You might also like
- Ethics and Diversity in Artificial Intelligence PoDocument22 pagesEthics and Diversity in Artificial Intelligence PoDeniz Mete TAŞDEMİRNo ratings yet
- Chapter Three: Artificial IntelligenceDocument41 pagesChapter Three: Artificial IntelligenceEPHREM ENDASHAWNo ratings yet
- HR Project TopicsDocument13 pagesHR Project TopicsthariniadmiresNo ratings yet
- Make Decisions: NPA Discussion - NHS White Paper. 28 Jul 2010Document4 pagesMake Decisions: NPA Discussion - NHS White Paper. 28 Jul 2010Idrees MohammedNo ratings yet
- NetCracker SDN Solution BrochureDocument2 pagesNetCracker SDN Solution Brochureyappanappa100% (1)
- 3G Parameters For RF TechnologyDocument64 pages3G Parameters For RF TechnologyMubash87No ratings yet
- Software Project Management PDFDocument121 pagesSoftware Project Management PDFAjay Kalal100% (1)
- Impact of IT On HealthoutcomesDocument20 pagesImpact of IT On HealthoutcomesTransform Healthcare ITNo ratings yet
- Role of GP in NHSDocument61 pagesRole of GP in NHSS M Niaz MowlaNo ratings yet
- Cloud Computing Big Data TechnologyDocument2 pagesCloud Computing Big Data TechnologyAjaysen R VangoorNo ratings yet
- 3g Mobile ComputingDocument17 pages3g Mobile ComputingswethaTMRNo ratings yet
- CPOE/EHR ImplementationDocument21 pagesCPOE/EHR Implementationjunaid_alauddin5634No ratings yet
- Cybersecurity, Risk Management, and Financial CrimeDocument12 pagesCybersecurity, Risk Management, and Financial CrimeNico NathanaelNo ratings yet
- Application Migration Considerations For Cloud ComputingDocument5 pagesApplication Migration Considerations For Cloud ComputingNagendra SinghNo ratings yet
- Network Management SystemDocument10 pagesNetwork Management SystemMuhammad Moriandy GozaliNo ratings yet
- Summary of The NHS White Paper 2010Document5 pagesSummary of The NHS White Paper 2010dub2746No ratings yet
- Huawei ACU2 Wireless Access Controller DatasheetDocument12 pagesHuawei ACU2 Wireless Access Controller Datasheetdexater007No ratings yet
- GSM MO Call FlowDocument16 pagesGSM MO Call FlowVenkanna Annam100% (1)
- BIOMETRICSDocument31 pagesBIOMETRICSDev Kumar Mohanty100% (3)
- Effect of Workplace Environment On The PerformanceDocument14 pagesEffect of Workplace Environment On The Performancedion syahraniNo ratings yet
- Software Development Proposal TemplateDocument10 pagesSoftware Development Proposal Templatexuni34No ratings yet
- Chapter 6 - Service-Oriented Architecture (Lecture 8 & 9) - 1Document70 pagesChapter 6 - Service-Oriented Architecture (Lecture 8 & 9) - 1sibhat mequanintNo ratings yet
- GSM Call FlowDocument9 pagesGSM Call FloweidjuliNo ratings yet
- Chapter 5Document3 pagesChapter 5moksha.86No ratings yet
- Coverage and Performance Evaluation of Mobile Cellular Structured WiMAXDocument245 pagesCoverage and Performance Evaluation of Mobile Cellular Structured WiMAXsameh305100% (1)
- 4G. TechnologyDocument39 pages4G. TechnologySunny JamesNo ratings yet
- Analysis On Web 3 0 and EDU 3 0 CriteriaDocument9 pagesAnalysis On Web 3 0 and EDU 3 0 CriteriaMusafir AdamNo ratings yet
- RAN 3G Interfaces+ProtocolsDocument15 pagesRAN 3G Interfaces+ProtocolsTushar SrivastavaNo ratings yet
- Wight Paper DpiDocument17 pagesWight Paper DpiradislamyNo ratings yet
- Legal-Number Portability-Business Rules-Port Order Processes PDFDocument60 pagesLegal-Number Portability-Business Rules-Port Order Processes PDFMaxNo ratings yet
- Introduction To Packet TracerDocument10 pagesIntroduction To Packet TracerKevinz KerrNo ratings yet
- 2g 3g WLL Cellular ConceptDocument39 pages2g 3g WLL Cellular ConceptVinod KumbharNo ratings yet
- SEMP Template - ABC EducationDocument9 pagesSEMP Template - ABC EducationCVSCEducationFundNo ratings yet
- Assignment Brief Employability and Professional DevelopmentDocument6 pagesAssignment Brief Employability and Professional Developmentchandni081050% (2)
- Cafetele Telecom Training: We'Re Here To Help!Document10 pagesCafetele Telecom Training: We'Re Here To Help!Tammam_HajjNo ratings yet
- What Is Artificial Intelligence?: Data: InformationDocument177 pagesWhat Is Artificial Intelligence?: Data: InformationRajesh I SNo ratings yet
- A New Direction For Computer Architecture ResearchDocument10 pagesA New Direction For Computer Architecture ResearchdbpublicationsNo ratings yet
- Data Security in Local Network Using Distributed Firewall Seminar PresentationDocument28 pagesData Security in Local Network Using Distributed Firewall Seminar PresentationTiju SinghNo ratings yet
- Capstone Project ProposalDocument19 pagesCapstone Project ProposalHolly StephensNo ratings yet
- ForYourIrisOnly Brochure - Identity Management With Iris Recognition TechnologyDocument7 pagesForYourIrisOnly Brochure - Identity Management With Iris Recognition TechnologyIriTechIncNo ratings yet
- Handoff in Cellular Systems: Submitted By: Sireesha Vempati. Venkata Uppuluri. Vijaya PetlaDocument6 pagesHandoff in Cellular Systems: Submitted By: Sireesha Vempati. Venkata Uppuluri. Vijaya Petlaanc62No ratings yet
- IT Services Management - NotesDocument10 pagesIT Services Management - NotesVijay Thomas KurienNo ratings yet
- Sierra Wireless SCADA WhitepaperDocument10 pagesSierra Wireless SCADA WhitepapergayathiriNo ratings yet
- Online Job PortalDocument35 pagesOnline Job PortalPriya RathiNo ratings yet
- Wireless Sensor Networks The Basics Part I PDFDocument8 pagesWireless Sensor Networks The Basics Part I PDFAditya WijayantoNo ratings yet
- Telecommunications SectorDocument16 pagesTelecommunications Sectorpreeti25No ratings yet
- Cloud Computing: Helping Financial Institutions Leverage The Cloud To Improve IT EfficiencyDocument15 pagesCloud Computing: Helping Financial Institutions Leverage The Cloud To Improve IT EfficiencyIBMBankingNo ratings yet
- Cross Border RemittancesDocument36 pagesCross Border Remittanceselamurugan07No ratings yet
- M HealthDocument81 pagesM HealthAbebe ChekolNo ratings yet
- A Survey On Identity and Access ManagementDocument4 pagesA Survey On Identity and Access ManagementInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Topic 3 Computer Ethics: Mariano Marcos State University - College of Arts and Sciences - Department of Computer ScienceDocument7 pagesTopic 3 Computer Ethics: Mariano Marcos State University - College of Arts and Sciences - Department of Computer ScienceJamara Pucan100% (1)
- Prediction of Diabetes Using Classi Cation AlgorithmsDocument8 pagesPrediction of Diabetes Using Classi Cation AlgorithmsIrfan LasvegasNo ratings yet
- The Future InternetDocument17 pagesThe Future InternetITU-T Technology Watch100% (4)
- Strategic Planning Process and Background References PDFDocument11 pagesStrategic Planning Process and Background References PDFMarmie CamayangNo ratings yet
- Insur XDocument15 pagesInsur XJuan CumbradoNo ratings yet
- National Electricity Policy 2022 DraftDocument38 pagesNational Electricity Policy 2022 Draftsoumya sethyNo ratings yet
- The Network InfrastructureDocument5 pagesThe Network InfrastructureJil PatelNo ratings yet
- Digital Hospital ConsultancyDocument27 pagesDigital Hospital ConsultancymahaNo ratings yet
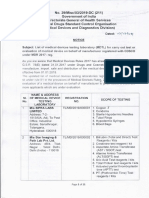
- List of MDTL Updated On 07 - 07 - 2021 - MED DEV TESTING LABS Listed by CdscoDocument11 pagesList of MDTL Updated On 07 - 07 - 2021 - MED DEV TESTING LABS Listed by CdscoRama VenugopalNo ratings yet
- India Heals 2020 - Indian ExhibitorsDocument2 pagesIndia Heals 2020 - Indian ExhibitorsRama VenugopalNo ratings yet
- NARAYANA Hrudayala - TariffDocument82 pagesNARAYANA Hrudayala - TariffRama VenugopalNo ratings yet
- Enterprise Performance Management For Healthcare OrganizationsDocument10 pagesEnterprise Performance Management For Healthcare OrganizationsRama VenugopalNo ratings yet
- Mahindra Group Sustainability Snapshot 2011-12Document36 pagesMahindra Group Sustainability Snapshot 2011-12Rama Venugopal100% (1)
- India Narayana 2008Document26 pagesIndia Narayana 2008Thameem Ul AnsariNo ratings yet
- NABH - Accreditation Timeline - Doc - HHDocument1 pageNABH - Accreditation Timeline - Doc - HHRama VenugopalNo ratings yet
- GlioblastomaDocument2 pagesGlioblastomaDaniela BulmagăNo ratings yet
- Nnaca Sop 302Document6 pagesNnaca Sop 302Thusitha LakpriyaNo ratings yet
- AMA Retrospective AuditsDocument2 pagesAMA Retrospective AuditsEma ForgacsNo ratings yet
- Reed - Reflection Paper Nurs631Document10 pagesReed - Reflection Paper Nurs631api-215994182No ratings yet
- Neonatal and Obstetric Risk Assessment (NORA) Pregnancy Cohort Study in SingaporeDocument7 pagesNeonatal and Obstetric Risk Assessment (NORA) Pregnancy Cohort Study in SingaporePremier PublishersNo ratings yet
- Cystic Fibrosis: Meet The Client: Debbie BakerDocument8 pagesCystic Fibrosis: Meet The Client: Debbie BakerJasjit Singh100% (1)
- Acute Viral Hepatitis: Jonathan WalaDocument49 pagesAcute Viral Hepatitis: Jonathan WalaAntony WaithakaNo ratings yet
- 2020 ESC Guidelines On Sports Cardiology and Exercise in Patients With Cardiovascular DiseaseDocument80 pages2020 ESC Guidelines On Sports Cardiology and Exercise in Patients With Cardiovascular DiseaseKlaraNo ratings yet
- Asthma Fullguideline 2009Document132 pagesAsthma Fullguideline 2009Lajwanti DesignersNo ratings yet
- Thesis Synopsis - Kiran RathiDocument4 pagesThesis Synopsis - Kiran RathiKiran RathiNo ratings yet
- Task 5 Case NotesDocument3 pagesTask 5 Case NotesGunawan MDNo ratings yet
- Medication AdministrationDocument3 pagesMedication AdministrationMonika SarmientoNo ratings yet
- Healthia Limited: Fill Your Boots!Document31 pagesHealthia Limited: Fill Your Boots!ashok yadavNo ratings yet
- AgonistsDocument25 pagesAgonistsOfficially RandomNo ratings yet
- Pharm MCQ BookDocument11 pagesPharm MCQ BookanojanNo ratings yet
- Doh Admin. 2010-0018Document29 pagesDoh Admin. 2010-0018Mar OrdanzaNo ratings yet
- L30 - FPSC Paper Mill Colony C38/1, Gurdwara Road, Siddheshwar LucknowDocument4 pagesL30 - FPSC Paper Mill Colony C38/1, Gurdwara Road, Siddheshwar LucknowShamsuddin ShamsNo ratings yet
- Siare Perseo - Service ManualDocument55 pagesSiare Perseo - Service ManualsolcarwxNo ratings yet
- Stress Hyperglycemia: Anand MosesDocument4 pagesStress Hyperglycemia: Anand MosesDaeng Arya01No ratings yet
- Eshre Guideline Endometriosis 2022Document192 pagesEshre Guideline Endometriosis 2022Patricia100% (1)
- Selective Awareness TherapyDocument10 pagesSelective Awareness TherapyHashem Al AttasNo ratings yet
- UNILABDocument6 pagesUNILABDaniel Nacorda0% (1)
- Vitreous Hemorrhage: Retina Eye Specialists Retina Eye SpecialistsDocument2 pagesVitreous Hemorrhage: Retina Eye Specialists Retina Eye SpecialistsMarcel Antek CivilNo ratings yet
- Glaucoma: by Tekia BuntynDocument18 pagesGlaucoma: by Tekia BuntynTekia BuntynNo ratings yet
- Nursing Care of The ElderlyDocument11 pagesNursing Care of The ElderlySpislgal PhilipNo ratings yet
- Nursing Care Plan For Inflammatory Bowel DiseaseDocument17 pagesNursing Care Plan For Inflammatory Bowel DiseaseLyka Joy DavilaNo ratings yet
- Unit 1 Chap 1 and 2Document7 pagesUnit 1 Chap 1 and 2Ariane Grace OcampoNo ratings yet
- 2UDocument47 pages2Uucnursingcesdev2008100% (3)
- Chakra-Chart Deborah KingDocument2 pagesChakra-Chart Deborah KingLaura Dafina Drãguț100% (2)
- Plan Your DrillDocument4 pagesPlan Your DrillStan BTOB,BTS,TXTNo ratings yet