You might also like
- Depression Conceptualization and Treatment: Dialogues from Psychodynamic and Cognitive Behavioral PerspectivesFrom EverandDepression Conceptualization and Treatment: Dialogues from Psychodynamic and Cognitive Behavioral PerspectivesChristos CharisNo ratings yet
- 2005, Vol.23, Issues 4, Psychocutaneous DiseaseDocument162 pages2005, Vol.23, Issues 4, Psychocutaneous DiseaseRizweta DestinNo ratings yet
- Improving the Mental Health Consultation: Introducing a short circuit tool to aid patient understanding and dispel stigmaFrom EverandImproving the Mental Health Consultation: Introducing a short circuit tool to aid patient understanding and dispel stigmaNo ratings yet
- Skin and PsycheDocument7 pagesSkin and PsycheGeorgios Lerios100% (1)
- Integrative Pathways: Navigating Chronic Illness with a Mind-Body-Spirit ApproachFrom EverandIntegrative Pathways: Navigating Chronic Illness with a Mind-Body-Spirit ApproachNo ratings yet
- Meditation Its EffectDocument11 pagesMeditation Its Effectmanisami7036No ratings yet
- Psycho Dermatology Basic Concepts AdvDocument4 pagesPsycho Dermatology Basic Concepts AdvLuther BlissettNo ratings yet
- Clinical Management in PsychodermatologyDocument294 pagesClinical Management in Psychodermatologymconsultorpsi100% (2)
- Stress and Skin Disorders, 2017Document257 pagesStress and Skin Disorders, 2017Elisa Carrera50% (4)
- Therapeutic Hotline Treatment of Prurigo Nodularis and Lichen Simplex Chronicus With GabapentinDocument6 pagesTherapeutic Hotline Treatment of Prurigo Nodularis and Lichen Simplex Chronicus With Gabapentinwilliam28asshole100% (1)
- Mohammad Jafferany, Katlein França - Geriatric Psychodermatology - Psychocutaneous Disorders in The Elderly-Nova Science Pub Inc (2015)Document295 pagesMohammad Jafferany, Katlein França - Geriatric Psychodermatology - Psychocutaneous Disorders in The Elderly-Nova Science Pub Inc (2015)Alexandra DobrescuNo ratings yet
- Object Relations TheoryDocument2 pagesObject Relations TheoryMonika Joseph0% (1)
- Psychiatry Notes For PGDocument8 pagesPsychiatry Notes For PGskycall28100% (1)
- See PsoriasisDocument12 pagesSee PsoriasisRobert HardakerNo ratings yet
- Trichotillomania An Important Psychocutaneous DisorderDocument5 pagesTrichotillomania An Important Psychocutaneous DisorderKatya LeyNo ratings yet
- Michael H. Antoni, Roselyn Smith-Stress Management Intervention For Women With Breast Cancer-Amer Psychological Assn (2003)Document222 pagesMichael H. Antoni, Roselyn Smith-Stress Management Intervention For Women With Breast Cancer-Amer Psychological Assn (2003)KmoespinoNo ratings yet
- 57 Psychopathology OCD 2007PDFDocument4 pages57 Psychopathology OCD 2007PDFLIDIYA MOL P VNo ratings yet
- Excoriation FaqDocument1 pageExcoriation FaqaladininsaneNo ratings yet
- Advances in Geriatric DermatologyDocument119 pagesAdvances in Geriatric DermatologyWILLIAM100% (1)
- Scoring System of DermatologyDocument11 pagesScoring System of DermatologyFitri FirdausiyaNo ratings yet
- Somatics Brochure Thymatron PDFDocument8 pagesSomatics Brochure Thymatron PDFCumhur TaşNo ratings yet
- Role of Homoeopathy in Psychological Disorders: January 2020Document6 pagesRole of Homoeopathy in Psychological Disorders: January 2020Madhu Ronda100% (1)
- Mirtazapine PDF PDFDocument23 pagesMirtazapine PDF PDFBoneGrissleNo ratings yet
- Chapter 27 - Anxiety-Related, Obsessive-Compulsive, Trauma and Stressor-Related, Somatic, and Dissociative DisordersDocument10 pagesChapter 27 - Anxiety-Related, Obsessive-Compulsive, Trauma and Stressor-Related, Somatic, and Dissociative DisordersKTNo ratings yet
- Wampold Specific IngredientsDocument7 pagesWampold Specific IngredientsJonathon BenderNo ratings yet
- Mill Shul Bert Williams 2012Document25 pagesMill Shul Bert Williams 2012AdityaTirtakusumaNo ratings yet
- Wood Lamp DermatologyDocument6 pagesWood Lamp Dermatologyindriyanti natasya ayu utami kotten100% (1)
- Ego Mechanisms of Defense and Personality Psychopathology PDFDocument7 pagesEgo Mechanisms of Defense and Personality Psychopathology PDFjansen9mawikereNo ratings yet
- A Case ExampleDocument10 pagesA Case ExampleCarole WanNo ratings yet
- PsychotherapyDocument49 pagesPsychotherapyionNo ratings yet
- Advances in Schizophrenia Research 2009Document461 pagesAdvances in Schizophrenia Research 2009Roberto CabreraNo ratings yet
- Offensive Deffensive - Stress and DTDocument5 pagesOffensive Deffensive - Stress and DTCristina EneNo ratings yet
- Psychopharmacology: Borderline Personality DisorderDocument7 pagesPsychopharmacology: Borderline Personality DisorderAwais FaridiNo ratings yet
- Psychotherapy For Treating Anxiety DisordersDocument11 pagesPsychotherapy For Treating Anxiety DisordersShaista ArshadNo ratings yet
- Journal Korn Complex TraumaDocument15 pagesJournal Korn Complex TraumaPsihoterapijaNo ratings yet
- OCD Relapse PreventionDocument8 pagesOCD Relapse PreventionElena Estrada DíezNo ratings yet
- Austin Journal of Multiple Sclerosis & NeuroimmunologyDocument14 pagesAustin Journal of Multiple Sclerosis & NeuroimmunologyAustin Publishing GroupNo ratings yet
- Emdr Choking PhobiaDocument12 pagesEmdr Choking PhobiaCatherine NENo ratings yet
- EMDR For Paraprofessional Use With Cism InterventionsDocument49 pagesEMDR For Paraprofessional Use With Cism InterventionsmiguelplenoNo ratings yet
- Transcranial Magnetic StimulationDocument8 pagesTranscranial Magnetic StimulationThonny EspinosaNo ratings yet
- MDMA-Assisted Psychotherapy Therapist Adherence and Competence Ratings ManualDocument38 pagesMDMA-Assisted Psychotherapy Therapist Adherence and Competence Ratings ManualCyberterton4No ratings yet
- 1999 Aversion Therapy-BEDocument6 pages1999 Aversion Therapy-BEprabhaNo ratings yet
- Use of Flash Technique On A GroupDocument1 pageUse of Flash Technique On A GroupElisa ValdésNo ratings yet
- PsychopharmacologyDocument49 pagesPsychopharmacologysazaki224No ratings yet
- Somatoform Disorders A Worldwide Perspective IDocument302 pagesSomatoform Disorders A Worldwide Perspective Ialex_crinaNo ratings yet
- PDF VersionDocument6 pagesPDF Versionservicesmi123100% (1)
- Treatments For Depression 1065502Document9 pagesTreatments For Depression 1065502api-548296191No ratings yet
- Knowledge Notes - Catie and Cutlass SummaryDocument3 pagesKnowledge Notes - Catie and Cutlass SummaryvinodksahuNo ratings yet
- Psychotherapy For Panic Disorder PDFDocument9 pagesPsychotherapy For Panic Disorder PDFdreaming100% (2)
- Aaron T. Beck, M.D.: Villaviray, Paulino III Cristino, Jomarie 3apsDocument12 pagesAaron T. Beck, M.D.: Villaviray, Paulino III Cristino, Jomarie 3apsRarajNo ratings yet
- Capitulo2-What Caracterizes Effective TherapistsDocument17 pagesCapitulo2-What Caracterizes Effective TherapistsMiriam Marques0% (1)
- Translate Kaplan Sadock Sinopsis Psikiatri Komprehensif Halaman 721 730 PDF FreeDocument76 pagesTranslate Kaplan Sadock Sinopsis Psikiatri Komprehensif Halaman 721 730 PDF FreeHadi GunaNo ratings yet
- Antidepressant Use in Adults With Chronic Kidney DiseaseDocument1 pageAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
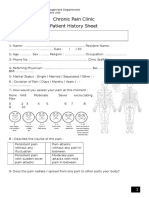
- Chronic Pain Clinic Patient History SheetDocument4 pagesChronic Pain Clinic Patient History SheetBelal N. MahfouzNo ratings yet
- Chapter 5 AnxietyDocument16 pagesChapter 5 AnxietyMark Jayson JuevesNo ratings yet
- Drug Free Nutrition For Brain ImbalancesDocument41 pagesDrug Free Nutrition For Brain ImbalancesricardfelipeNo ratings yet
- Ketamine SpecialistguidelinesonuseDocument12 pagesKetamine SpecialistguidelinesonuseDeboraNainggolanNo ratings yet
- BATHE TechniqueDocument3 pagesBATHE TechniqueYan Sheng HoNo ratings yet
- Clinical Interviewing. BMA 2017 Psychiatry Book of The YearDocument2 pagesClinical Interviewing. BMA 2017 Psychiatry Book of The Yearjohnny chawNo ratings yet
- Caarms ScaleDocument73 pagesCaarms ScaleAdon RamaNo ratings yet
- Neurostimulators in EpilepsyDocument5 pagesNeurostimulators in EpilepsyLuis Daniel Bernal CondeNo ratings yet
- Traditional Chinese Medicine For EpilepsyDocument31 pagesTraditional Chinese Medicine For EpilepsyLuis Daniel Bernal CondeNo ratings yet
- Neurologists' Knowledge of and Attitudes Toward Epilepsy Surgery A National SurveyDocument8 pagesNeurologists' Knowledge of and Attitudes Toward Epilepsy Surgery A National SurveyLuis Daniel Bernal CondeNo ratings yet
- Absolute Hospital Medicine ReviewDocument213 pagesAbsolute Hospital Medicine ReviewLuis Daniel Bernal Conde83% (6)
- Routine of Prenatal CareDocument85 pagesRoutine of Prenatal CareLuis Daniel Bernal CondeNo ratings yet
- Natriuretic Peptides in Heart Failure Should Therapy Be Guided by BNP LevelsDocument9 pagesNatriuretic Peptides in Heart Failure Should Therapy Be Guided by BNP LevelsLuis Daniel Bernal CondeNo ratings yet
- The Pathophysiology of Hypertension in Patients With ObesityDocument13 pagesThe Pathophysiology of Hypertension in Patients With ObesityLuis Daniel Bernal CondeNo ratings yet
- Diuretic Use in Renal DiseaseDocument10 pagesDiuretic Use in Renal DiseaseLuis Daniel Bernal CondeNo ratings yet
- Diuretic Use in Renal DiseaseDocument10 pagesDiuretic Use in Renal DiseaseLuis Daniel Bernal CondeNo ratings yet
- 2010 - Metabolic Acidosis - Pathophysiology, Diagnosis and ManagementDocument12 pages2010 - Metabolic Acidosis - Pathophysiology, Diagnosis and ManagementRodrigo Sigfrido BorgoñaNo ratings yet
- Neonatal SeizuresDocument13 pagesNeonatal SeizuresLuis Daniel Bernal CondeNo ratings yet
- Early Diagnosis of Minor Brain Damage in InfancyDocument7 pagesEarly Diagnosis of Minor Brain Damage in InfancyLuis Daniel Bernal CondeNo ratings yet
- Wound ManagementDocument12 pagesWound ManagementLuis Daniel Bernal CondeNo ratings yet
- Definitions and Classification of Hemolytic AnemiasDocument4 pagesDefinitions and Classification of Hemolytic AnemiasLuis Daniel Bernal CondeNo ratings yet
- An Integrated View of Potassium Homeostasis 2015Document13 pagesAn Integrated View of Potassium Homeostasis 2015Robert DinuNo ratings yet
- Diabetic Neuropathy-A ReviewDocument10 pagesDiabetic Neuropathy-A ReviewLuis Daniel Bernal CondeNo ratings yet
- The Endocannabinoid System and The BrainDocument27 pagesThe Endocannabinoid System and The BrainLuis Daniel Bernal CondeNo ratings yet
- The AnemiasDocument4 pagesThe AnemiasLuis Daniel Bernal CondeNo ratings yet
- κοινωνική φοβία μελέτη περίπτωσηςDocument4 pagesκοινωνική φοβία μελέτη περίπτωσηςEleni Tzanaki-ArnaoutakiNo ratings yet
- CBT EssayDocument16 pagesCBT EssayCristín Ní LiatháinNo ratings yet
- Anxiety - Symptoms, Types, Causes, Prevention, and TreatmentDocument12 pagesAnxiety - Symptoms, Types, Causes, Prevention, and Treatmentzandro padillaNo ratings yet
- Detailed Lesson Plan in MAPEH 5Document19 pagesDetailed Lesson Plan in MAPEH 5Lorie Mae CORPUZNo ratings yet
- Prokop HumanFearsDocument6 pagesProkop HumanFearsSamNo ratings yet
- Asynchronous Activity On Anxiety EDITABLEDocument7 pagesAsynchronous Activity On Anxiety EDITABLETrishaNo ratings yet
- Itp (Finals) - Psychological DisorderDocument6 pagesItp (Finals) - Psychological DisorderviyaleannahNo ratings yet
- Reading 6 M1 Scanning and SkimmingDocument2 pagesReading 6 M1 Scanning and SkimmingAshe FoxNo ratings yet
- Nursing Care Plan Dissociative... 2 JanDocument18 pagesNursing Care Plan Dissociative... 2 Janannu100% (1)
- The Promise of Energy Psychology Nexus PDF by Brendan D. MurphyDocument7 pagesThe Promise of Energy Psychology Nexus PDF by Brendan D. MurphyBrendan D. MurphyNo ratings yet
- Treatment of Anxiety in ChildrenDocument45 pagesTreatment of Anxiety in Childrenapi-285691153No ratings yet
- Chapter 4 Psychology NotesDocument12 pagesChapter 4 Psychology Notesaanya jainNo ratings yet
- Eating Anxiety PDFDocument9 pagesEating Anxiety PDFweber domingosNo ratings yet
- 1st Periodical Test Eng 8Document5 pages1st Periodical Test Eng 8Aira Monica PlancoNo ratings yet
- Augustson & Dougher (1997)Document11 pagesAugustson & Dougher (1997)CarminhaNo ratings yet
- Bard College of Fear by CarreauDocument4 pagesBard College of Fear by CarreauShaggy DNo ratings yet
- Psychiatric Nursing Notes by Dr. FaustoDocument377 pagesPsychiatric Nursing Notes by Dr. Faustopertru08100% (2)
- 2nd Week PresentationDocument30 pages2nd Week PresentationRevina LabradorNo ratings yet
- AP Psych - Psychological DisordersDocument6 pagesAP Psych - Psychological DisordersKloie WalkerNo ratings yet
- Assignmernt 9.1 Pscyological Disorder Part 1Document4 pagesAssignmernt 9.1 Pscyological Disorder Part 1Shana MariusNo ratings yet
- Symptoms and Causes: What Are Coulrophobia Triggers?Document4 pagesSymptoms and Causes: What Are Coulrophobia Triggers?Jessie Pasian Jr.No ratings yet
- Eng FileDocument6 pagesEng FileManuela MartelNo ratings yet
- Neurotic Dis.Document82 pagesNeurotic Dis.Lyka Mustika DelimaNo ratings yet
- Anxiety Dissorder PDFDocument273 pagesAnxiety Dissorder PDFdnaNo ratings yet
- Miley Cyrus Has A Twerking ProblemDocument2 pagesMiley Cyrus Has A Twerking ProblemJimmy TrinhNo ratings yet
- A History in Anxiety-From Hipocrates To DSM.Document7 pagesA History in Anxiety-From Hipocrates To DSM.Rox SalazarNo ratings yet
- The Correlation of Social Anxiety Towards The Behaviour of Grade 12 Students in SJDM Cornerstone College Inc.Document47 pagesThe Correlation of Social Anxiety Towards The Behaviour of Grade 12 Students in SJDM Cornerstone College Inc.Mark The PainterNo ratings yet
- Psychiatric Nursing 1Document11 pagesPsychiatric Nursing 1api-3731845100% (1)
- Fear of Public SpeakingDocument16 pagesFear of Public SpeakingSerc YablaNo ratings yet
- Psy 211 Writing Assignment 2Document4 pagesPsy 211 Writing Assignment 2api-285051253No ratings yet
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (24)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)