You might also like
- Reproductive Impact of Congenital Mu Llerian AnomaliesDocument5 pagesReproductive Impact of Congenital Mu Llerian AnomaliessasaNo ratings yet
- Gong Fei (Orcid ID: 0000-0003-3699-8776) Li Xihong (Orcid ID: 0000-0002-0986-760X)Document21 pagesGong Fei (Orcid ID: 0000-0003-3699-8776) Li Xihong (Orcid ID: 0000-0002-0986-760X)Clarithq LengguNo ratings yet
- Risk Factors Associated With Fetal Pleural Effusion in Prenatal Diagnosis: A Retrospective Study in A Single Institute in Southern ChinaDocument6 pagesRisk Factors Associated With Fetal Pleural Effusion in Prenatal Diagnosis: A Retrospective Study in A Single Institute in Southern Chinachristian roblesNo ratings yet
- Referensi No 7Document5 pagesReferensi No 7Bagus Wanda HabibullahNo ratings yet
- Endometriosis and Human Infertility: A New Investigation Into The Role of Eutopic EndometriumDocument8 pagesEndometriosis and Human Infertility: A New Investigation Into The Role of Eutopic Endometrium12ock312No ratings yet
- Hard Arson 2008Document7 pagesHard Arson 2008elda zulkarnainNo ratings yet
- VCUAM ClassificationDocument5 pagesVCUAM ClassificationpolygoneNo ratings yet
- Frequency and Types of Uterine Anomalies During Caesarean SectionDocument5 pagesFrequency and Types of Uterine Anomalies During Caesarean SectionBOONo ratings yet
- Midwifery Triage of First Trimester Bleeding: Susan A. Krause,, and Barbara W. GravesDocument12 pagesMidwifery Triage of First Trimester Bleeding: Susan A. Krause,, and Barbara W. GravesRival Risvaldi RusliNo ratings yet
- Evidence-Based Management of Endometrioma: Tarek A Gelbaya, Luciano G NardoDocument10 pagesEvidence-Based Management of Endometrioma: Tarek A Gelbaya, Luciano G NardofebrianoramadhanaNo ratings yet
- Fetal Structural Anomaly Screening at 11-14 Weeks of Gestation at Maharaj Nakorn Chiang Mai HospitalDocument6 pagesFetal Structural Anomaly Screening at 11-14 Weeks of Gestation at Maharaj Nakorn Chiang Mai HospitalobgynlaosNo ratings yet
- Occult Placenta Accreta: Risk Factors, Adverse Obstetrical Outcomes, and Recurrence in Subsequent PregnanciesDocument4 pagesOccult Placenta Accreta: Risk Factors, Adverse Obstetrical Outcomes, and Recurrence in Subsequent PregnanciesElla ChiraNo ratings yet
- Hum. Reprod.-2008-Bellver-278-84Document7 pagesHum. Reprod.-2008-Bellver-278-84Grigoriu RaduNo ratings yet
- The Prevalence of Congenital Uterine Anomalies in Unselected and High-Risk Populations A Systematic ReviewDocument11 pagesThe Prevalence of Congenital Uterine Anomalies in Unselected and High-Risk Populations A Systematic ReviewMoustafa KamelNo ratings yet
- Mullerian MalformationsDocument6 pagesMullerian MalformationsMau JkjlNo ratings yet
- Family History As A Risk Factor For Pelvic Organ Prolapse: Original ArticleDocument7 pagesFamily History As A Risk Factor For Pelvic Organ Prolapse: Original ArticlepakemainmainNo ratings yet
- An Analysis of Uterine Rupture at The Nnamdi AzikiweDocument5 pagesAn Analysis of Uterine Rupture at The Nnamdi AzikiweNublah Permata LestariNo ratings yet
- Findings in Uterine Biopsies Obtained by Laparotomy From Bitches With Unexplained Infertility or Pregnancy Loss: An Observational StudyDocument11 pagesFindings in Uterine Biopsies Obtained by Laparotomy From Bitches With Unexplained Infertility or Pregnancy Loss: An Observational Studyrafael molina bernalNo ratings yet
- Acupuncture For Uterine FibroidsDocument17 pagesAcupuncture For Uterine FibroidsTomas MascaroNo ratings yet
- Maternal and Obstetric Outcome of Women With Epilepsy 2009 SeizureDocument4 pagesMaternal and Obstetric Outcome of Women With Epilepsy 2009 Seizurebilal hadiNo ratings yet
- Endometriosis-Associated Infertility: Surgery and IVF, A Comprehensive Therapeutic ApproachDocument8 pagesEndometriosis-Associated Infertility: Surgery and IVF, A Comprehensive Therapeutic ApproachRangga AdityaNo ratings yet
- Risk Factors For Uterine Fibroids Among Women Undergoing Tubal SterilizationDocument8 pagesRisk Factors For Uterine Fibroids Among Women Undergoing Tubal SterilizationWahyu Tri KusprasetyoNo ratings yet
- Maternal Mortality and Associated Near-Misses Among Emergency Intrapartum Obstetric Referrals in Mulago Hospi...Document7 pagesMaternal Mortality and Associated Near-Misses Among Emergency Intrapartum Obstetric Referrals in Mulago Hospi...khotibNo ratings yet
- En Dome Trio 4Document7 pagesEn Dome Trio 4DONATA URBANINo ratings yet
- Management of Asherman's SyndromeDocument14 pagesManagement of Asherman's SyndromeEquipmed VenezuelaNo ratings yet
- NIH Public Access: Author ManuscriptDocument20 pagesNIH Public Access: Author ManuscriptJes LopNo ratings yet
- Detection of Chromosome Aberrations in TheDocument3 pagesDetection of Chromosome Aberrations in TheSonia Delgado EspinozaNo ratings yet
- Acute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisDocument6 pagesAcute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisIntan Wahyu CahyaniNo ratings yet
- Journal Pre-Proof: Journal of Pediatric and Adolescent GynecologyDocument18 pagesJournal Pre-Proof: Journal of Pediatric and Adolescent GynecologyCorey WoodsNo ratings yet
- Materials and MethodsDocument1 pageMaterials and MethodsImtihanamiseNo ratings yet
- Clinicopathological Study of Endometrium in Patients With Abnormal Uterine BleedingDocument7 pagesClinicopathological Study of Endometrium in Patients With Abnormal Uterine BleedingNazia BhatNo ratings yet
- Prenatal Management, Pregnancy and Pediatric Outcomes in Fetuses With Septated Cystic HygromaDocument5 pagesPrenatal Management, Pregnancy and Pediatric Outcomes in Fetuses With Septated Cystic HygromawitaNo ratings yet
- Histopathological Correlation of Abnormal Uterine BleedingDocument4 pagesHistopathological Correlation of Abnormal Uterine BleedingasclepiuspdfsNo ratings yet
- Clinical and Morphological Features of Uterine FibroidDocument7 pagesClinical and Morphological Features of Uterine FibroidCentral Asian StudiesNo ratings yet
- The Use of Acupuncture With in Vitro Fertilization: Is There A Point?Document10 pagesThe Use of Acupuncture With in Vitro Fertilization: Is There A Point?lu salviaNo ratings yet
- Endometriosis and The Neoplastic Process JurnalDocument12 pagesEndometriosis and The Neoplastic Process JurnalDhe'chi Sudah Tak Tul'lalitNo ratings yet
- ABORTIONDocument22 pagesABORTIONcacaNo ratings yet
- Obstetrical Outcomes in Women With ChorioamnionitisDocument6 pagesObstetrical Outcomes in Women With ChorioamnionitisCentral Asian StudiesNo ratings yet
- 2020 Article 1400Document10 pages2020 Article 1400Kim RamirezNo ratings yet
- Shehla PDFDocument4 pagesShehla PDFRahmayanti YuliaNo ratings yet
- Abnormal Uterine Bleeding in Perimenopausal WomenDocument15 pagesAbnormal Uterine Bleeding in Perimenopausal WomenOrchid LandNo ratings yet
- Genital Tract Fistulae in The Republic of Yemen, Sana'a - SciAlert Responsive VersionDocument11 pagesGenital Tract Fistulae in The Republic of Yemen, Sana'a - SciAlert Responsive VersionAli AlyousfeNo ratings yet
- Bhattacharya 2008Document7 pagesBhattacharya 2008Wh SquadNo ratings yet
- Gim 20047Document4 pagesGim 20047Sabhina AnseliaNo ratings yet
- Print 1 FixDocument10 pagesPrint 1 Fixafriskha bulawanNo ratings yet
- Causes of Congenital MalformationsDocument5 pagesCauses of Congenital MalformationsBenyam ZenebeNo ratings yet
- Adekanle Et AlDocument5 pagesAdekanle Et AlI_Ketut_Wahyu_MerthaNo ratings yet
- Pi Is 0002937811009379Document9 pagesPi Is 0002937811009379Mirza FinandarNo ratings yet
- Female Sterility and Her Paraclinical Care in Lubumbashi Inventory From 1998 To 2001Document5 pagesFemale Sterility and Her Paraclinical Care in Lubumbashi Inventory From 1998 To 2001International Journal of Innovative Science and Research TechnologyNo ratings yet
- High Rate of Uterine Rupture in A Conflict Setting of Hajjah, YemenDocument3 pagesHigh Rate of Uterine Rupture in A Conflict Setting of Hajjah, YemenShofi Dhia AiniNo ratings yet
- Journal Obgyne DR - ApDocument6 pagesJournal Obgyne DR - Apoktaviana54No ratings yet
- Srgype 02 00039 PDFDocument4 pagesSrgype 02 00039 PDFkhusnulNo ratings yet
- VACTERL Association in MARDocument4 pagesVACTERL Association in MARAnneSaputraNo ratings yet
- Prognostic Factors For Assisted Reproductive Technology in Women With Endometriosis-Related InfertilityDocument10 pagesPrognostic Factors For Assisted Reproductive Technology in Women With Endometriosis-Related InfertilityJunaedi SusantoNo ratings yet
- Vollenhoven B. Introduction: The Epidemiology of Uterine LeiomyomasDocument9 pagesVollenhoven B. Introduction: The Epidemiology of Uterine LeiomyomasRandilufti SantosoNo ratings yet
- Fallopian Tubes - Literature Review of Anatomy and Etiology in Female InfertilityDocument4 pagesFallopian Tubes - Literature Review of Anatomy and Etiology in Female InfertilityRekha KORANGANo ratings yet
- Fetal Cystic Hygroma The Importance of Natural HistoryDocument7 pagesFetal Cystic Hygroma The Importance of Natural HistoryNGUYỄN XUÂN SangNo ratings yet
- Fetal-Placental DisordersFrom EverandFetal-Placental DisordersNicholas S. AssaliRating: 5 out of 5 stars5/5 (1)
- Management of Infertility: A Practical ApproachFrom EverandManagement of Infertility: A Practical ApproachAntonio Simone LaganàNo ratings yet
- 1.emollients Prescribing Guideline Sept 2013Document4 pages1.emollients Prescribing Guideline Sept 2013kyle31No ratings yet
- Taking A Dermatological History - Dermatology - FastbleepDocument5 pagesTaking A Dermatological History - Dermatology - Fastbleepkyle31No ratings yet
- Necessary Elements of A Dermatologic History and Physical Evaluation PDFDocument9 pagesNecessary Elements of A Dermatologic History and Physical Evaluation PDFkyle31No ratings yet
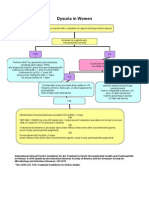
- Women With Dysuria AlgorhtmDocument1 pageWomen With Dysuria Algorhtmkyle31No ratings yet
- AntihypertensiveDocument1 pageAntihypertensivekyle31No ratings yet
- Marsupialization of A Bartholin's Cyst or AbscessDocument2 pagesMarsupialization of A Bartholin's Cyst or Abscesskyle31No ratings yet
- A Brief Review: The Epidemiology of Acquired Melanocytic NeviDocument9 pagesA Brief Review: The Epidemiology of Acquired Melanocytic Nevikyle31No ratings yet
- 2020-Study-Guide NinjaDocument248 pages2020-Study-Guide NinjaDalal Hazel100% (1)
- Real-Time PCR PDFDocument48 pagesReal-Time PCR PDFcontramondum1232039100% (1)
- Dow QuickFinder 2019-nCoV Kit-1Document8 pagesDow QuickFinder 2019-nCoV Kit-1German NarvaezNo ratings yet
- Managing GMP, HSE and HTA Regulations in Multiproduct ATMP ManufacturingDocument28 pagesManaging GMP, HSE and HTA Regulations in Multiproduct ATMP Manufacturingalnzeer omerNo ratings yet
- BiologyDocument4 pagesBiologyAbanggi k sangmaNo ratings yet
- XsxsxsDocument4 pagesXsxsxsBayu Ragil PangestuNo ratings yet
- GastricDocument142 pagesGastricMore MorenoNo ratings yet
- Anatomy & Physiology RenalDocument27 pagesAnatomy & Physiology RenalMuchamad Wisuda RiswantoNo ratings yet
- Cardiovascular and RespiratoryDocument51 pagesCardiovascular and RespiratoryAya PalomeraNo ratings yet
- Food Phreaking Issue 01: ISSN 2372-6504Document30 pagesFood Phreaking Issue 01: ISSN 2372-6504Marc PaulusmaNo ratings yet
- Protein Synthesis Notes and DiagramDocument34 pagesProtein Synthesis Notes and Diagramapi-267117865100% (1)
- Unit 7 - Vesicular MoleDocument43 pagesUnit 7 - Vesicular MoleN. Siva100% (1)
- Chronic Venous InsufficiencyDocument42 pagesChronic Venous InsufficiencyMeor FahmiNo ratings yet
- Clinical Applications of Artificial Intelligence and Machine Learning in Cancer Diagnosis - FutureDocument11 pagesClinical Applications of Artificial Intelligence and Machine Learning in Cancer Diagnosis - FutureVanroNo ratings yet
- Unit 1Document14 pagesUnit 1RajeshNo ratings yet
- Circulatory SystemDocument5 pagesCirculatory SystemTan XiangNo ratings yet
- Hyperemesis GravidarumDocument4 pagesHyperemesis GravidarumAaliyaan KhanNo ratings yet
- Osmosis Endocrine, Pathology - Tumors - Endocrine Tumors PDFDocument7 pagesOsmosis Endocrine, Pathology - Tumors - Endocrine Tumors PDFYusril Marhaen0% (1)
- Nutrition During Pregnancy and LactationDocument240 pagesNutrition During Pregnancy and LactationDede MashaNo ratings yet
- IFA Sports Nutrition Certification Test Answer Form: Tester: Date: NameDocument8 pagesIFA Sports Nutrition Certification Test Answer Form: Tester: Date: NameSimbarashe MabambeNo ratings yet
- Test Paper (Chegg Essay Evaluation)Document15 pagesTest Paper (Chegg Essay Evaluation)living smart lifestyleNo ratings yet
- Biology Discussion Animal Cell Culture - History, Types and ApplicationsDocument27 pagesBiology Discussion Animal Cell Culture - History, Types and ApplicationsManish SoniNo ratings yet
- What Is Dna and Its Importance in Humans BodyDocument1 pageWhat Is Dna and Its Importance in Humans BodyayeshaNo ratings yet
- Immunity Mark SchemeDocument6 pagesImmunity Mark SchemeDNo ratings yet
- 1 ChromosomesDocument9 pages1 ChromosomesOmprakash Kumar SinghNo ratings yet
- Atopic DermatitisDocument30 pagesAtopic DermatitislcaldezNo ratings yet
- Trisomy 21Document32 pagesTrisomy 21Alexandru EsteraNo ratings yet
- Outcome and Prognosis GDDDocument20 pagesOutcome and Prognosis GDDIfah Inayah D'zatrichaNo ratings yet
- GmosDocument5 pagesGmosapi-297206777100% (1)
- Bronchial AsthmaDocument40 pagesBronchial AsthmaNik Rose ElNo ratings yet