You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
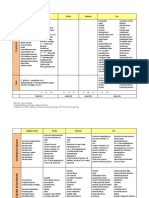
- Cat Muscles - Origin, Insertion, ActionDocument5 pagesCat Muscles - Origin, Insertion, ActionHarvey Domingo93% (29)
- Cat Muscles - Origin, Insertion, ActionDocument5 pagesCat Muscles - Origin, Insertion, ActionHarvey Domingo93% (29)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Practice Exam 1Document5 pagesPractice Exam 1Anonymous jSTkQVC27bNo ratings yet
- Concept Mapping - An Effective, Active Teaching-Learning MethodDocument7 pagesConcept Mapping - An Effective, Active Teaching-Learning MethodHarvey DomingoNo ratings yet
- Puberty and AdolescenceDocument3 pagesPuberty and AdolescenceHarvey Domingo100% (1)
- The Brachial PlexusDocument1 pageThe Brachial PlexusHarvey DomingoNo ratings yet
- The Brachial PlexusDocument1 pageThe Brachial PlexusHarvey Domingo100% (1)
- Bracket B CertificationDocument2 pagesBracket B CertificationHarvey DomingoNo ratings yet
- Bones - ChecklistDocument3 pagesBones - ChecklistHarvey DomingoNo ratings yet
- Why Have There Been No Great Women ArtistsDocument7 pagesWhy Have There Been No Great Women ArtistsHarvey DomingoNo ratings yet
- CV 2020Document3 pagesCV 2020api-519861494No ratings yet
- ICGH 2017 Proceeding Update ISBNDocument527 pagesICGH 2017 Proceeding Update ISBNRizki Robby NasutionNo ratings yet
- ICCB2019 ProceedingsDocument98 pagesICCB2019 Proceedingsdakic85No ratings yet
- Bishinik2002 10 OriginalDocument12 pagesBishinik2002 10 Originalalan woolardNo ratings yet
- Dust V - June 2011 EditDocument33 pagesDust V - June 2011 EditDust MagazineNo ratings yet
- CNS questions-WPS OfficeDocument39 pagesCNS questions-WPS OfficeEvidence ChaibvaNo ratings yet
- Neurology of Swallowing and DysphagiaDocument24 pagesNeurology of Swallowing and DysphagiaMaríaFernandaCampanoGacitúaNo ratings yet
- HTN and Arrh AfzalDocument8 pagesHTN and Arrh AfzalAFA.BLSNo ratings yet
- ICH Guidline AHADocument22 pagesICH Guidline AHABima GhovaroliyNo ratings yet
- Cerebrovascular DiseaseDocument13 pagesCerebrovascular DiseasebobtagubaNo ratings yet
- Stroke: BackgroundDocument10 pagesStroke: Backgroundjhay-r reyesNo ratings yet
- Tri County News Shopper, September 12, 2011Document24 pagesTri County News Shopper, September 12, 2011Pioneer GroupNo ratings yet
- Critical Care Nursing: Questions Bank and Model AnswerDocument70 pagesCritical Care Nursing: Questions Bank and Model AnswerHusseini ElghamryNo ratings yet
- Go Red For Women PresentationDocument31 pagesGo Red For Women PresentationadithiNo ratings yet
- Cerebrovascular AccidentDocument30 pagesCerebrovascular AccidentRichard Charles UmlasNo ratings yet
- Carotid Artery Disease FlyerDocument2 pagesCarotid Artery Disease Flyerdinh son myNo ratings yet
- Andrew MouldenDocument7 pagesAndrew Mouldenmika2k01100% (1)
- PIIS0007091220305663Document13 pagesPIIS0007091220305663Ana Belén Artero CastañoNo ratings yet
- The Effectiveness of PNF Method in Rehabilitation of Patients After Ischemic StrokeDocument18 pagesThe Effectiveness of PNF Method in Rehabilitation of Patients After Ischemic StrokeCristian Florin CrasmaruNo ratings yet
- Irfan Mir NotesDocument199 pagesIrfan Mir NotesSwathi AnantulaNo ratings yet
- MSM Sulphur For HealthDocument7 pagesMSM Sulphur For HealthMasterOfHotGlass100% (1)
- Medical Surgical Nursing Review 1Document422 pagesMedical Surgical Nursing Review 1jeshemaNo ratings yet
- Effectiveness of Proprioceptive Neuromuscular FacilitationDocument4 pagesEffectiveness of Proprioceptive Neuromuscular FacilitationMuhajir AjiNo ratings yet
- Quackery, The 20 Million Dollar DuckDocument20 pagesQuackery, The 20 Million Dollar DuckAustin Macauley Publishers Ltd.No ratings yet
- Platelet Aggregation Profile and Cardiovascular Event - Nani Parfati PDFDocument27 pagesPlatelet Aggregation Profile and Cardiovascular Event - Nani Parfati PDFdetaciNo ratings yet
- Eyes and Stroke The Visual Aspects of Cerebrovascular DiseaseDocument11 pagesEyes and Stroke The Visual Aspects of Cerebrovascular DiseaseAlessandro ZadraNo ratings yet
- Cardiovascular Benefits and Risks of Moderate Alcohol ConsumptionDocument26 pagesCardiovascular Benefits and Risks of Moderate Alcohol ConsumptionJessica BarcelonaNo ratings yet
- Stroke Syndromes - MCA, ACA, ICA, PCA, Vertebrobasilar Artery SDocument3 pagesStroke Syndromes - MCA, ACA, ICA, PCA, Vertebrobasilar Artery Sabu_abdisysyaakirNo ratings yet
- Stroke IskemikDocument6 pagesStroke IskemikVania Valentina100% (1)