You might also like
- NSTP - HealthDocument38 pagesNSTP - Healthmftaganas86% (7)
- TFN RVWDocument145 pagesTFN RVWmftaganasNo ratings yet
- Routes of Drug AdministrationDocument24 pagesRoutes of Drug Administrationmftaganas100% (1)
- NCM 100-Nursing ProcessDocument117 pagesNCM 100-Nursing ProcessmftaganasNo ratings yet
- Introduction To Sociology and AnthropologyDocument10 pagesIntroduction To Sociology and AnthropologymftaganasNo ratings yet
- Immediate Newborn Care (Autosaved)Document183 pagesImmediate Newborn Care (Autosaved)mftaganasNo ratings yet
- Faye GDocument34 pagesFaye GmftaganasNo ratings yet
- Flower ArrangementDocument20 pagesFlower Arrangementmftaganas86% (7)
- Topical MedicationsDocument24 pagesTopical MedicationsmftaganasNo ratings yet
- Admission of PatientsDocument4 pagesAdmission of Patientsmftaganas100% (2)
- Cast CareDocument47 pagesCast CaremftaganasNo ratings yet
- Competency Appraisal ExamDocument5 pagesCompetency Appraisal Exammftaganas100% (1)
- Measuring Intake and OutputDocument24 pagesMeasuring Intake and Outputmftaganas83% (6)
- NCPDocument7 pagesNCPmftaganasNo ratings yet
- NCPDocument7 pagesNCPmftaganasNo ratings yet
- Care of Patients With TractionDocument25 pagesCare of Patients With Tractionmftaganas100% (1)
- ENEMADocument37 pagesENEMAmftaganas100% (3)
- 77 Teen PregnancyDocument20 pages77 Teen PregnancymftaganasNo ratings yet
- Brand Name: Amethopterin Classification: Anti-Neoplastic Mechanism of Action: Indication: Side Effects: Nsg. ConsiderationsDocument4 pagesBrand Name: Amethopterin Classification: Anti-Neoplastic Mechanism of Action: Indication: Side Effects: Nsg. ConsiderationsmftaganasNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- ECG Fast and Easy chp12 PDFDocument40 pagesECG Fast and Easy chp12 PDFkikyfauziaNo ratings yet
- Artificial HeartDocument17 pagesArtificial HeartRAKESHKANNAN100% (1)
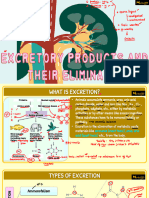
- Vipin Sir Biology 19. Excretory Products and Their EliminationDocument55 pagesVipin Sir Biology 19. Excretory Products and Their EliminationvanshpatelssisNo ratings yet
- Physiology and Neurobiliogy 2275 UCONN Test 3Document8 pagesPhysiology and Neurobiliogy 2275 UCONN Test 3sin117No ratings yet
- NHV Tripsy Supplement For Pets 100mlDocument1 pageNHV Tripsy Supplement For Pets 100mljjes86No ratings yet
- Tumors and Cancers Endocrine Glands - Blood - Marrow - LymphDocument231 pagesTumors and Cancers Endocrine Glands - Blood - Marrow - LymphAndré Jason MendesNo ratings yet
- Hormones & Hormones AntagonistsDocument27 pagesHormones & Hormones AntagonistsVarsha Shende KhobragadeNo ratings yet
- Procedure 1 Brest Examination Self ExaminationDocument4 pagesProcedure 1 Brest Examination Self ExaminationPriyanka SheoranNo ratings yet
- Funda SL FinalsDocument3 pagesFunda SL FinalsKarylle Joy ValenciaNo ratings yet
- Female RTOG Normal Pelvis Atlas PDFDocument129 pagesFemale RTOG Normal Pelvis Atlas PDFsusdoctor100% (1)
- Hyperprolactinemia, Galactorrhea, and Pituitary AdenomasDocument14 pagesHyperprolactinemia, Galactorrhea, and Pituitary AdenomasSumiya JssalbNo ratings yet
- Cardiac Cycle by Dr. RoomiDocument71 pagesCardiac Cycle by Dr. RoomiMudassar Roomi100% (3)
- Second Year Anatomy Guidelines - AIMC ACADEMIADocument29 pagesSecond Year Anatomy Guidelines - AIMC ACADEMIAMazen KhalidNo ratings yet
- Qt.2 Summative Test 1 & 2Document5 pagesQt.2 Summative Test 1 & 2Susan Salvador100% (1)
- Class AgnathaDocument5 pagesClass AgnathaJackie Swift Funtanilla100% (1)
- Echo 20190914164646458Document2 pagesEcho 20190914164646458Gigi DajoyagNo ratings yet
- 11 Lung PathologyDocument7 pages11 Lung PathologycarlgangcaNo ratings yet
- Endocrine AgentsDocument10 pagesEndocrine AgentsWendy VasquezNo ratings yet
- Sistem Pertahanan Tubuh: DidapatDocument54 pagesSistem Pertahanan Tubuh: DidapatNur JaziLahNo ratings yet
- Chapter 13 Nervous System in Mammals - Lecture NotesDocument6 pagesChapter 13 Nervous System in Mammals - Lecture Notesapi-3728508100% (4)
- Master Radiology Notes UrologyDocument106 pagesMaster Radiology Notes UrologySafwan ShaikhNo ratings yet
- Renal PhysiologyDocument5 pagesRenal PhysiologyJayricDepalobosNo ratings yet
- Atrial Septal DefectDocument7 pagesAtrial Septal DefectRose WidantiNo ratings yet
- Complete Eloptic Directory (OCR) PDFDocument308 pagesComplete Eloptic Directory (OCR) PDFAnonymous SCZ4uYNo ratings yet
- Histology of AppendixDocument1 pageHistology of Appendixalyson_l100% (1)
- Health Policy Advisory Committee On TechnologyDocument76 pagesHealth Policy Advisory Committee On TechnologyTài NguyễnNo ratings yet
- Alcoholic Liver DiseaseDocument22 pagesAlcoholic Liver DiseaseRaju NiraulaNo ratings yet
- Nervous System WebquestDocument3 pagesNervous System Webquestsilrub8015No ratings yet
- HCS 3rd YearDocument44 pagesHCS 3rd YearDafny CzarinaNo ratings yet
- Breast AugmentationDocument7 pagesBreast AugmentationnikitagustiNo ratings yet