You might also like
- Pharmacology Module PDFDocument23 pagesPharmacology Module PDFmirza_baig_46100% (1)
- SOP For Identification Techniques For Parasite Assays inDocument68 pagesSOP For Identification Techniques For Parasite Assays inDr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU Philippines100% (1)
- DIAGNOSTIC CYTOLOGY Notes (VetClinPath)Document4 pagesDIAGNOSTIC CYTOLOGY Notes (VetClinPath)Shirley Faye SalesNo ratings yet
- Special Veterinary Pathology: The Canadian Veterinary Journal. La Revue Veterinaire Canadienne February 1990Document2 pagesSpecial Veterinary Pathology: The Canadian Veterinary Journal. La Revue Veterinaire Canadienne February 1990Alonso Guardado100% (1)
- NEW ETHICS NNNNNNNNN)Document12 pagesNEW ETHICS NNNNNNNNN)Mulugeta100% (1)
- 2015 Proceeding - Management of The Patient With Canine Parvovirus EnteritisDocument7 pages2015 Proceeding - Management of The Patient With Canine Parvovirus EnteritisJHack2No ratings yet
- Birds and Exotics - MCannon PDFDocument42 pagesBirds and Exotics - MCannon PDFAl OyNo ratings yet
- Veterinary Clinical Pathology Clerkship ProgramDocument46 pagesVeterinary Clinical Pathology Clerkship ProgramDrVijayata ChoudharyNo ratings yet
- Clinical Pathology ReviewDocument11 pagesClinical Pathology Reviewrob hNo ratings yet
- Clinical Biochemistry - Clinical Pathology and Procedures - VetDocument9 pagesClinical Biochemistry - Clinical Pathology and Procedures - VetHimmet AslanNo ratings yet
- Characteristics of Hemostasis During Experimental Ehrlichia Canis InfectionDocument9 pagesCharacteristics of Hemostasis During Experimental Ehrlichia Canis InfectionDiana Granada100% (1)
- Veterinary PathologyDocument5 pagesVeterinary PathologyDrRakesh Raki100% (1)
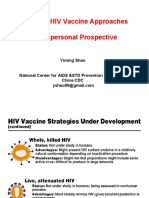
- Novel Vaccine Approaches (Yiming Shao)Document29 pagesNovel Vaccine Approaches (Yiming Shao)National Press Foundation100% (1)
- CANINE-Spontaneous Pneumothorax in DogsDocument7 pagesCANINE-Spontaneous Pneumothorax in Dogstaner_soysurenNo ratings yet
- Specialized Products From Amino Acids - Part 2Document16 pagesSpecialized Products From Amino Acids - Part 2Leon WarrenNo ratings yet
- Veterinary Basics1Document119 pagesVeterinary Basics1Saleem Ahmed Shahwani0% (1)
- Quality Assurance IN Histopathology: QC Should Consider The Whole ProcessDocument38 pagesQuality Assurance IN Histopathology: QC Should Consider The Whole Processalrasheed2020No ratings yet
- PrinsDocument44 pagesPrinsPalagiri MadhuNo ratings yet
- Anaemia in Dogs and Cats (Part 2) : Continuing EducationDocument6 pagesAnaemia in Dogs and Cats (Part 2) : Continuing EducationAchmad NugrohoNo ratings yet
- Pre Pubertal Gonadectomy in Dogs and Cats-Part IIIDocument5 pagesPre Pubertal Gonadectomy in Dogs and Cats-Part IIItaner_soysurenNo ratings yet
- #Spirochaetes & Mycoplasma#Document28 pages#Spirochaetes & Mycoplasma#Sarah PavuNo ratings yet
- Clinical Biochemistry: MSD Manual Veterinary ManualDocument5 pagesClinical Biochemistry: MSD Manual Veterinary ManualDursa MiressaNo ratings yet
- Anesthesia and Analgesia Book 1Document104 pagesAnesthesia and Analgesia Book 1JoanneYiNo ratings yet
- D1N3oS2crrS PDFDocument38 pagesD1N3oS2crrS PDFsharmasanjivNo ratings yet
- Post Parturient HemoglobinuriaDocument12 pagesPost Parturient HemoglobinuriaAli H. Sadiek أ.د. علي حسن صديق67% (3)
- Clinical Pathology Introductory LectureDocument14 pagesClinical Pathology Introductory Lecture11101955100% (1)
- Carbohydrate and Lipid MetabolismDocument47 pagesCarbohydrate and Lipid MetabolismShirley Faye SalesNo ratings yet
- Bacteriology Textbook 2009 PDFDocument298 pagesBacteriology Textbook 2009 PDFKrispinus SehandiNo ratings yet
- Cytologic Patterns - Eclinpath PDFDocument5 pagesCytologic Patterns - Eclinpath PDFJD46No ratings yet
- Project On Malaria 1Document9 pagesProject On Malaria 1Ankur BhatiaNo ratings yet
- Monografi AtropinDocument48 pagesMonografi AtropinWahyu AgustinaNo ratings yet
- The Result of Any Laboratory Test Is Only As Good As The Sample Received in The LaboratoryDocument16 pagesThe Result of Any Laboratory Test Is Only As Good As The Sample Received in The LaboratoryZeeshan YousufNo ratings yet
- Relevance of Serum Tumor MarkersDocument25 pagesRelevance of Serum Tumor MarkersDrPawan KirtaniNo ratings yet
- Suture MaterialDocument7 pagesSuture Materialtaner_soysuren100% (1)
- Principles, Applications and InterpretationsDocument64 pagesPrinciples, Applications and InterpretationsAbbi Yanto ArtNo ratings yet
- Techniques For Parasite Egg Identification in Faecal SamplesDocument9 pagesTechniques For Parasite Egg Identification in Faecal SamplesDr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU Philippines100% (2)
- Haemolysis i-WPS OfficeDocument69 pagesHaemolysis i-WPS OfficeIdrissa ContehNo ratings yet
- GIt HormonesDocument8 pagesGIt Hormonesriskyy1No ratings yet
- Inverse Polymerase Chain Reaction (Inverse PCR) Is A Variant of TheDocument8 pagesInverse Polymerase Chain Reaction (Inverse PCR) Is A Variant of TheNiraj Agarwal100% (1)
- Hints On Veterinary Ophthalmology: By/Sara Ahmed Hassouna BVSC, MSC Surgery Dept. Vet. Med. Alex. UniDocument39 pagesHints On Veterinary Ophthalmology: By/Sara Ahmed Hassouna BVSC, MSC Surgery Dept. Vet. Med. Alex. UniBibek SutradharNo ratings yet
- An Introduction To Antibodies and Their ApplicationsDocument100 pagesAn Introduction To Antibodies and Their ApplicationsAlessandroNo ratings yet
- 300 Questions and Answers in Radiography and Fluid Therapy For Veterinary Nurses - CawDocument4 pages300 Questions and Answers in Radiography and Fluid Therapy For Veterinary Nurses - CawsofalyruNo ratings yet
- MictobiologyDocument26 pagesMictobiologySaransh GhimireNo ratings yet
- Communicable Disease of The Gastro Intestinal TractDocument40 pagesCommunicable Disease of The Gastro Intestinal Tractɹǝʍdןnos100% (2)
- Outcomes of Dogs Undergoing Limb Amputation, Owner Satisfaction With Limb Amputation Procedures, and Owner Perceptions Regarding Postsurgical Adaptation: 64 Cases (2005-2012)Document7 pagesOutcomes of Dogs Undergoing Limb Amputation, Owner Satisfaction With Limb Amputation Procedures, and Owner Perceptions Regarding Postsurgical Adaptation: 64 Cases (2005-2012)William ChandlerNo ratings yet
- Veterinary Critical CareDocument15 pagesVeterinary Critical Caresudanfx100% (1)
- Vet CareplanexampleDocument6 pagesVet CareplanexampleAnonymous eJZ5HcNo ratings yet
- Fever of Unknown OriginDocument4 pagesFever of Unknown OriginPatricia PopNo ratings yet
- CestodesDocument34 pagesCestodesمصطفي خندقاويNo ratings yet
- Normal Dental Radiography in RabbitsDocument9 pagesNormal Dental Radiography in RabbitsMarcelo Anibal AlvarezNo ratings yet
- Lab Manual Hema 2Document16 pagesLab Manual Hema 2Charisse Ann ValdehuezaNo ratings yet
- Cep Halo SporinsDocument19 pagesCep Halo SporinsStarlet Rhonadez Bito-onon OrielNo ratings yet
- Veterinary Forensic ToxicologyDocument11 pagesVeterinary Forensic ToxicologyCarlos Alberto Chaves VelasquezNo ratings yet
- 3 Concentration Techniques SedimentationDocument18 pages3 Concentration Techniques SedimentationFatihah JahsmiNo ratings yet
- Tick Borne EncephalitisDocument7 pagesTick Borne Encephalitisขายหนังสือเตรียมสอบ เข้ามหาลัย ราคาถูกNo ratings yet
- Canine InsulinomaDocument5 pagesCanine Insulinomasoff4ikaNo ratings yet
- Lectured Veterinary GynecologyDocument1 pageLectured Veterinary GynecologygnpobsNo ratings yet
- Alpha Fetoprotein (Afp)Document10 pagesAlpha Fetoprotein (Afp)Andi UkengNo ratings yet
- 5 622647121207623762 PDFDocument13 pages5 622647121207623762 PDFNitin Kale100% (1)
- Veterinary ControversiesDocument3 pagesVeterinary Controversiestaner_soysurenNo ratings yet
- The Pattern Approach To Logic DiagnosisDocument12 pagesThe Pattern Approach To Logic Diagnosistaner_soysuren100% (1)
- Xylazine Sedation Antagonized With TolazolineDocument9 pagesXylazine Sedation Antagonized With Tolazolinetaner_soysurenNo ratings yet
- Treating Bone Deformities With Circular External Skeletal FixationDocument10 pagesTreating Bone Deformities With Circular External Skeletal Fixationtaner_soysurenNo ratings yet
- The Pituitary - Adrenal Axis and Pa Tho Physiology of HyperadrenocorticismDocument7 pagesThe Pituitary - Adrenal Axis and Pa Tho Physiology of Hyperadrenocorticismtaner_soysurenNo ratings yet
- Suture MaterialDocument7 pagesSuture Materialtaner_soysuren100% (1)
- Systemic Absorption of Topically Administered DrugsDocument8 pagesSystemic Absorption of Topically Administered Drugstaner_soysuren100% (2)
- Question Answer SessionDocument2 pagesQuestion Answer Sessiontaner_soysurenNo ratings yet
- Surgical Techniques For Extra Vascular Occlusiion of Tic ShuntsDocument7 pagesSurgical Techniques For Extra Vascular Occlusiion of Tic Shuntstaner_soysurenNo ratings yet
- Status Epilepticus-Patient Management and Pharmocologic TheraphyDocument7 pagesStatus Epilepticus-Patient Management and Pharmocologic Theraphytaner_soysuren100% (1)
- Status Epilepticus-Clinical Features and Pa Tho PhysiologyDocument8 pagesStatus Epilepticus-Clinical Features and Pa Tho Physiologytaner_soysurenNo ratings yet
- SOW-Feeding Management During Sow LactationDocument6 pagesSOW-Feeding Management During Sow Lactationtaner_soysuren100% (1)
- Small Animal Oxygen TherapyDocument10 pagesSmall Animal Oxygen Therapytaner_soysuren100% (1)
- Renal Effects of NSAIDDocument8 pagesRenal Effects of NSAIDtaner_soysurenNo ratings yet
- Pre Pubertal Gonadectomy in Dogs and Cats-Part IIIDocument5 pagesPre Pubertal Gonadectomy in Dogs and Cats-Part IIItaner_soysurenNo ratings yet
- Potential Adverse Effects of Long-Term Consumption of Fatty AcidsDocument11 pagesPotential Adverse Effects of Long-Term Consumption of Fatty Acidstaner_soysurenNo ratings yet
- Potassium BromideDocument2 pagesPotassium Bromidetaner_soysuren100% (1)
- Peripheral Parental NutritionDocument11 pagesPeripheral Parental Nutritiontaner_soysurenNo ratings yet
- Perianesthetic ArrhythmiasDocument10 pagesPerianesthetic Arrhythmiastaner_soysurenNo ratings yet
- Igorot Village: Get To Know..Document11 pagesIgorot Village: Get To Know..Elain RagosNo ratings yet
- Action, Desire and Subjectivity in Prabhakara MimamsaDocument28 pagesAction, Desire and Subjectivity in Prabhakara Mimamsasiddy_777No ratings yet
- Pnbcontr0223en (Web)Document308 pagesPnbcontr0223en (Web)James GeorgeNo ratings yet
- 2011 33 MaintenanceDocument16 pages2011 33 MaintenanceKrishna Khandige100% (1)
- Volume 2 Part 1 - Civil & Arch SpecificationsDocument173 pagesVolume 2 Part 1 - Civil & Arch Specificationsanish100% (1)
- Presentation On Anther Culture: Submitted To Submitted byDocument22 pagesPresentation On Anther Culture: Submitted To Submitted byvishnu0751No ratings yet
- Cutting Room Agility and ExcellenceDocument8 pagesCutting Room Agility and Excellenceperro perezNo ratings yet
- HCCI - Seminar Reports PPT PDF DOC PresentationDocument3 pagesHCCI - Seminar Reports PPT PDF DOC PresentationVenkatesh MohanNo ratings yet
- Air Cooler With Checking DoorDocument2 pagesAir Cooler With Checking DoorSuraj KumarNo ratings yet
- Podar International School (Icse) Practice Sheet STD: IX Chapter 28: Distance FormulaDocument2 pagesPodar International School (Icse) Practice Sheet STD: IX Chapter 28: Distance FormulaVanshika MehrotraNo ratings yet
- Edrolo ch3Document42 pagesEdrolo ch3YvonneNo ratings yet
- Baldor Motor TestDocument14 pagesBaldor Motor TestChecho BuenaventuraNo ratings yet
- Versana Premier Transducer GuideDocument4 pagesVersana Premier Transducer GuideDigo OtávioNo ratings yet
- QuestionsDocument6 pagesQuestionsRomeo martinezNo ratings yet
- AE451 Aerospace Engineering Design: Team HDocument140 pagesAE451 Aerospace Engineering Design: Team HÖmer Uğur ZayıfoğluNo ratings yet
- Safety Data Sheet: Section 1. Identification Jotun Essence Easy CleanDocument11 pagesSafety Data Sheet: Section 1. Identification Jotun Essence Easy CleanHồng PhongNo ratings yet
- History of DiamondsDocument21 pagesHistory of Diamondssilvernitrate1953No ratings yet
- NHouse SelfBuilder Brochure v2 Jan19 LowresDocument56 pagesNHouse SelfBuilder Brochure v2 Jan19 LowresAndrew Richard ThompsonNo ratings yet
- NTDCDocument8 pagesNTDCjaved_hanifNo ratings yet
- Sr. IBS DAS Consultant EngineerDocument4 pagesSr. IBS DAS Consultant EngineerMohamed KamalNo ratings yet
- Ficha-Tecnica-Tuberia MechDocument2 pagesFicha-Tecnica-Tuberia MechCarlos salazarNo ratings yet
- Meal Planning Guide e BookDocument7 pagesMeal Planning Guide e BookA'isha TijjaniNo ratings yet
- Chapter 1 Cumulative Review: Multiple ChoiceDocument2 pagesChapter 1 Cumulative Review: Multiple ChoiceJ. LeeNo ratings yet
- Conduit 5Document42 pagesConduit 5dediNo ratings yet
- Fractal Audio Footswitch Functions Guide PDFDocument22 pagesFractal Audio Footswitch Functions Guide PDFerikNo ratings yet
- Energy Thesis StatementDocument6 pagesEnergy Thesis Statementnicoledixonmobile100% (2)
- 2019 BMS1021 Practice Questions Answers PDFDocument12 pages2019 BMS1021 Practice Questions Answers PDFaskldhfdasjkNo ratings yet
- Sunday Afternoon, October 27, 2013: TechnologyDocument283 pagesSunday Afternoon, October 27, 2013: TechnologyNatasha MyersNo ratings yet
- Sip Dissertation - Final - Final For CollegeDocument17 pagesSip Dissertation - Final - Final For Collegevikashirulkar922No ratings yet
- Tsang Mui Millennium School 2019-2020 English Worksheet: Fill in The Blanks With The Correct Form of The VerbsDocument46 pagesTsang Mui Millennium School 2019-2020 English Worksheet: Fill in The Blanks With The Correct Form of The VerbscocoyipNo ratings yet
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (82)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4.5 out of 5 stars4.5/5 (6)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (254)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (60)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)