You might also like
- MCQs and Orals - Past YrsDocument5 pagesMCQs and Orals - Past YrskazchandranNo ratings yet
- Question SetsDocument45 pagesQuestion SetskazchandranNo ratings yet
- 23 SENSESpractical EN1Document17 pages23 SENSESpractical EN1kazchandranNo ratings yet
- Lect Resp4dDocument93 pagesLect Resp4dkazchandranNo ratings yet
- Senses Prelab23 En1Document50 pagesSenses Prelab23 En1kazchandranNo ratings yet
- Senses Prelab23 En1Document50 pagesSenses Prelab23 En1kazchandranNo ratings yet
- Male Genitlect6aDocument111 pagesMale Genitlect6akazchandranNo ratings yet
- AudiometryDocument5 pagesAudiometrykazchandranNo ratings yet
- Anatomy I I QuestionsDocument5 pagesAnatomy I I QuestionskazchandranNo ratings yet
- Lect Skin4aDocument98 pagesLect Skin4akazchandranNo ratings yet
- The Aim of Medicine Is Not To Know The DiseaseDocument4 pagesThe Aim of Medicine Is Not To Know The DiseasekazchandranNo ratings yet
- Ultrasound: The Lecture ContentsDocument12 pagesUltrasound: The Lecture ContentskazchandranNo ratings yet
- AttachmentDocument6 pagesAttachmentkazchandranNo ratings yet
- Anatomy I - QuestionsDocument5 pagesAnatomy I - QuestionskazchandranNo ratings yet
- Program of Study: Course: Abbreviation: ScheduleDocument3 pagesProgram of Study: Course: Abbreviation: SchedulekazchandranNo ratings yet
- Program of Study: Course: Abbreviation: ScheduleDocument3 pagesProgram of Study: Course: Abbreviation: SchedulekazchandranNo ratings yet
- VAB11 06a Population GeneticsDocument54 pagesVAB11 06a Population GeneticskazchandranNo ratings yet
- Cancer - How To Get An A in BioDocument12 pagesCancer - How To Get An A in BiokazchandranNo ratings yet
- VAB11 ZAB11 Exam QuestionsDocument2 pagesVAB11 ZAB11 Exam QuestionskazchandranNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- ICSE Biology Notes Nervous System For 20 PDFDocument25 pagesICSE Biology Notes Nervous System For 20 PDFMmt RdcNo ratings yet
- Third Years Log BookDocument11 pagesThird Years Log BookMeenakshi Kumar100% (2)
- Cranial Nerves and Their Sensory Association NeuronsDocument3 pagesCranial Nerves and Their Sensory Association NeuronsAnny AlvrzNo ratings yet
- Designing For The BlindDocument38 pagesDesigning For The BlindBharani KumarNo ratings yet
- Bahrick & HollichDocument47 pagesBahrick & HollichAlexandra HuhNo ratings yet
- Colour Vision TestsDocument9 pagesColour Vision Testsbforte09No ratings yet
- Perception of Moevemmt PDFDocument6 pagesPerception of Moevemmt PDFAbrar AhmadNo ratings yet
- Clinical Orthoptics 2019Document97 pagesClinical Orthoptics 2019Joseph IsraelNo ratings yet
- Chapter-2 PERCEPTIONDocument29 pagesChapter-2 PERCEPTIONSuman BhandariNo ratings yet
- 08 Subjective Refraction AstigmatismDocument51 pages08 Subjective Refraction Astigmatismgenalinang100% (1)
- Accommodation InsufficiencyDocument5 pagesAccommodation InsufficiencyAmrit PokharelNo ratings yet
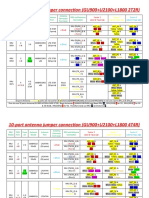
- Antennas Model & RRU Model (Use and Connection)Document11 pagesAntennas Model & RRU Model (Use and Connection)TheinHtayAungAungNo ratings yet
- What Is ColorDocument8 pagesWhat Is ColorCyprian ObiokoyeNo ratings yet
- Ophthalmic Epidemiology:: A Clouded VisionDocument31 pagesOphthalmic Epidemiology:: A Clouded Visionnutrifmeal arifNo ratings yet
- Approach To A Case of CataractDocument18 pagesApproach To A Case of CataractVineet GuptaNo ratings yet
- 10 6 Random Numbers 0 To 1Document5,001 pages10 6 Random Numbers 0 To 1sNo ratings yet
- Halstead-Reitan Battery of Neuropsychological TestsDocument14 pagesHalstead-Reitan Battery of Neuropsychological TestsSreesanth Kannoly50% (2)
- CataractsDocument72 pagesCataractsKusum RoyNo ratings yet
- Glaucoma Word FileDocument34 pagesGlaucoma Word Fileanon_784834955100% (1)
- Introduction To Psychology PSY 101: Lecture 4: Module 5 Sensation Lecturer: Catherine SesayDocument58 pagesIntroduction To Psychology PSY 101: Lecture 4: Module 5 Sensation Lecturer: Catherine SesayNgaima SesayNo ratings yet
- Primary Progression Test - Stage 3 English Paper 1 PDFDocument12 pagesPrimary Progression Test - Stage 3 English Paper 1 PDFkpjhun89% (18)
- CV Arief Revisi Februari 2016Document5 pagesCV Arief Revisi Februari 2016poetraNo ratings yet
- An Introduction To Design Thinking: Corey Ford Cford@stanford - EduDocument34 pagesAn Introduction To Design Thinking: Corey Ford Cford@stanford - EduTroy Rowe BrownNo ratings yet
- PSY101 Quiz 3290512Document7 pagesPSY101 Quiz 3290512Maya GeeNo ratings yet
- Phacoemulsification Versus Small Incision Cataract Surgery For Treatment ofDocument7 pagesPhacoemulsification Versus Small Incision Cataract Surgery For Treatment ofRagni MishraNo ratings yet
- Anisometropia PDFDocument2 pagesAnisometropia PDFIndhumathiNo ratings yet
- Morphologic Alterations On Posterior Iris-Claw Intraocular Lenses After Traumatic DisenclavationDocument5 pagesMorphologic Alterations On Posterior Iris-Claw Intraocular Lenses After Traumatic DisenclavationYanjinlkham Kh100% (1)
- Quick Guideto TympanometryDocument6 pagesQuick Guideto TympanometryWilhelm HeinleinNo ratings yet
- Weber TestDocument5 pagesWeber TestSuranewNo ratings yet
- MCQ Ophthalmo WITH AnswersDocument3 pagesMCQ Ophthalmo WITH AnswersEddie Lim100% (1)