World Health Organisation. (1987). Prevention and control of
intestinal parasitic infections.
95. Jump up^ Opara, K (2012). "The Impact of Intestinal Parasitic Infections on
the Nutritional Status of Rural and Urban School-Aged Children in
Nigeria". International Journal of MCH and AIDS 1 (1): 7382.
96. ^ Jump up to:
a
b
Caldern, J.; Navarro, M. E.; Jimenez-Capdeville, M. E.;
Santos-Diaz, M. A.; Golden, A.; Rodriguez-Leyva, I.; Borja-Aburto, V.; Daz-
Barriga, F. (2001). "Exposure to Arsenic and Lead and Neuropsychological
Development in Mexican Children". Environmental Research 85 (2): 69
76. doi:10.1006/enrs.2000.4106.PMID 11161656.
97. Jump up^ Bouchard M.F., Sauv S., Barbeau B., Legrand M., Brodeur M..,
Bouffard T. et al. (2011). "Intellectual impairment in school-age children
exposed to manganese from drinking water" (PDF). Environmental Health
Perspectives 119 (1):
138. doi:10.1289/ehp.1002321. PMC 3018493. PMID 20855239.
98. ^ Jump up to:
a
b
Bouchard M.F., Chevrier J., Harley K.G., Kogut K., Vedar M.,
Calderon N. et al. (2011). "Prenatal exposure to organophosphate
pesticides and IQ in 7-year-old children". Environmental Health
Perspectives119 (8): 1189
95. doi:10.1289/ehp.1003185. PMC 3237357. PMID 21507776.
99. Jump up^ Rauh V., Arunajadai S., Horton M., Perera F., Hoepner L., Barr
D.B., Whyatt R. (2011). "Seven-year neurodevelopmental scores and
prenatal exposure to chlorpyrifos, a common agricultural
pesticide".Environmental Health Perspectives 119 (8): 1196
1201. doi:10.1289/ehp.1003160. PMC 3237355.PMID 21507777.
100. Jump up^ Bosquet Enlow, M.; Egeland, B.; Blood, E. A.; Wright, R. O.;
Wright, R. J. (2012). "Interpersonal trauma exposure and cognitive
development in children to age 8 years: A longitudinal study". Journal of
Epidemiology & Community Health 66 (11): 1005. doi:10.1136/jech-2011-
200727.
101. Jump up^ Low, J. A.; Handley-Derry, M. H.; Burke, S. O.; Peters, R. D.;
Pater, E. A.; Killen, H. L.; Derrick, E. J. (1992). "Association of intrauterine
fetal growth retardation and learning deficits at age 9 to 11
years".American journal of obstetrics and gynecology 167 (6): 1499
1505. doi:10.1016/0002-9378(92)91727-R.PMID 1471654.
Further reading[edit]
Berl MM, Duke ES, Mayo J, et al. (August 2010). "Functional anatomy of
listening and reading comprehension during development". Brain
Lang 114 (2): 115
25. doi:10.1016/j.bandl.2010.06.002.PMC 2962416. PMID 20656105.
Bishop DV, Anderson M, Reid C, Fox AM (2011). "Auditory development
between 7 and 11 years: an event-related potential (ERP) study". In
Koenig, Thomas. PLoS ONE 6 (5):
e18993.doi:10.1371/journal.pone.0018993. PMC 3090390. PMID 21573
058.
Friederici AD, Brauer J, Lohmann G (2011). "Maturation of the language
network: from inter- to intrahemispheric connectivities". In Rodriguez-
Fornells, Antoni. PLoS ONE 6 (6):
e20726.doi:10.1371/journal.pone.0020726. PMC 3113799. PMID 21695
183.
Giedd JN, Rapoport JL (September 2010). "Structural MRI of pediatric
brain development: what have we learned and where are we
going?". Neuron 67 (5): 728
34. doi:10.1016/j.neuron.2010.08.040.PMC 3285464. PMID 20826305.
Hu Z, Chan RC, McAlonan GM (2010). "Maturation of social attribution
skills in typically developing children: an investigation using the social
attribution task". Behav Brain Funct 6: 10. doi:10.1186/1744-9081-6-
10. PMC 2830993. PMID 20181076.
Jolles DD, Crone EA (2012). "Training the developing brain: a
neurocognitive perspective". Front Hum Neurosci 6:
76. doi:10.3389/fnhum.2012.00076. PMC 3321411. PMID 22509
161.
Mooney, Carol Garhart (2000). Theories of Childhood: an
Introduction to Dewey, Montessori, Erikson, Piaget & Vygotsky.
Redleaf Press. ISBN 1-884834-85-X.
Poulin-Dubois D, Brooker I, Chow V (2009). "The developmental
origins of nave psychology in infancy". Adv Child Dev Behav.
Advances in Child Development and Behavior 37: 55
104.doi:10.1016/S0065-2407(09)03702-
1. ISBN 9780123744708. PMID 19673160.
Stiles J, Jernigan TL (2010). "The basics of brain
development". Neuropsychol Rev 20 (4): 327
48.doi:10.1007/s11065-010-9148-
4. PMC 2989000. PMID 21042938.
Tau GZ, Peterson BS (January 2010). "Normal development of
brain circuits".Neuropsychopharmacology 35 (1): 147
68. doi:10.1038/npp.2009.115. PMC 3055433.PMID 19794405.
Vannest J, Karunanayaka PR, Schmithorst VJ, Szaflarski JP,
Holland SK (May 2009). "Language networks in children:
evidence from functional MRI studies". AJR Am J
Roentgenol 192 (5): 1190
6.doi:10.2214/AJR.08.2246. PMC 2791163. PMID 19380541.
Ninivaggi, F.J. (2013). Biomental Child Development: Perspectives
on Psychology and Parenting. Lanham, MD: Rowman &
Littlefield.
External links[edit]
Wikimedia
Commons
has media
related
to Child
development.
The Society for Research in Child Development (SRCD)
Child development, including developmental delays
Developmental Psychology: teaching about child development
Child Development Parenting Child Psychology Info
World Association for Infant Mental Health
Child Development Guide | Developmental Stages From Birth To Teens
It's the Parenting, Dodo | Living Hero Radio Show and Podcast special. With
Arun Gandhi telling 4 stories of growing up with Mahatma Gandhi's non-
violent parenting and childhood development practices and Dr. Marcy
Axness, author of Parenting for Peace giving parenting guidelines and
information. Jan 2013
[show]
V
T
E
Human biological and psychological development
[show]
V
T
E
Symptoms and signs: Speech and voice / Symptoms involving head and neck (R47R49, 784)
[show]
V
T
E
Mental and behavioral disorders (F 290319)
[show]
V
T
E
Developmental disorders: Dyslexia and related specific developmental disorders (F80F83, 315)
Retrieved from
"http://en.wikipedia.org/w/index.php?title=Child_development&oldid=59218795
5"
Categories:
Developmental psychology
Child development
Childhood
Hidden categories:
CS1 errors: dates
Pages containing cite templates with deprecated parameters
Articles needing additional medical references from August 2012
All articles needing additional references
All articles with unsourced statements
Articles with unsourced statements from August 2012
Articles to be expanded from June 2008
All articles to be expanded
Articles with unsourced statements from April 2012
Commons category template with no category set
Commons category with page title same as on Wikidata
Navigation menu
Personal tools
Create account
Log in
Namespaces
Article
Talk
Variants
Views
Read
Edit
Actions
View history
Search
Navigation
Main page
Contents
Featured content
Current events
Random article
Donate to Wikipedia
Wikimedia Shop
Interaction
Help
About Wikipedia
Community portal
Recent changes
Contact page
Tools
What links here
Related changes
Upload file
Special pages
Permanent link
Page information
Data item
Cite this page
Print/export
Create a book
Download as PDF
Printable version
Languages
Deutsch
Bahasa Melayu
Nederlands
Norsk bokml
Norsk nynorsk
Portugus
Simple English
Edit links
This page was last modified on 24 January 2014 at 16:03.
Text is available under the Creative Commons Attribution-ShareAlike
License; additional terms may apply. By using this site, you agree to
the Terms of Use and Privacy Policy.
Wikipedia is a registered trademark of the Wikimedia Foundation, Inc., a
non-profit organization.
Privacy policy
About Wikipedia
Disclaimers
Contact Wikipedia
Developers
Mobile view
You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Anatomy of Personality: The Lessons of Psychosurgery: - Prefrontal Leucotomy (By 1937)Document14 pagesThe Anatomy of Personality: The Lessons of Psychosurgery: - Prefrontal Leucotomy (By 1937)LouNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Children and Adolescent LiteratureDocument3 pagesChildren and Adolescent LiteratureMaiccah AcostaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Name: - Richardo Lingat - Course/Yr/Section: BSED EN 1-1 Date: - ScoreDocument2 pagesName: - Richardo Lingat - Course/Yr/Section: BSED EN 1-1 Date: - ScoreLingat RichardoNo ratings yet
- Follow Those Germs Grades 3-5Document3 pagesFollow Those Germs Grades 3-5CloroxClassroomNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Psyc110 Quiz & Final Exam Study GuideDocument5 pagesPsyc110 Quiz & Final Exam Study GuideEstela VelazcoNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- PRISMA-ScR TipSheet Item1-1 PDFDocument1 pagePRISMA-ScR TipSheet Item1-1 PDFRicardo PucinelliNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 100 Quotes From The Secret MovieDocument6 pages100 Quotes From The Secret MovieSUZANAMIKENo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Lesson PlanDocument3 pagesLesson PlanCrislyn AbergasNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Brand ElementsDocument4 pagesBrand ElementsHUỲNH TRẦN THIỆN PHÚCNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Finals Om: Student: Limheya Lester Glenn R. Prof: Geuel F. AusteDocument13 pagesFinals Om: Student: Limheya Lester Glenn R. Prof: Geuel F. AusteXXXXXXXXXXXXXXXXXX100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- US 244484 Demonstrate Knowledge UnderstandingDocument71 pagesUS 244484 Demonstrate Knowledge Understandingleburu rebaone0% (1)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Classroom Management January 3, 2022 FinalDocument46 pagesClassroom Management January 3, 2022 FinalMuhammad AliNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Modernism in LiteratureDocument14 pagesModernism in LiteratureFlorentina ŞugubeţuNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Oral Communication Module 6Document23 pagesOral Communication Module 6JamRey Vlogs100% (1)
- Best Practices Guide To Intervention: Teaching Students With Severe Emotional and Behavioral DisordersDocument101 pagesBest Practices Guide To Intervention: Teaching Students With Severe Emotional and Behavioral DisordersenaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Republic of The Philippines Cavite State University Don Severino Delas Alas Campus Indang, CaviteDocument3 pagesRepublic of The Philippines Cavite State University Don Severino Delas Alas Campus Indang, CaviteCorrine IvyNo ratings yet
- A Qualitative Study On Parents' Standards Influence On Grade 12 STEM Students Academic Performance at Jesus Is Lord Colleges FoundationDocument80 pagesA Qualitative Study On Parents' Standards Influence On Grade 12 STEM Students Academic Performance at Jesus Is Lord Colleges FoundationKevs PatsNo ratings yet
- Star Lesson Plan Math 7 6 15Document9 pagesStar Lesson Plan Math 7 6 15api-324335186No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Dark Side of EntrepreneurshipDocument13 pagesDark Side of EntrepreneurshipAmr AbdelMoneimNo ratings yet
- Integrated SkillsDocument17 pagesIntegrated SkillsAsaad Fakhri100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Behavior Flow ChartDocument1 pageBehavior Flow ChartVanessa HoffarthNo ratings yet
- Politeness PresentDocument41 pagesPoliteness Presentt3nee702No ratings yet
- 468 U N I T 4: Nursing Care of Clients With Alterations in Psychosocial AdaptationDocument1 page468 U N I T 4: Nursing Care of Clients With Alterations in Psychosocial AdaptationMercy JacobNo ratings yet
- 7 - Format Tugas Kontrak Kuliah Seminar On ELTDocument7 pages7 - Format Tugas Kontrak Kuliah Seminar On ELTYahya BadruzNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Chapter 4-Reflection 4 - CABALIDADocument5 pagesChapter 4-Reflection 4 - CABALIDAJeralyn CABALIDANo ratings yet
- Will You, As The Human Resource Department Head, Accept The Boss' Will You, As The Human Resource Department Head, Accept The Boss'Document2 pagesWill You, As The Human Resource Department Head, Accept The Boss' Will You, As The Human Resource Department Head, Accept The Boss'marichu apiladoNo ratings yet
- 15 Child PsychologyDocument46 pages15 Child PsychologyVesley B Robin100% (2)
- Jurnal-Ptk PKN Kelas 3 Penerapan Metode Demonstrasi Untuk Meningkatkan HaDocument11 pagesJurnal-Ptk PKN Kelas 3 Penerapan Metode Demonstrasi Untuk Meningkatkan HakangroisNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Bui Nguyen Phuong - Working - in - Profession - Learning - PortfolioDocument33 pagesBui Nguyen Phuong - Working - in - Profession - Learning - PortfolioNguyên Phương BùiNo ratings yet
- Edu WKP (2019) 15Document109 pagesEdu WKP (2019) 15Bruno OliveiraNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)