You might also like
- Spanish PhrasebookDocument126 pagesSpanish PhrasebookSky Sage100% (4)
- TCM Tongue Diagnosis - Complete Health and HappinessDocument17 pagesTCM Tongue Diagnosis - Complete Health and HappinessmusatiiNo ratings yet
- Biomechanics NotesDocument21 pagesBiomechanics Notesstarlight9394100% (1)
- Guidelines For The Prevention of Intravascular Catheter-Related InfectionsDocument36 pagesGuidelines For The Prevention of Intravascular Catheter-Related InfectionsasupicuNo ratings yet
- Health Facilities and Services Regulatory Bureau: Republic of The Philippines Department of HealthDocument23 pagesHealth Facilities and Services Regulatory Bureau: Republic of The Philippines Department of HealthChamee MallillinNo ratings yet
- Pediatric Ophthalmology and Strabismus - David TaylorDocument1,180 pagesPediatric Ophthalmology and Strabismus - David TaylorEvelyn Sepulveda92% (12)
- 1 Prismaflexcrrtintro Seg12007 110326040426 Phpapp02Document38 pages1 Prismaflexcrrtintro Seg12007 110326040426 Phpapp02Sami Maghrebi100% (1)
- Border Molding & Vent HolesDocument4 pagesBorder Molding & Vent HolesGina Kissey100% (1)
- Development of The Digestive SystemDocument90 pagesDevelopment of The Digestive Systemyusrah mukhtarNo ratings yet
- Typhoid Fever GraphsDocument9 pagesTyphoid Fever GraphsMarjoree MedianaNo ratings yet
- Trend and Disease Burden of Bacillary Dysentery in China (1991-2000)Document9 pagesTrend and Disease Burden of Bacillary Dysentery in China (1991-2000)Rosa ArrascueNo ratings yet
- Risk Factors Associated With Typhoid Fever in Children Aged 2-16 Years in Karachi, PakistanDocument9 pagesRisk Factors Associated With Typhoid Fever in Children Aged 2-16 Years in Karachi, PakistandianislamiatyNo ratings yet
- A Study of Typhoid Fever in Five Asian Countries: Disease Burden and Implications For ControlsDocument4 pagesA Study of Typhoid Fever in Five Asian Countries: Disease Burden and Implications For ControlsPutu SuartiniNo ratings yet
- Adults' Perceived Prevalence of Enteric Fever Predicts Laboratory-Validated Incidence of Typhoid Fever in ChildrenDocument12 pagesAdults' Perceived Prevalence of Enteric Fever Predicts Laboratory-Validated Incidence of Typhoid Fever in ChildrenAnonymous 4OuVwgoNNuNo ratings yet
- Pmid 36550736 IpiDocument6 pagesPmid 36550736 Ipiajaya basnetNo ratings yet
- Risk Factors Associated With Typhoid Fever in Children Aged 2-16 Years in Karachi, PakistanDocument9 pagesRisk Factors Associated With Typhoid Fever in Children Aged 2-16 Years in Karachi, Pakistandwiwahyu ningsihNo ratings yet
- Ak 2011Document6 pagesAk 2011bouchra8blsNo ratings yet
- Risk Factors Associated With Typhoid Fever in Children Aged 216 Years in Karachi PakistanDocument8 pagesRisk Factors Associated With Typhoid Fever in Children Aged 216 Years in Karachi Pakistanامتیاز ہاشم بزنجوNo ratings yet
- Research Article: Viral Agents of Diarrhea in Young Children in Two Primary Health Centers in Edo State, NigeriaDocument6 pagesResearch Article: Viral Agents of Diarrhea in Young Children in Two Primary Health Centers in Edo State, NigeriariniNo ratings yet
- Research ArticleDocument9 pagesResearch ArticleTauhannyNo ratings yet
- Ajol File Journals - 233 - Articles - 208047 - Submission - Proof - 208047 2773 517395 1 10 20210602Document6 pagesAjol File Journals - 233 - Articles - 208047 - Submission - Proof - 208047 2773 517395 1 10 20210602Musa ZiramiNo ratings yet
- 2016 Article 1977Document10 pages2016 Article 1977Claudia NeculoiuNo ratings yet
- Denguetrend IJMRDocument8 pagesDenguetrend IJMRAshutosh TiwariNo ratings yet
- Catheter-Associated Urinary Tract Infections in Intensive Care Unit PatientsDocument7 pagesCatheter-Associated Urinary Tract Infections in Intensive Care Unit PatientsHaris AnsarNo ratings yet
- Healthcare: Allergic Rhinitis and Laryngeal Pathology: Real-World EvidenceDocument9 pagesHealthcare: Allergic Rhinitis and Laryngeal Pathology: Real-World EvidencePutri Rizky AmaliaNo ratings yet
- Epidemiology of Secondary Peritonitis: Analysis of 545 CasesDocument6 pagesEpidemiology of Secondary Peritonitis: Analysis of 545 CasesIntan KarmilaNo ratings yet
- Infection Status of Hospitalized Diarrheal Patients With Gastrointestinal Protozoa, Bacteria, and Viruses in The Republic of KoreaDocument9 pagesInfection Status of Hospitalized Diarrheal Patients With Gastrointestinal Protozoa, Bacteria, and Viruses in The Republic of KoreaMelia Kusuma WardaniNo ratings yet
- Aniwada 1332015 BJMMR23249 DSNDocument11 pagesAniwada 1332015 BJMMR23249 DSNelias aniwadaNo ratings yet
- s0895 4356 - 2899 - 2900231 020170725 19043 153tn3d With Cover Page v2Document8 pagess0895 4356 - 2899 - 2900231 020170725 19043 153tn3d With Cover Page v2HAMNA ZAINABNo ratings yet
- Covid 19 Patients' Clinical Characteristics, Discharge Rate, and Fatality Rate of Meta AnalysisDocument7 pagesCovid 19 Patients' Clinical Characteristics, Discharge Rate, and Fatality Rate of Meta AnalysisDelfina RubioNo ratings yet
- Etiologic and Epidemiologic Analysis of Hand FootDocument9 pagesEtiologic and Epidemiologic Analysis of Hand FootAisah AisahNo ratings yet
- Rota Vietnam EE FisherDocument7 pagesRota Vietnam EE FisherKartavya TiwariNo ratings yet
- Geographic Pattern of Typhoid Fever in India: A Model-Based Estimate of Cohort and Surveillance DataDocument9 pagesGeographic Pattern of Typhoid Fever in India: A Model-Based Estimate of Cohort and Surveillance DataYogesh MedewarNo ratings yet
- Fetch ObjectDocument7 pagesFetch ObjectBilly UntuNo ratings yet
- TetanusDocument5 pagesTetanusejaejaeja6No ratings yet
- Clinical Characteristics of Children With Coronavirus Disease 2019 in Hubei, ChinaDocument6 pagesClinical Characteristics of Children With Coronavirus Disease 2019 in Hubei, ChinaBobanBisercicNo ratings yet
- Wabah TBC Di VietnamDocument8 pagesWabah TBC Di VietnamSatya WangsaNo ratings yet
- Ijn 27 440Document6 pagesIjn 27 440Arun SedhainNo ratings yet
- 2018 Monitoring and Detection of Leprosy Patients in Southest China A Retrospective Study 2010 - 2014Document8 pages2018 Monitoring and Detection of Leprosy Patients in Southest China A Retrospective Study 2010 - 2014Jorge RicardoNo ratings yet
- Journal Pre-Proof: International Journal of Infectious DiseasesDocument14 pagesJournal Pre-Proof: International Journal of Infectious DiseasesKenya EspinozaNo ratings yet
- CKD 19 2 118Document7 pagesCKD 19 2 118GritoNo ratings yet
- Video 4 PDFDocument9 pagesVideo 4 PDFMirza RisqaNo ratings yet
- Potential Transmision HAI by Non Critical ProductDocument8 pagesPotential Transmision HAI by Non Critical ProductSofyan FauziNo ratings yet
- Prevalence of Tuberculosis in Faridabad District, Haryana State, IndiaDocument8 pagesPrevalence of Tuberculosis in Faridabad District, Haryana State, IndianovireandysasmitaNo ratings yet
- Salmonella Paratyphi A Rates AsiaDocument3 pagesSalmonella Paratyphi A Rates Asiasuryanti meilindaNo ratings yet
- Priorities For Research and Control of Cestode Zoonoses in AsiaDocument11 pagesPriorities For Research and Control of Cestode Zoonoses in AsiahansmeetNo ratings yet
- The Rise of Imported Dengue Infections in Victoria, Australia, 2010-2016Document11 pagesThe Rise of Imported Dengue Infections in Victoria, Australia, 2010-2016Satriya WibawaNo ratings yet
- DengueclinicaliranianjDocument13 pagesDengueclinicaliranianjKeshav ShandilyaNo ratings yet
- 1 s2.0 S1201971219304229 MainDocument10 pages1 s2.0 S1201971219304229 MainAlleidya SalsabiillaNo ratings yet
- Dengue Clini Calir AnianjDocument13 pagesDengue Clini Calir Anianjmeceda8565No ratings yet
- Demographic and Clinical Features of Dengue Fever in Pakistan From 2003-2007: A Retrospective Cross-Sectional StudyDocument8 pagesDemographic and Clinical Features of Dengue Fever in Pakistan From 2003-2007: A Retrospective Cross-Sectional Studyann_michelle7No ratings yet
- Aubron Et Al. 2014 Infecções UrináriasDocument10 pagesAubron Et Al. 2014 Infecções UrináriasLeandro FigueiraNo ratings yet
- Ohnishi 2021Document5 pagesOhnishi 2021As MaaNo ratings yet
- Nejmoa 2002032Document13 pagesNejmoa 2002032Juan Antonio LópezNo ratings yet
- HIV Epidemic in ChinaDocument9 pagesHIV Epidemic in ChinaIsabella Rodríguez VelázquezNo ratings yet
- Paratyphi A Rates, Asia: SalmonellaDocument3 pagesParatyphi A Rates, Asia: SalmonellaYos SudarsoNo ratings yet
- Health-Care Workers' Occupational Exposures To Body Fluids in 21 Countries in Africa: Systematic Review and Meta-AnalysisDocument17 pagesHealth-Care Workers' Occupational Exposures To Body Fluids in 21 Countries in Africa: Systematic Review and Meta-AnalysisgusdeNo ratings yet
- International Journal of Infectious DiseasesDocument5 pagesInternational Journal of Infectious Diseaseslaksono_adeNo ratings yet
- Surveillance of Healthcare-Associated Infections in Indonesian HospitalsDocument12 pagesSurveillance of Healthcare-Associated Infections in Indonesian HospitalsRidha MardiyaniNo ratings yet
- 19 Ninan EtalDocument6 pages19 Ninan EtaleditorijmrhsNo ratings yet
- Prevalensi Gout Tibet ChinaDocument5 pagesPrevalensi Gout Tibet ChinaShared LifeNo ratings yet
- 718-1519-1-SM 2Document6 pages718-1519-1-SM 2NicoleNo ratings yet
- Update: Cholera Outbreak - Haiti, 2010: Morbidity and Mortality Weekly ReportDocument36 pagesUpdate: Cholera Outbreak - Haiti, 2010: Morbidity and Mortality Weekly Reportdougmcvay420No ratings yet
- ReferensiDocument243 pagesReferensiyasminNo ratings yet
- WAO Journal: Pei-Ying Lin, Chun-Hui Chu, Fang-Yu Chang, Ya-Wen Huang, Hui-Ju Tsai, Tsung-Chieh YaoDocument10 pagesWAO Journal: Pei-Ying Lin, Chun-Hui Chu, Fang-Yu Chang, Ya-Wen Huang, Hui-Ju Tsai, Tsung-Chieh YaoSiti Arum WidiyantiNo ratings yet
- Telehealth in Urology: A Systematic Review of The Literature. How Much Can Telemedicine Be Useful During and After The COVID-19 Pandemic?Document26 pagesTelehealth in Urology: A Systematic Review of The Literature. How Much Can Telemedicine Be Useful During and After The COVID-19 Pandemic?bintag mahaputraNo ratings yet
- Jalalpur Jattan Case StudyDocument8 pagesJalalpur Jattan Case Studyduracell19No ratings yet
- Urinary GuidelinesDocument9 pagesUrinary GuidelinesCabinet VeterinarNo ratings yet
- Guidance for COVID-19: Prevention, Control, Diagnosis and ManagementFrom EverandGuidance for COVID-19: Prevention, Control, Diagnosis and ManagementNo ratings yet
- Pristian Class X-4 22Document1 pagePristian Class X-4 22aura009No ratings yet
- Tugas ArtikelDocument4 pagesTugas Artikelaura009No ratings yet
- Tab Grup Clipboard Icon: Rivaldi Krisna Wijaya VIII E/35Document1 pageTab Grup Clipboard Icon: Rivaldi Krisna Wijaya VIII E/35aura009No ratings yet
- Questions:: V (4i + (2t + 2 1/3) J) M SDocument2 pagesQuestions:: V (4i + (2t + 2 1/3) J) M Saura009No ratings yet
- Mortality in Typhoid Intestinal Perforation-A Declining TrendDocument3 pagesMortality in Typhoid Intestinal Perforation-A Declining Trendaura009No ratings yet
- 2014 - SMFM - Society For Maternal-Fetal Medicine (SMFM) Special Report, The Maternal-Fetal Medicine Subspecialists' Role Within A Health Care SystemDocument10 pages2014 - SMFM - Society For Maternal-Fetal Medicine (SMFM) Special Report, The Maternal-Fetal Medicine Subspecialists' Role Within A Health Care SystemjrNo ratings yet
- BisinosisDocument4 pagesBisinosisMaría IgnaciaNo ratings yet
- Rehab Grand Rounds: Comprehensive Approach To The Management of Scapular Dyskinesia in The Overhead Throwing AthleteDocument8 pagesRehab Grand Rounds: Comprehensive Approach To The Management of Scapular Dyskinesia in The Overhead Throwing AthletekotraeNo ratings yet
- Tea Research PDFDocument3 pagesTea Research PDFStefan BugaleteNo ratings yet
- Doctor Su-Kabtas Family PracticeDocument6 pagesDoctor Su-Kabtas Family PracticeSrood TalibNo ratings yet
- Ophthalmology Referral Guidelines: Document IDDocument28 pagesOphthalmology Referral Guidelines: Document IDBambang AdiNo ratings yet
- Laboratory Activity 3 - HIS Lab - Classification of Health Care FacilitiesDocument5 pagesLaboratory Activity 3 - HIS Lab - Classification of Health Care FacilitiesCaissa Andrea Beatrice BaylenNo ratings yet
- Hallux Valgus SXDocument569 pagesHallux Valgus SXandi100% (2)
- Maha Iec - ppt2Document23 pagesMaha Iec - ppt2Ajay IyerNo ratings yet
- Product ListDocument2 pagesProduct Listpreeti dNo ratings yet
- BDS-Batch 11-Module 1 - CA - Anatomy Question BankDocument2 pagesBDS-Batch 11-Module 1 - CA - Anatomy Question BankcheckmateNo ratings yet
- Danh Mục Sách Điện Tử: Trường Đại Học Y DượC Huế T.T Thông Tin Thư ViệnDocument8 pagesDanh Mục Sách Điện Tử: Trường Đại Học Y DượC Huế T.T Thông Tin Thư ViệnLinh TinhNo ratings yet
- Evaluating The Neurologic Status of Unconscious PatientDocument3 pagesEvaluating The Neurologic Status of Unconscious Patientsambel_88No ratings yet
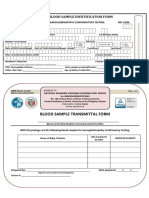
- HEM-FO-01&02, Rev.02 - ID FormsDocument1 pageHEM-FO-01&02, Rev.02 - ID FormsHazelle karren ManabatNo ratings yet
- Resume: Nivetha RavichandranDocument3 pagesResume: Nivetha Ravichandran777No ratings yet
- Clinic Schedule - October 2019Document3 pagesClinic Schedule - October 2019Syed Mohammad UsmanNo ratings yet
- ATLS 9th Edition Compendium For Update FinalDocument6 pagesATLS 9th Edition Compendium For Update FinalJorge BustosNo ratings yet
- SSCDocument50 pagesSSCMustafa Tambawala100% (1)
- Ppod Guide PrediabetesDocument5 pagesPpod Guide PrediabetesMahe ZabinNo ratings yet
- Higado 1Document86 pagesHigado 1Carlos CuadrosNo ratings yet