You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Holstein Hargreaves Endo Topics 2003Document11 pagesHolstein Hargreaves Endo Topics 2003aninuraniyahNo ratings yet
- Holstein Hargreaves Endo Topics 2003Document11 pagesHolstein Hargreaves Endo Topics 2003aninuraniyahNo ratings yet
- Treated ExfoliativeDocument3 pagesTreated ExfoliativeaninuraniyahNo ratings yet
- Systemic Diseases Caused by Oral InfectionDocument12 pagesSystemic Diseases Caused by Oral InfectionaninuraniyahNo ratings yet
- Restoring Endodontically Treated TeethDocument20 pagesRestoring Endodontically Treated Teethlishenwong100% (1)
- Hand Hygiene GuideDocument2 pagesHand Hygiene GuideaninuraniyahNo ratings yet
- MucoceleDocument4 pagesMucoceleaninuraniyahNo ratings yet
- Literatur 2Document7 pagesLiteratur 2aninuraniyahNo ratings yet
- PULPOTOMIDocument8 pagesPULPOTOMIaninuraniyahNo ratings yet
- 4 PDFDocument3 pages4 PDFLanggeng Perdhana Jangan MenyerahNo ratings yet
- ExfoliativeDocument4 pagesExfoliativeaninuraniyahNo ratings yet
- Journal ReadingDocument4 pagesJournal ReadingVeny AlfianiNo ratings yet
- 4 PDFDocument3 pages4 PDFLanggeng Perdhana Jangan MenyerahNo ratings yet
- MucoceleDocument4 pagesMucoceleaninuraniyahNo ratings yet
- Eugenol 3Document7 pagesEugenol 3aninuraniyahNo ratings yet
- MucoceleDocument4 pagesMucoceleaninuraniyahNo ratings yet
- Eugenol 2Document6 pagesEugenol 2aninuraniyahNo ratings yet
- Journal ReadingDocument4 pagesJournal ReadingVeny AlfianiNo ratings yet
- EugenolDocument6 pagesEugenolaninuraniyahNo ratings yet
- Clinical tips for full veneer tooth preparationDocument7 pagesClinical tips for full veneer tooth preparationaninuraniyahNo ratings yet
- 5-Surgical Treatment of RanulaDocument5 pages5-Surgical Treatment of RanulaDevi AlfianiNo ratings yet
- SterilisasiDocument6 pagesSterilisasianinuraniyahNo ratings yet
- Micro-Marsupialization Technique For Mucocele On Ventral Tongue in 4-Year-8-Month Old ChildDocument2 pagesMicro-Marsupialization Technique For Mucocele On Ventral Tongue in 4-Year-8-Month Old ChildaninuraniyahNo ratings yet
- Ranula and Sublingual Salivary Gland ExcisionDocument4 pagesRanula and Sublingual Salivary Gland ExcisionaninuraniyahNo ratings yet
- Nursing Caries PedoDocument37 pagesNursing Caries PedoFourthMolar.comNo ratings yet
- Jop 2012 110716Document8 pagesJop 2012 110716aninuraniyahNo ratings yet
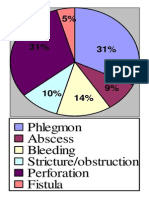
- Phlegmon Abscess Bleeding Stricture/obstruction Perforation FistulaDocument1 pagePhlegmon Abscess Bleeding Stricture/obstruction Perforation FistulaaninuraniyahNo ratings yet
- Gambaran Status KariesDocument9 pagesGambaran Status KariesaninuraniyahNo ratings yet
- Hand Hygiene GuideDocument2 pagesHand Hygiene GuideaninuraniyahNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Clinical Management of Orthodontic Root ResorbtionDocument142 pagesClinical Management of Orthodontic Root Resorbtionmarina_cretu1995No ratings yet
- Avulsed TeethDocument3 pagesAvulsed TeethSimona DobreNo ratings yet
- Endodontics: Colleagues ExcellenceDocument8 pagesEndodontics: Colleagues ExcellenceMitzi Noemi MorenoNo ratings yet
- Classification of Traumatic InjuriesDocument13 pagesClassification of Traumatic InjuriesbhavaaishuNo ratings yet
- Dental Trauma Professional PamphletDocument3 pagesDental Trauma Professional Pamphletnona aryan50% (2)
- Ellis FracturesDocument40 pagesEllis Fracturespriti adsulNo ratings yet
- Traumatic Dental Injuries, Management and Complications in School Going Children and Adolescents. An Update.Document8 pagesTraumatic Dental Injuries, Management and Complications in School Going Children and Adolescents. An Update.IJAR JOURNALNo ratings yet
- Traumatic InjuryDocument3 pagesTraumatic Injurymdio midoNo ratings yet
- Clinical EndoDocument16 pagesClinical EndoabdallahNo ratings yet
- IADT Guidlelines UpdateDocument5 pagesIADT Guidlelines Updateqiao fenNo ratings yet
- Pediatric Dentistry FinDocument66 pagesPediatric Dentistry FinAbdurhman MubarkNo ratings yet
- ABGD Written Study Questions 2007Document291 pagesABGD Written Study Questions 2007velangni100% (1)
- Orthodontic Update TruePDF-October 2019Document44 pagesOrthodontic Update TruePDF-October 2019Daniel DochioiuNo ratings yet
- Best Splinting Methods in Case of Dental Injury-A Literature ReviewDocument8 pagesBest Splinting Methods in Case of Dental Injury-A Literature ReviewGisela Pulido PatronNo ratings yet
- Reimplantation of Avulsed Tooth - A Case StudyDocument3 pagesReimplantation of Avulsed Tooth - A Case Studyrahul sharmaNo ratings yet
- Dental Trauma Flip Chart PermanentDocument2 pagesDental Trauma Flip Chart PermanentIuliaNo ratings yet
- Dental Injuries - Tony SkapetisDocument32 pagesDental Injuries - Tony SkapetisHesti RahayuNo ratings yet
- Dental Trauma Guide PDFDocument20 pagesDental Trauma Guide PDFLucianSerpescuNo ratings yet
- Sequelae of Traumatic Injuries To Primary Teeth PedoDocument32 pagesSequelae of Traumatic Injuries To Primary Teeth PedoFourthMolar.com100% (3)
- Jdhodt 01 00025Document6 pagesJdhodt 01 00025dithaNo ratings yet
- Reimplantation of Avulsed Primary Teeth in Children - A Systematic ReviewDocument9 pagesReimplantation of Avulsed Primary Teeth in Children - A Systematic ReviewKrishna KadamNo ratings yet
- IADT Guidelines for Managing Avulsed TeethDocument9 pagesIADT Guidelines for Managing Avulsed TeethHashem Motahir Ali Al-ShamiriNo ratings yet
- Emergency Mang TraumaDocument16 pagesEmergency Mang Traumaeliemaalouf4No ratings yet
- Anti Virus and Anti FungalDocument18 pagesAnti Virus and Anti FungalNicole Ava ChangNo ratings yet
- Of Dental Sciences: Case ReportDocument4 pagesOf Dental Sciences: Case ReportGede AnjasmaraNo ratings yet
- Endo-perio MCQ by Dr. A7md S3odiDocument35 pagesEndo-perio MCQ by Dr. A7md S3odimdio midoNo ratings yet
- 1-9 Iadt Guidelines Combined - LR - 11-5-2013Document27 pages1-9 Iadt Guidelines Combined - LR - 11-5-2013Pepo BelovedNo ratings yet
- P Endo LesionDocument68 pagesP Endo Lesionمحمد ابوالمجدNo ratings yet
- New Splinting Recommendation for Teeth Following TraumaDocument73 pagesNew Splinting Recommendation for Teeth Following TraumaSHRINIVAS GARJENo ratings yet
- Management of Luxation InjuriesDocument2 pagesManagement of Luxation InjuriesNur KamaliahNo ratings yet