You might also like
- Protocol - IM DyspneaDocument7 pagesProtocol - IM DyspneaTrisNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Novena to St Pio for HealingDocument5 pagesNovena to St Pio for HealingelijahmariaNo ratings yet
- COPD Differential Diagnosis ModuleDocument44 pagesCOPD Differential Diagnosis ModulenicusoorNo ratings yet
- Gyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesDocument8 pagesGyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesVon HippoNo ratings yet
- HerniaDocument5 pagesHerniasarguss14100% (5)
- Polycystic Kidney DiseaseDocument9 pagesPolycystic Kidney DiseaseCésar Aguilar ContrerasNo ratings yet
- Vasculitis MindnodeDocument1 pageVasculitis MindnodeToño VargasNo ratings yet
- Clinical Reasoning On Doc Faculty Dev Tuesday VersionDocument76 pagesClinical Reasoning On Doc Faculty Dev Tuesday VersionMutiah FadilahNo ratings yet
- Preventive Pediatrics Part 1Document6 pagesPreventive Pediatrics Part 1mkct111No ratings yet
- GI BLEED - Medicine - Internal MedicineDocument11 pagesGI BLEED - Medicine - Internal Medicinezezma GamingNo ratings yet
- Lupus Case PresentationDocument48 pagesLupus Case PresentationRoscelie KhoNo ratings yet
- Lec 2 - Blood VesselsDocument12 pagesLec 2 - Blood VesselsJeffrey LübbertNo ratings yet
- (Pedia 3A) NEPHRO COMPILED PDFDocument40 pages(Pedia 3A) NEPHRO COMPILED PDFNoreenNo ratings yet
- Differential Diagnosis Fever With RashDocument15 pagesDifferential Diagnosis Fever With RashJeetat OngNo ratings yet
- Q: Describe The Diagnostic Criteria & Lab Investigation of SLE. AnsDocument28 pagesQ: Describe The Diagnostic Criteria & Lab Investigation of SLE. AnsSajib Nakib100% (1)
- AIR DROP EXAMنسختي PDFDocument35 pagesAIR DROP EXAMنسختي PDFYara AlmouallemNo ratings yet
- Hem-Onc: AnswerDocument3 pagesHem-Onc: AnswerAman Raj KNo ratings yet
- History Physical FormatDocument3 pagesHistory Physical FormatfilchibuffNo ratings yet
- MCQ 1. Heart Sound Heart Sound S1 S2Document7 pagesMCQ 1. Heart Sound Heart Sound S1 S2Atirah AaNo ratings yet
- Isabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderDocument15 pagesIsabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderCharlz ZipaganNo ratings yet
- Scoring System and Algorithm For Chronic RhinosinusitisDocument10 pagesScoring System and Algorithm For Chronic RhinosinusitispicassowaffleNo ratings yet
- Disorders of Sex Development (DSD) DevelopmentDocument40 pagesDisorders of Sex Development (DSD) DevelopmentAndi AdityaNo ratings yet
- Types of Arthritis: SOLOMON SALLFORSDocument3 pagesTypes of Arthritis: SOLOMON SALLFORSSolomon Seth SallforsNo ratings yet
- Case Mannequin Body InteractDocument5 pagesCase Mannequin Body InteractAVITA TRISTA NINGRUM100% (1)
- Cellulitis Oral Case PresDocument48 pagesCellulitis Oral Case PresLet BorlagdanNo ratings yet
- Cranial Fossa Notes - HelpfulDocument4 pagesCranial Fossa Notes - HelpfulKo HakuNo ratings yet
- Legal Medicine Review PDFDocument10 pagesLegal Medicine Review PDFGhie TangonanNo ratings yet
- Oral Cases Study Guide - PediatricsDocument68 pagesOral Cases Study Guide - PediatricsJohn100% (1)
- OBSTETRIC FORMDocument4 pagesOBSTETRIC FORMKhylamarie VillalunaNo ratings yet
- PATHO 4-3 Diseases of The EsophagusDocument7 pagesPATHO 4-3 Diseases of The EsophagusMiguel Cuevas DolotNo ratings yet
- Pediatrics:: History Taking and Physical Examination of AdolescentsDocument14 pagesPediatrics:: History Taking and Physical Examination of AdolescentsJüdith Marie Reyes BauntoNo ratings yet
- Harrison-Principals of Internal Medicine 20th. Ed. Prt.7-11Document707 pagesHarrison-Principals of Internal Medicine 20th. Ed. Prt.7-11Choi DongYiNo ratings yet
- IM-Module B Summarized Notes (IBD)Document69 pagesIM-Module B Summarized Notes (IBD)DeepbluexNo ratings yet
- Small Group DiscussionDocument3 pagesSmall Group DiscussionBea SamonteNo ratings yet
- Internal Medicine Quick TablesDocument276 pagesInternal Medicine Quick Tablesjoey plouffeNo ratings yet
- Most Common Nelsons 16th EdDocument32 pagesMost Common Nelsons 16th EdRegine PanaliganNo ratings yet
- Medicine OSCE - Common Diseases Ver2Document4 pagesMedicine OSCE - Common Diseases Ver2TrisNo ratings yet
- Carbuncle, Incision, Drainage, DebridementDocument11 pagesCarbuncle, Incision, Drainage, DebridementAlvin Germo PasuquinNo ratings yet
- Outline For History TakingDocument2 pagesOutline For History TakingBlancheNo ratings yet
- M&M Hypovolemic ShockDocument30 pagesM&M Hypovolemic ShockRyan FornollesNo ratings yet
- Classification of The Epilepsies: Purpose: For Clinical DiagnosisDocument25 pagesClassification of The Epilepsies: Purpose: For Clinical Diagnosisayu rifqiNo ratings yet
- Gallbladder and Extrahepatic Biliary System - FinlDocument14 pagesGallbladder and Extrahepatic Biliary System - FinlJoevet T. TadlasNo ratings yet
- Acute Poststreptococcal GlomerulonephritisDocument69 pagesAcute Poststreptococcal GlomerulonephritisJirran CabatinganNo ratings yet
- Rhino SinusitisDocument57 pagesRhino SinusitisArif MohammedNo ratings yet
- IM 3A PE Cardiology Dr. JumangitDocument12 pagesIM 3A PE Cardiology Dr. JumangitCzara DyNo ratings yet
- Cerebral PalsyDocument14 pagesCerebral PalsyWaode SittrisnawatiNo ratings yet
- Neurology in TableDocument93 pagesNeurology in TableHassan Bani SaeidNo ratings yet
- FundosDocument2 pagesFundosfarorangeNo ratings yet
- Common Ent EmergenciesDocument65 pagesCommon Ent EmergenciesferaNo ratings yet
- GynexDocument73 pagesGynexDominque RabastoNo ratings yet
- Review Slides OphthaDocument14 pagesReview Slides OphthaSUSHMITA MAE ROSE CONTRERASNo ratings yet
- Physical Diagnosis Information OverviewDocument119 pagesPhysical Diagnosis Information OverviewNarcis PopaNo ratings yet
- Mediastinum and Its ContentsDocument11 pagesMediastinum and Its ContentsPap YeeNo ratings yet
- Review Lectures Forlu6: Basic Eye Exam Common Opd Complaints Common Er Cases PharmacologyDocument110 pagesReview Lectures Forlu6: Basic Eye Exam Common Opd Complaints Common Er Cases Pharmacologyupmed2012block9No ratings yet
- Prenatal Assessment GuideDocument17 pagesPrenatal Assessment GuideCyndryl SampotonNo ratings yet
- Hypertension Management GuideDocument8 pagesHypertension Management GuideSugimoto Karla Erika100% (1)
- Approach To The Patient With Rheumatic DiseaseDocument11 pagesApproach To The Patient With Rheumatic DiseasetedplushNo ratings yet
- HNLDocument10 pagesHNLRhaffy Bearneza RapaconNo ratings yet
- ImmunizationDocument32 pagesImmunizationRhaffy Bearneza RapaconNo ratings yet
- This Will Aid in Identifying The Esophagus.: Cervical Esophagostomy Operative StepsDocument1 pageThis Will Aid in Identifying The Esophagus.: Cervical Esophagostomy Operative StepsRhaffy Bearneza RapaconNo ratings yet
- Benign Febrile SeizureDocument15 pagesBenign Febrile SeizureRhaffy Bearneza RapaconNo ratings yet
- Daily CensusDocument2 pagesDaily CensusRhaffy Bearneza RapaconNo ratings yet
- Physical Examination of The KneeDocument52 pagesPhysical Examination of The KneeRhaffy Bearneza RapaconNo ratings yet
- Didactics With The Consultant - BreechDocument68 pagesDidactics With The Consultant - BreechRhaffy Bearneza RapaconNo ratings yet
- Repeat C-Section DeliveryDocument1 pageRepeat C-Section DeliveryRhaffy Bearneza RapaconNo ratings yet
- Anaesthesia For Medical StudentDocument266 pagesAnaesthesia For Medical Studentprevet100% (4)
- Therapeutic Flow SheetDocument2 pagesTherapeutic Flow SheetRhaffy Bearneza RapaconNo ratings yet
- General Data: G.E.L. Male 3 Yo Roman Catholic Brgy. Dungon C. Mandurrio Iloilo CityDocument75 pagesGeneral Data: G.E.L. Male 3 Yo Roman Catholic Brgy. Dungon C. Mandurrio Iloilo CityRhaffy Bearneza RapaconNo ratings yet
- AssignmentDocument1 pageAssignmentRhaffy Bearneza RapaconNo ratings yet
- Rhaffy BDocument3 pagesRhaffy BRhaffy Bearneza RapaconNo ratings yet
- Physical Examination of The Foot and AnkleDocument42 pagesPhysical Examination of The Foot and AnkleRhaffy Bearneza RapaconNo ratings yet
- MunchausenDocument2 pagesMunchausenRhaffy Bearneza RapaconNo ratings yet
- LabDocument4 pagesLabRhaffy Bearneza RapaconNo ratings yet
- Presentation 1Document24 pagesPresentation 1Rhaffy Bearneza RapaconNo ratings yet
- Presentations TipsDocument21 pagesPresentations Tipsapi-253601657No ratings yet
- CPC Case Study NoDocument15 pagesCPC Case Study NoRhaffy Bearneza RapaconNo ratings yet
- Perception Towards Smoking of Intermediate Pupils of SelectedDocument2 pagesPerception Towards Smoking of Intermediate Pupils of SelectedRhaffy Bearneza RapaconNo ratings yet
- Renal Failure 111111Document2 pagesRenal Failure 111111Rhaffy Bearneza RapaconNo ratings yet
- Autolytic or Autodigestive Changes After DeathDocument10 pagesAutolytic or Autodigestive Changes After DeathRhaffy Bearneza Rapacon100% (1)
- Herpes Simplex VirusDocument26 pagesHerpes Simplex VirusRhaffy Bearneza RapaconNo ratings yet
- FinalDocument4 pagesFinalRhaffy Bearneza RapaconNo ratings yet
- Herpes Simplex VirusDocument26 pagesHerpes Simplex VirusRhaffy Bearneza RapaconNo ratings yet
- Final Power PointDocument46 pagesFinal Power PointRhaffy Bearneza RapaconNo ratings yet
- CPC FinalsDocument2 pagesCPC FinalsRhaffy Bearneza RapaconNo ratings yet
- Clinico Pathological ConferenceDocument18 pagesClinico Pathological ConferenceRhaffy Bearneza RapaconNo ratings yet
- Interpersonal PowerDocument5 pagesInterpersonal PowerRhaffy Bearneza RapaconNo ratings yet
- Parts of ShipDocument6 pagesParts of ShipJaime RodriguesNo ratings yet
- JY Series Single-Phase Capacitor Induction MotorsDocument1 pageJY Series Single-Phase Capacitor Induction MotorsAditya PrasetyoNo ratings yet
- Clean Milk ProductionDocument19 pagesClean Milk ProductionMohammad Ashraf Paul100% (3)
- Effect of Some Algal Filtrates and Chemical Inducers On Root-Rot Incidence of Faba BeanDocument7 pagesEffect of Some Algal Filtrates and Chemical Inducers On Root-Rot Incidence of Faba BeanJuniper PublishersNo ratings yet
- Young Women's Sexuality in Perrault and CarterDocument4 pagesYoung Women's Sexuality in Perrault and CarterOuki MilestoneNo ratings yet
- A Compilation of Thread Size InformationDocument9 pagesA Compilation of Thread Size Informationdim059100% (2)
- Garlic Benefits - Can Garlic Lower Your Cholesterol?Document4 pagesGarlic Benefits - Can Garlic Lower Your Cholesterol?Jipson VargheseNo ratings yet
- Crew Served WeaponsDocument11 pagesCrew Served WeaponsKyle Fagin100% (1)
- Cyclograph User ManualDocument15 pagesCyclograph User ManualPeter BateNo ratings yet
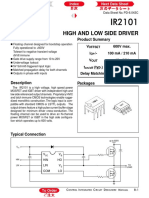
- Datasheet PDFDocument6 pagesDatasheet PDFAhmed ElShoraNo ratings yet
- Chap 2 Debussy - LifejacketsDocument7 pagesChap 2 Debussy - LifejacketsMc LiviuNo ratings yet
- Abdomen - FRCEM SuccessDocument275 pagesAbdomen - FRCEM SuccessAbin ThomasNo ratings yet
- Clausius TheoremDocument3 pagesClausius TheoremNitish KumarNo ratings yet
- CAE The Most Comprehensive and Easy-To-Use Ultrasound SimulatorDocument2 pagesCAE The Most Comprehensive and Easy-To-Use Ultrasound Simulatorjfrías_2No ratings yet
- Peptic Ulcer Disease: Causes, Symptoms and TreatmentDocument24 pagesPeptic Ulcer Disease: Causes, Symptoms and TreatmentOktaviana Sari Dewi100% (1)
- Railway Airport Docks and HarbourDocument21 pagesRailway Airport Docks and HarbourvalarmathibalanNo ratings yet
- Chap06 (6 24 06)Document74 pagesChap06 (6 24 06)pumba1234No ratings yet
- APLICACIONES PARA AUTOS Y CARGA LIVIANADocument50 pagesAPLICACIONES PARA AUTOS Y CARGA LIVIANApancho50% (2)
- KAC-8102D/8152D KAC-9102D/9152D: Service ManualDocument18 pagesKAC-8102D/8152D KAC-9102D/9152D: Service ManualGamerAnddsNo ratings yet
- Essentials For Professionals: Road Surveys Using SmartphonesDocument25 pagesEssentials For Professionals: Road Surveys Using SmartphonesDoly ManurungNo ratings yet
- Stability Calculation of Embedded Bolts For Drop Arm Arrangement For ACC Location Inside TunnelDocument7 pagesStability Calculation of Embedded Bolts For Drop Arm Arrangement For ACC Location Inside TunnelSamwailNo ratings yet
- Product ListDocument4 pagesProduct ListyuvashreeNo ratings yet
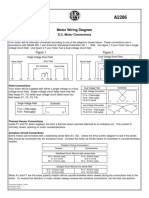
- Motor Wiring Diagram: D.C. Motor ConnectionsDocument1 pageMotor Wiring Diagram: D.C. Motor Connectionsczds6594No ratings yet
- Rectifiers and FiltersDocument68 pagesRectifiers and FiltersMeheli HalderNo ratings yet
- g4 - Stress Analysis of Operating Gas Pipeline Installed by HorizontalDocument144 pagesg4 - Stress Analysis of Operating Gas Pipeline Installed by HorizontalDevin DickenNo ratings yet
- 中美两国药典药品分析方法和方法验证Document72 pages中美两国药典药品分析方法和方法验证JasonNo ratings yet
- Who will buy electric vehicles Segmenting the young Indian buyers using cluster analysisDocument12 pagesWho will buy electric vehicles Segmenting the young Indian buyers using cluster analysisbhasker sharmaNo ratings yet
- 2 - Elements of Interior DesignDocument4 pages2 - Elements of Interior DesignYathaarth RastogiNo ratings yet
- The Templist Scroll by :dr. Lawiy-Zodok (C) (R) TMDocument144 pagesThe Templist Scroll by :dr. Lawiy-Zodok (C) (R) TM:Lawiy-Zodok:Shamu:-El100% (5)
- CG Module 1 NotesDocument64 pagesCG Module 1 Notesmanjot singhNo ratings yet