You might also like
- Spring Con Reg. 09Document7 pagesSpring Con Reg. 09YACNNED2869No ratings yet
- CIY Move 2008 Info PacketDocument5 pagesCIY Move 2008 Info Packetlarue23No ratings yet
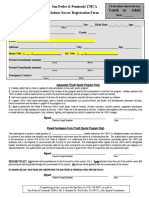
- Official Medical Information and Release FormDocument2 pagesOfficial Medical Information and Release FormtheNOLAtreeNo ratings yet
- Counselor ApplicationDocument6 pagesCounselor ApplicationAngelica WalkerNo ratings yet
- Teen MedicalDocument1 pageTeen MedicalJohn C StarkNo ratings yet
- Applicationb IIDocument7 pagesApplicationb IIreload99No ratings yet
- Greater Houston Area Chapter American Red Cross Youth Volunteer Application FormDocument6 pagesGreater Houston Area Chapter American Red Cross Youth Volunteer Application FormLauren KhooNo ratings yet
- 2015 Medical Consent FormDocument3 pages2015 Medical Consent Formapi-137720004No ratings yet
- CIY Liability FormDocument1 pageCIY Liability Formapi-3713285No ratings yet
- Parent/Guardian Information: Continued On ReverseDocument2 pagesParent/Guardian Information: Continued On Reverseadhi eng lrtNo ratings yet
- Staffer Search App FormDocument3 pagesStaffer Search App FormPamela Anne CanlasNo ratings yet
- Pds Medical-Cert Waiver 2023-RspcDocument1 pagePds Medical-Cert Waiver 2023-RspcRon MenesNo ratings yet
- Ministry Trip Application 10Document2 pagesMinistry Trip Application 10erichaysehkoNo ratings yet
- Return Completed (Both Sides) Registration Form With CheckDocument2 pagesReturn Completed (Both Sides) Registration Form With CheckFrancis HerouxNo ratings yet
- Registration 2010 2011Document3 pagesRegistration 2010 2011cubanita11No ratings yet
- 2014 15 y Bas Registration Form Clark PleasantDocument4 pages2014 15 y Bas Registration Form Clark Pleasantapi-231914240No ratings yet
- Lehigh Spring FestivalDocument1 pageLehigh Spring FestivalNerlynn2002No ratings yet
- Harambee Community Action Day: Please Return As Soon As PossibleDocument2 pagesHarambee Community Action Day: Please Return As Soon As Possibleapi-27159300No ratings yet
- CUMC Medical Consent 2010-2011Document1 pageCUMC Medical Consent 2010-2011Matthew Dunn-RankinNo ratings yet
- TN Umap ApplicationDocument1 pageTN Umap ApplicationtncircuitriderNo ratings yet
- Blank Permission SlipDocument1 pageBlank Permission Slipgraham5333No ratings yet
- 2016 Enrollment FormDocument5 pages2016 Enrollment Formapi-278479176No ratings yet
- Registration and ConsentDocument1 pageRegistration and ConsentcbcyouthNo ratings yet
- ST Pauls Camp Service TeamDocument2 pagesST Pauls Camp Service TeamJonathan CundanganNo ratings yet
- Registration and Medical ReleaseDocument1 pageRegistration and Medical Releaseelizabeth_nabil2452No ratings yet
- Socalmmr2012 Consent FormDocument1 pageSocalmmr2012 Consent FormohjulienneNo ratings yet
- Youth Permission SlipDocument1 pageYouth Permission SlipazaleaeducationNo ratings yet
- 2012 Staff AppDocument2 pages2012 Staff Applindy7190No ratings yet
- Sky-Zone Medical ReleaseDocument1 pageSky-Zone Medical ReleaseSteve GilletteNo ratings yet
- Rady Childrens HospitalDocument6 pagesRady Childrens HospitalTom HeavenNo ratings yet
- Pac Audition FormDocument1 pagePac Audition FormJade Marie Gatungan SorillaNo ratings yet
- GAL Application - Become A GAL in SCDocument5 pagesGAL Application - Become A GAL in SCWylde FaerieNo ratings yet
- Referral FormDocument2 pagesReferral FormRANDY BAOGBOG100% (1)
- SWFLC - Volunteer-ApplicationDocument4 pagesSWFLC - Volunteer-Applicationapi-237649615No ratings yet
- Adult Volunteer ApplicationDocument2 pagesAdult Volunteer ApplicationAmy Gibson100% (2)
- T-Shirt Size (Adult Sizes) Xs SM Med LG XL XXLDocument3 pagesT-Shirt Size (Adult Sizes) Xs SM Med LG XL XXLmainstageNo ratings yet
- General Release / Permission Form: ACTIVITIES: (Initial All That Apply)Document2 pagesGeneral Release / Permission Form: ACTIVITIES: (Initial All That Apply)Megan JonesNo ratings yet
- 2008/2009 Bethany Baptist Church - SM Permission/Waiver FormDocument4 pages2008/2009 Bethany Baptist Church - SM Permission/Waiver FormjdbroozerNo ratings yet
- Thanksgiving Church Mission Application Form: Personal DataDocument6 pagesThanksgiving Church Mission Application Form: Personal Datastelin90No ratings yet
- ChristianEdRegistration2017 2018Document2 pagesChristianEdRegistration2017 2018jgm4551No ratings yet
- ASY Reg Summercamp2012Document2 pagesASY Reg Summercamp2012ASYMCA YCONo ratings yet
- Intake Sheet For VAWCDocument2 pagesIntake Sheet For VAWCDaisy Palero Tibayan88% (8)
- PPCRV Volunteer Application FormDocument1 pagePPCRV Volunteer Application FormCARES Martin Federic Palco33% (3)
- YMCA Youth Indoor Soccer Registration FormDocument1 pageYMCA Youth Indoor Soccer Registration FormRalph BracamonteNo ratings yet
- Registration Form 2011Document4 pagesRegistration Form 2011Charles Autumn GwynnNo ratings yet
- Globalization, Coffee and Justice in Chiapas, Mexico: Witness For Peace Travel Program ApplicationDocument4 pagesGlobalization, Coffee and Justice in Chiapas, Mexico: Witness For Peace Travel Program ApplicationStan DuncanNo ratings yet
- Mission San Luis Rey Parish "New Student" Registration Form ENGLISH FAITH FORMATION 2012-2013 SemesterDocument4 pagesMission San Luis Rey Parish "New Student" Registration Form ENGLISH FAITH FORMATION 2012-2013 SemestersanluisreyparishNo ratings yet
- Ril FormDocument1 pageRil Formapi-400016232100% (1)
- Health FormDocument2 pagesHealth Formapi-247535323No ratings yet
- 2013 Spring Summe BrochureDocument8 pages2013 Spring Summe Brochurejvirchow17No ratings yet
- Membership FormDocument2 pagesMembership Formmjrt2006No ratings yet
- Core Team 22-23 RegistrationDocument8 pagesCore Team 22-23 Registrationjakertomay7No ratings yet
- TEMPLATE Medical Release WITHOUT Notary 1Document1 pageTEMPLATE Medical Release WITHOUT Notary 1Peter WagnerNo ratings yet
- Background Check FormDocument2 pagesBackground Check Formapi-256948363No ratings yet
- 2013 Spring Summer BrochureDocument8 pages2013 Spring Summer Brochurejvirchow17No ratings yet
- PDS Medical RSPCDocument1 pagePDS Medical RSPCMyka Andrea GarciaNo ratings yet
- Youth Rally 2014 Health Form PDFDocument1 pageYouth Rally 2014 Health Form PDFJordan ForstonNo ratings yet
- 2010 YP Magazine CoverDocument1 page2010 YP Magazine CoverbradfiscusNo ratings yet
- GPWV Team ScoresDocument1 pageGPWV Team ScoresbradfiscusNo ratings yet
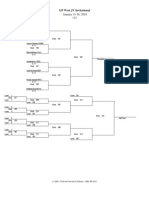
- January 15-16, 2010 112: GP West JV InvitationalDocument13 pagesJanuary 15-16, 2010 112: GP West JV InvitationalbradfiscusNo ratings yet
- TN Conference Color CoverDocument2 pagesTN Conference Color CoverbradfiscusNo ratings yet
- January 15-16, 2010 103: GP West InvitationalDocument28 pagesJanuary 15-16, 2010 103: GP West InvitationalbradfiscusNo ratings yet
- WNW 2010 Description of WorkshopsDocument5 pagesWNW 2010 Description of WorkshopsbradfiscusNo ratings yet
- WNW Tshirt Order FormDocument1 pageWNW Tshirt Order FormbradfiscusNo ratings yet
- Final Team ScoresDocument1 pageFinal Team ScoresbradfiscusNo ratings yet
- Independence Holiday TournamentDocument1 pageIndependence Holiday TournamentbradfiscusNo ratings yet
- Indy Pre Tournament BracketsDocument65 pagesIndy Pre Tournament BracketsbradfiscusNo ratings yet
- EpworthhistoricalbookDocument60 pagesEpworthhistoricalbookbradfiscusNo ratings yet
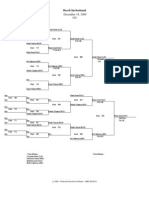
- December 19, 2009 103: Beech InvitationalDocument14 pagesDecember 19, 2009 103: Beech InvitationalbradfiscusNo ratings yet
- YPM Registration FormDocument3 pagesYPM Registration FormbradfiscusNo ratings yet
- WNW 2010 Leader's Guide FinalDocument15 pagesWNW 2010 Leader's Guide FinalbradfiscusNo ratings yet
- Sonic Final Team ScoresDocument1 pageSonic Final Team ScoresbradfiscusNo ratings yet